Novel Characteristics of Race-Specific Genetic Functions in Korean CADASIL


1
Department of Neurology, Kangdong Sacred Heart Hospital, College of Medicine, Hallym University, Seoul 05355, Korea
2
The Korean Cerebrovascular Research Institute, Seoul 03100, RKorea
3
Department of Neurology, Seoul National University Hospital, Seoul 03080, Korea
*
Authors to whom correspondence should be addressed.
†
Both authors contributed equally to this work.
Medicina 2019, 55(9), 521; https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090521
Submission received: 14 June 2019
/
Revised: 19 August 2019
/
Accepted: 21 August 2019
/
Published: 22 August 2019
(This article belongs to the Special Issue Restorative Neurology: From Bench to Bedside and Vice Versa. Advances and Challenges)
Abstract
:Background and Objectives: Previous studies found differences in the characteristics of NOTCH3 mutations in Caucasians and Asians with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). Therefore, we sought to investigate the correlations between genetic and clinical/radiological findings in Korean CADASIL patients including some variants of unknown significance (VUS). Materials and Methods: We screened 198 patients with a suspected diagnosis of CADASIL between 2005 and 2015 via Sanger sequencing. Results: A total of 34 subjects (52.5 ± 9.5 years) were included. The majority of the mutations were in exon 3 and exon 11. R75P mutations (n = 5), followed by Y465C and R544C mutations (n = 4) were the most prevalent. Patients with those mutations exhibited less frequent anterior temporal (AT) or external capsular (EC) hyperintensities compared to patients with other locus mutations. Hemorrhagic stroke (HS) was found to be associated with mutations in exon 3 (R75P), exon 9 (Y465C), exon 11 (R587C), and exon 22 (R1175W variants), which were common locations in our study. Although it is unclear that genetic differences might affect the phenotypes in ethnicities, Asian population shows less migraine or seizure, but more intracerebral hemorrhage. Unlike in westernized countries, typical AT or EC hyperintensities may not be significant MRI markers, at least in Korean CADASIL patients. Furthermore, similar to R75P phenotypes, it is a novel finding that patients with Y465C and R1175W VUS have less frequent AT involvement than Caucasians. Conclusion: The associations between HS and common genetic locations account for the increased development of intracerebral hemorrhage in Koreans rather than Caucasians. We suggest that some CADASIL mutations appear to impart novel region-specific characteristics.
1. Introduction
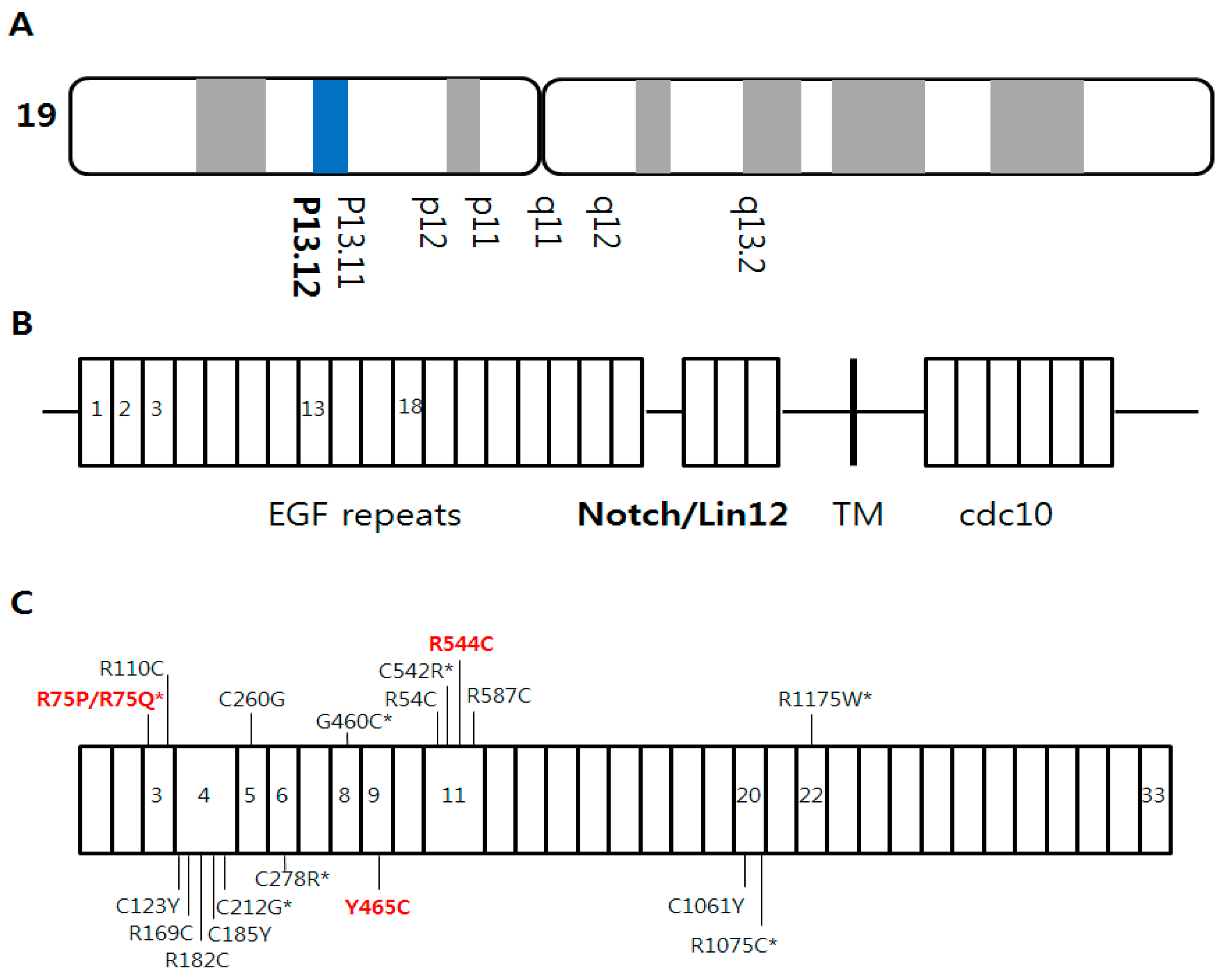
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a rare hereditary disease caused by mutations in the NOTCH3 gene, which encodes for the first five epidermal growth factor repeats on chromosome 19p13.12 (Figure 1A,B). CADASIL is characterized by severe white matter changes (WMCs), especially in the anterior temporal (AT) and external capsule (EC) lesions. The main clinical symptoms are recurrent ischemic stroke (IS), migraine, and progressive dementia [1].
While the majority of NOTCH3 gene mutations were found in exon 4 in Caucasians [2,3] and in Chinese mainland [4], those were in exon 11 in Han Chinese in Taiwan [5] and in Koreans [6,7]. In contrast to westernized countries, an infrequent involvement of AT hyperintensities on T2-weighted magnetic resonance imaging (MRI) was also observed in Asian studies [5,8].
Although the underlying genetic mechanisms remain unclear, a specific gene has unique roles, and so changes in amino acids via gene mutations may provoke alterations that lead to region-specific functional deficits. Therefore, we sought to investigate the correlations between genetic and clinical/radiological findings in Korean CADASIL patients including some variants of unknown significance (VUS).
2. Materials and Methods
We screened 198 consecutive patients with a suspected diagnosis of CADASIL between 2005 and 2015 at Seoul National University Hospital (SNUH). Genetic work-ups were performed based on the physicians’ discretion considering the previous medical history, neurological examination, and MRI findings. The inclusion criteria were severe white matter hyperintensities on the brain MRI and at least one of the following: recurrent subcortical infarction at relatively young age, cognitive impairment, psychiatric symptoms, migraine, seizure, and family history of strokes. Patients with definite etiologies of large artery stenosis or cardioembolism for index stroke lesions were excluded. Among them, 34 patients were diagnosed as having known NOTCH3 mutations (n = 23) or novel VUS (n = 11).
Mutational hotspots of the NOTCH3 gene in exons 2–23 were screened via Sanger sequencing. Genomic deoxyribonucleic acid (DNA) was extracted from peripheral blood. The polymerase chain reaction sequences were compared with the previously published NOTCH3 DNA sequences. To identify the likely significance of known NOTCH3 DNA sequences or variants, we examined published literature, the “NOTCH3 gene homepage-Leiden Open Variation Database 3.0” (Leiden University Medical Center, Leiden, The Netherlands), and “Exome Aggregation Consortium database”.
1.5 Tesla or 3.0 Tesla MRI was performed in almost patients except two subjects. One was a daughter of a symptomatic patient. Since she did not have any clinical symptoms, she did not want to take brain image. Although another subject did not have MRI image, MRI results from other hospitals were available only on chart records. The WMCs and cerebral microbleeds (CMBs) were assessed with a scoring system by using modified Fazekas scales that was based on previous literatures [9]. We analyzed the AT and EC lesions, which are known to be useful markers for CADASIL. The institutional review board (Approval number: H-1504-064-664) approved this study protocol, and written informed consent was obtained from all participants.
3. Results
Among a total of 34 subjects, 11 known mutations (n = 23) and 8 VUS (n = 11) were identified. Ischemic stroke (IS) was the most common symptom (n = 15), and the other manifestations were HS (n = 6) and migraine (n = 8). Seizure was not detected in our study population. Hemorrhagic stroke (HS) was found to be associated with mutations in exon 3 (R75P), exon 9 (Y465C), exon 11 (R587C), and exon 22 (R1175W VUS) (see Table 1).
The majority of the mutations or VUS were in exon 3 and exon 11. R75P mutations (n = 5), followed by Y465C and R544C mutations (n = 4) were the most prevalent (Figure 1C and Figure S1). Although the enrolled patients were gathered from multiple areas, three of the four CADASIL patients with R544C mutation were born on Jeju Island.
Among the five subjects with R75P mutations or R75Q VUS, only one individual showed AT hyperintensities. In four patients with Y465C mutations, none had ischemic strokes. Among them, three patients are one family. Among the four subjects with R544C mutations, three patients did not have any strokes and did not show AT or EC hyperintensities (Table 1).
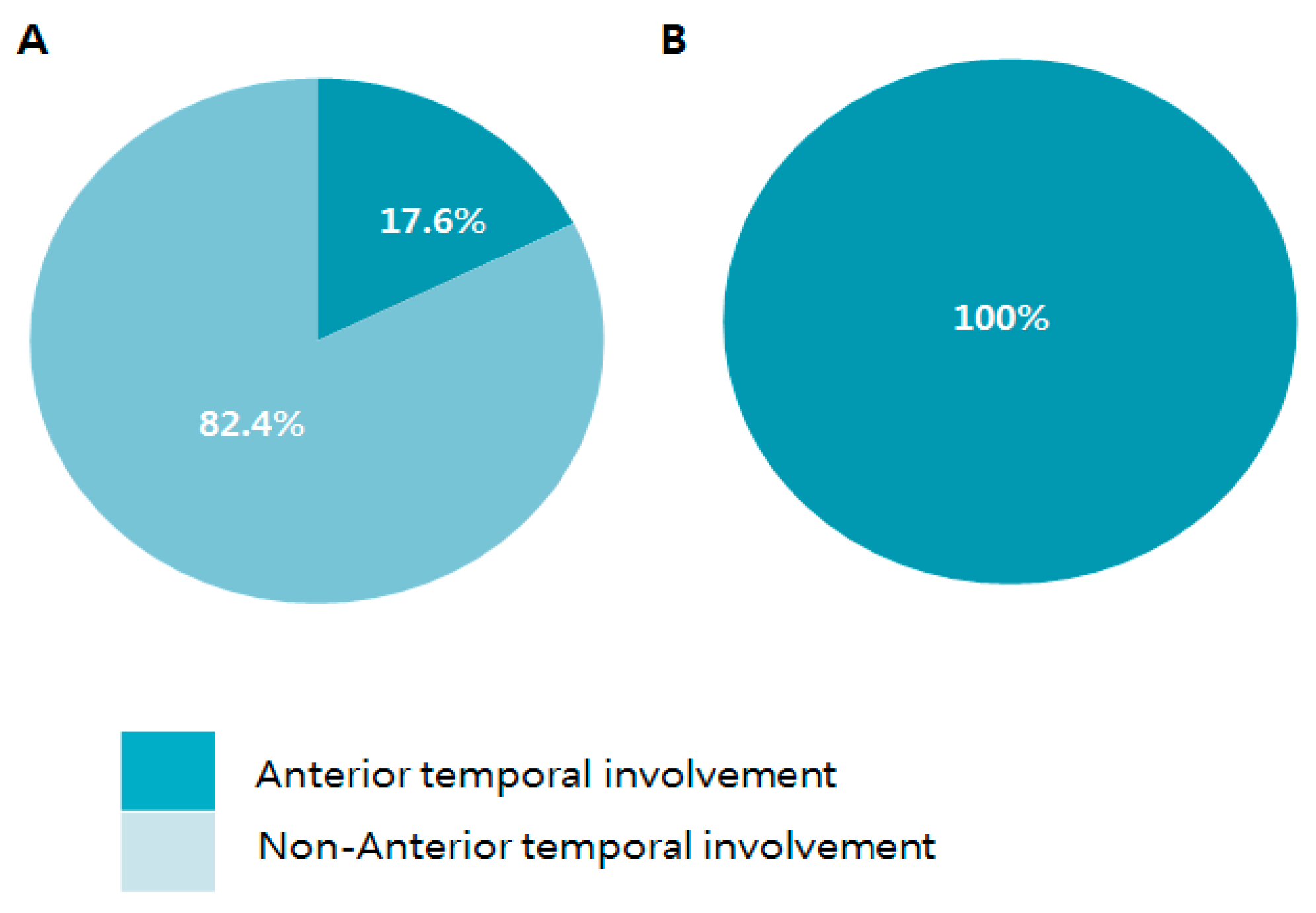
While all patients with mutations in exon 4 had AT lesions, approximately less than a third of patients with mutations in some mutational hotspots had AT lesions; R75P/R75Q VUS (16.7%), Y465C (0%), R544C (25%), and R1175W VUS (33.3%) (see Figure 2). As a result, compared to mutations in exon 4, the proportion of AT involvement in patients with the most prevalent loci was 17.6% (Figure 3A,B). Results with EC hyperintensities also showed similar distribution.
The genetic spectrum, clinical manifestations, and MRI findings of CADASIL in different articles were compared in Table 2.
4. Discussion
Unlike previous reports from western countries, our results demonstrated that the majority of mutations were in exon 11 followed by exon 3. The majority of mutations (R75P, Y465C, R544C, and R1175W VUS) were associated with less prevalent AT or EC hyperintensities. HS was found to be associated with R75P, Y465C, R587C mutations, and R1175W VUS, which were common loci in our study. These results suggest that the characteristics of NOTCH3 mutations in Koreans may be different from those in Caucasians.
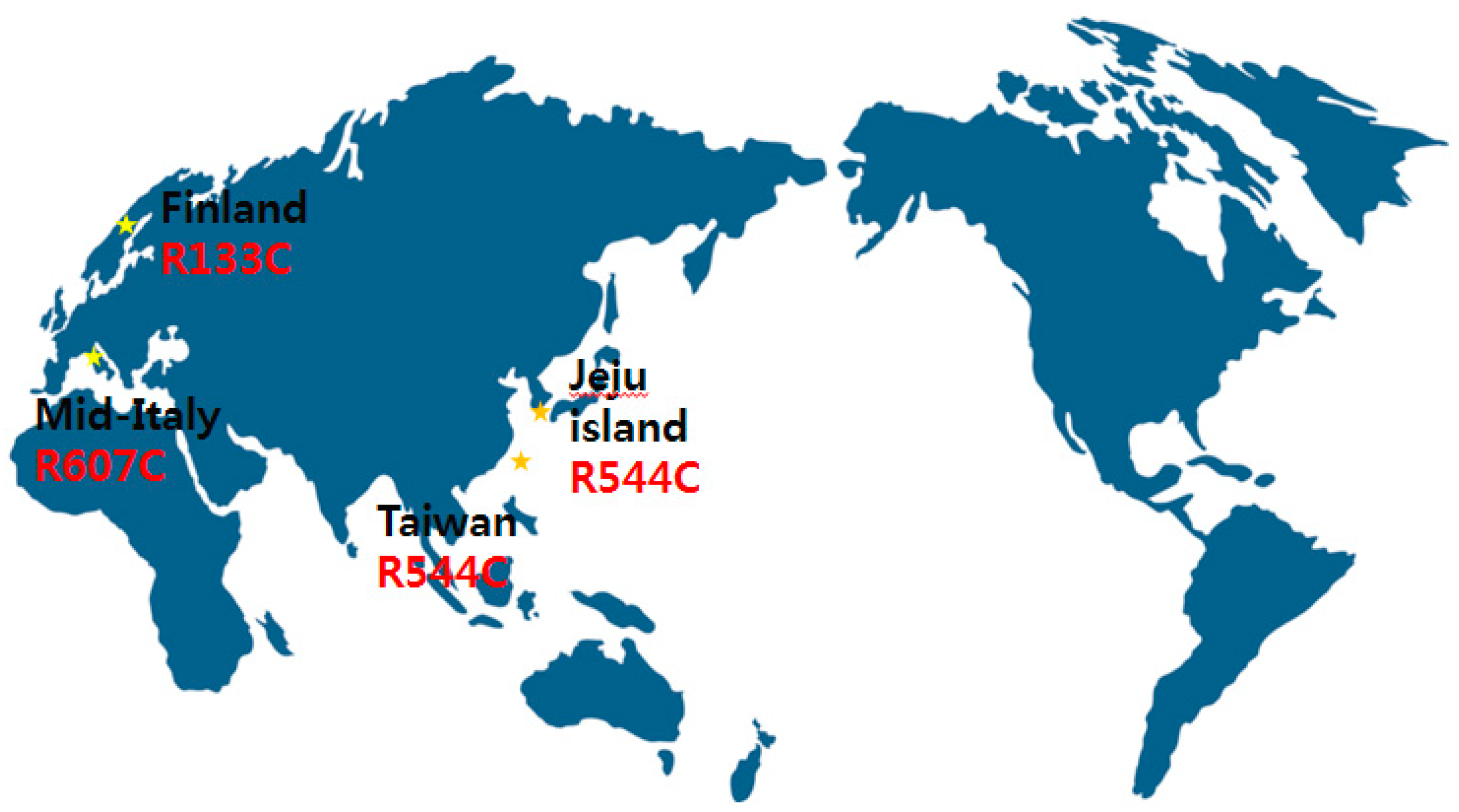
According to previous Caucasian articles, NOTCH3 mutations were frequently found in exons 2–6, especially in exon 4 [1,2,10,11]. In British cases, 73% of NOTCH3 mutations were in exon 4 [2]. However, in 20 subjects in 17 Korean CADASIL families on Jeju Island, 85% of NOTCH3 mutations were in exon 11 and R544C mutations were present in 75% of patients [7]. This predominance of the R544C mutation is quite interesting. Three of four CADASIL patients with the R544C mutation in exon 11 were born on Jeju Island, which suggests a ‘founder effect’. This founder has been reported in small, isolated islands or inlands such as Taiwan (R544C) [5], Finland (R133C) [3], and mid-Italy (R607C) [12] (Figure 4). There are some Taiwan studies that analyze stroke etiology and radiological findings focused on R544C mutations [13,14]. According to a prospective, multicenter study in Taiwan, small-vessel occlusion was significantly associated with R544C mutation [13]. Another Taiwan study demonstrated that of 67 patients with R544C mutations, patients with intracerebral hemorrhage (ICH) onset were more likely to have white matter hyperintensities and higher total cerebral MBs [14]. Despite a lot of controversy, R75P could be considered the best explained cystein sparing Notch3 mutation to date [6,8]. Furthermore, recent study demonstrated another cystein sparing Notch3 mutation (D80G) in four German families [15]. These findings are evaluated as having broadened insight in CADASIL.
There were no patients that presented with seizures, which is in accordance with previous literatures [5,6]. While approximately half of patients reported migraines in British (54.2%) [2] and American (40%) groups, migraine appeared to be less prevalent in Asians (Chinese, 4.8%; Korean, 10%) [5]. Most of the patients with R75P mutations/R75Q VUS (IS, n = 4; HS, n = 1) demonstrated strokes as clinical symptoms. Although the exact patho-mechanisms of intracerebral hemorrhage (ICH) in CADASIL patients are not fully elucidated yet, MBs and antithrombotics seem to be associated with the increased risk of ICH. Notably, HS was found to be associated with mutations in exon 3 (R75P), exon 9 (Y465C), exon 11 (R587C), and exon 22 (R1175W VUS), which were common locations in this study. Compared to those patients, none of the patients with NOTCH3 mutations in exon 4 had HS. These findings may account for the increased development of ICH in Korean individuals rather than Caucasians [6]. In this study, although the association between R544C and HS has not been proven, it is thought that the number of enrolled patients with R544C is too small.
AT and EC hyperintensities have been regarded as significant markers for Caucasian CADASIL patients, with a sensitivity of 89% [2]. However, this was not consistent with the results of an Asian study (42.9% in Chinese and only 20% in Korean) [5,7]. There were typical AT hyperintensities in only one of six subjects with R75P mutations/R75Q VUS and one of four patients with R544C mutations. Previous articles demonstrated that R75P mutations were associated with an infrequent involvement of AT lesions, thus widening the spectrum of CADASIL [6,8]. It is noteworthy that these types of NOTCH3 mutations occurred in the majority of Korean CADASIL patients. Therefore, we suggest that AT or EC lesions may not be significant MRI markers, at least in Korean CADASIL.
In addition, it is a novel finding of this study that patients with Y465C and R1175W VUS have low AT involvement. However, the number of patients included is too small to generalize this result.
Conventionally, cerebral WMCs have been indicated in microangiopathy-related cerebral damage and have shared patho-mechanisms with CMBs. However, there were no definite linear correlations between the number of CMBs and the Fazekas scales (Spearman’s r = 0.51). These observations suggest that WMCs in CADASIL patients result from a different pathophysiology than conventional small-vessel diseases. Because the AT pole has a unique rotatory structure and is vascularized by anterior temporal artery, AT hyperintensities are enlarged perivascular spaces that exhibit myelin degeneration and subsequent axonal disruption, and are not lacunar infarctions [11,16].
There are some caveats. First, because this was a small single-center study, our findings may not be applicable to other populations. Second, we conducted NOTCH3 genetic sequencing in patients with a suspected diagnosis of CADASIL or their relatives. Some asymptomatic CADASIL carriers may have been excluded. Third, this was a retrospective study. Since most patients were examined during the acute stroke period, cognitive evaluations were not sufficient. Finally, we may have missed or overestimated the significance of mutations or VUS. However, to evaluate mutations accurately, we searched both published articles and NOTCH3 gene databases.
5. Conclusions
In conclusion, unlike in westernized countries, typical AT or EC hyperintensities may not be significant MRI markers, at least in Korean CADASIL patients. The associations between HS and common locations in our study may account for the increased development of ICH in Korean individuals rather than Caucasians. Although the underlying genetic mechanisms remain unclear, we suggest that some CADASIL mutations appear to impart novel region-specific characteristics. To clarify the variable functional roles of NOTCH3 mutations, more cell expression studies may be needed.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/1648-9144/55/9/521/s1, Figure S1: Exon distributions in NOTCH3 gene mutations.
Author Contributions
S-H.L. devised the original study concept and design. Y.K. performed the data analysis. S.-H.L. made intellectual contribution. Y.K. wrote the manuscript. Both authors interpreted the results.
Funding
This research was funded by the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI) funded by the Ministry of Health & Welfare, Republic of Korea, grant number HI17C0076, and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT, grant number NRF-2018R1A2A2A05022369. This research was funded by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT, grant number NRF-2018R1C1B5086320.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chabriat, H.; Joutel, A.; Dichgans, M.; Tournier-Lasserve, E.; Bousser, M.G. Cadasil. Lancet. Neurol. 2009, 8, 643–653. [Google Scholar] [CrossRef]
- Markus, H.S.; Martin, R.J.; Simpson, M.A.; Dong, Y.B.; Ali, N.; Crosby, A.H.; Powell, J.F. Diagnostic strategies in CADASIL. Neurology 2002, 59, 1134–1138. [Google Scholar] [CrossRef] [PubMed]
- Mykkanen, K.; Savontaus, M.L.; Juvonen, V.; Sistonen, P.; Tuisku, S.; Tuominen, S.; Penttinen, M.; Lundkvist, J.; Viitanen, M.; Kalimo, H.; et al. Detection of the founder effect in Finnish CADASIL families. Eur. J. Hum. Genet. EJHG 2004, 12, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zuo, Y.; Sun, W.; Zhang, W.; Lv, H.; Huang, Y.; Xiao, J.; Yuan, Y.; Wang, Z. The genetic spectrum and the evaluation of CADASIL screening scale in Chinese patients with NOTCH3 mutations. J. Neurol. Sci. 2015, 354, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Liu, C.S.; Chang, M.H.; Lin, K.P.; Fuh, J.L.; Lu, Y.C.; Liu, Y.F.; Soong, B.W. Population-specific spectrum of NOTCH3 mutations, MRI features and founder effect of CADASIL in Chinese. J. Neurol. 2009, 256, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Choi, E.J.; Choi, C.G.; Kim, G.; Choi, J.H.; Yoo, H.W.; Kim, J.S. Characteristics of CADASIL in Korea: A novel cysteine-sparing Notch3 mutation. Neurology 2006, 66, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.C.; Kang, S.Y.; Kang, J.H.; Park, J.K. Intracerebral hemorrhages in CADASIL. Neurology 2006, 67, 2042–2044. [Google Scholar] [CrossRef] [PubMed]
- Ueda, A.; Ueda, M.; Nagatoshi, A.; Hirano, T.; Ito, T.; Arai, N.; Uyama, E.; Mori, K.; Nakamura, M.; Shinriki, S.; et al. Genotypic and phenotypic spectrum of CADASIL in Japan: The experience at a referral center in Kumamoto University from 1997 to 2014. J. Neurol. 2015, 262, 1828–1836. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Neuroradiol. 1987, 8, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Desmond, D.W.; Moroney, J.T.; Lynch, T.; Chan, S.; Chin, S.S.; Mohr, J.P. The natural history of CADASIL: A pooled analysis of previously published cases. Stroke J. Cereb. Circ. 1999, 30, 1230–1233. [Google Scholar] [CrossRef] [PubMed]
- Peters, N.; Opherk, C.; Bergmann, T.; Castro, M.; Herzog, J.; Dichgans, M. Spectrum of mutations in biopsy-proven CADASIL: Implications for diagnostic strategies. Arch. Neurol. 2005, 62, 1091–1094. [Google Scholar] [CrossRef] [PubMed]
- Dotti, M.T.; Federico, A.; Mazzei, R.; Bianchi, S.; Scali, O.; Conforti, F.L.; Sprovieri, T.; Guidetti, D.; Aguglia, U.; Consoli, D.; et al. The spectrum of Notch3 mutations in 28 Italian CADASIL families. J. Neurol. Neurosurg. Psychiatry 2005, 76, 736–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, S.C.; Chen, Y.R.; Chi, N.F.; Chen, C.H.; Cheng, Y.W.; Hsieh, F.I.; Hsieh, Y.C.; Yeh, H.L.; Sung, P.S.; Hu, C.J.; et al. Prevalence and clinical characteristics of stroke patients with p.R544C NOTCH3 mutation in Taiwan. Ann. Clin. Transl. Neurol. 2019, 6, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Tang, S.C.; Cheng, Y.W.; Tsai, H.H.; Chi, N.F.; Sung, P.S.; Yeh, H.L.; Lien, L.M.; Lin, H.J.; Lee, M.J.; et al. Detrimental effects of intracerebral haemorrhage on patients with CADASIL harbouring NOTCH3 R544C mutation. J. Neurol. Neurosurg. Psychiatry 2019, 90, 841–843. [Google Scholar] [CrossRef] [PubMed]
- Wollenweber, F.A.; Hanecker, P.; Bayer-Karpinska, A.; Malik, R.; Bazner, H.; Moreton, F.; Muir, K.W.; Muller, S.; Giese, A.; Opherk, C.; et al. Cysteine-sparing CADASIL mutations in NOTCH3 show proaggregatory properties in vitro. Stroke J. Cereb. Circ. 2015, 46, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Ihara, M.; Tham, C.; Low, R.W.; Slade, J.Y.; Moss, T.; Oakley, A.E.; Polvikoski, T.; Kalaria, R.N. Neuropathological correlates of temporal pole white matter hyperintensities in CADASIL. Stroke J. Cereb. Circ. 2009, 40, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.C.; Song, S.K.; Lee, J.S.; Kang, S.Y.; Kang, J.H. Diversity of stroke presentation in CADASIL: Study from patients harboring the predominant NOTCH3 mutation R544C. J. Stroke Cereb. Dis. 2013, 22, 126–131. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
NOTCH3 gene mutations. (A) NOTCH3 gene located on chromosome 19p13.12; (B) NOTCH3 gene mutations are located within the extracellular domain that encodes the epidermal growth factor like repeats, 3 Lin-NOTCH repeats, and 1 transmembrane region; (C) NOTCH3 gene mutations or variants of unknown significances in our study. Red bold text is the most common genetic region in this study. * Novel variants of unknown significance.
Figure 1.
NOTCH3 gene mutations. (A) NOTCH3 gene located on chromosome 19p13.12; (B) NOTCH3 gene mutations are located within the extracellular domain that encodes the epidermal growth factor like repeats, 3 Lin-NOTCH repeats, and 1 transmembrane region; (C) NOTCH3 gene mutations or variants of unknown significances in our study. Red bold text is the most common genetic region in this study. * Novel variants of unknown significance.

Figure 2.
Anterior temporal pole involvement according to specific exon locations.

Figure 3.
Anterior temporal pole involvement in prevalent NOTCH3 mutations compared to mutations in Exon 4. (A) NOTCH3 gene mutations of R75P, Y465C, R544C, and R1175W variants of unknown significance (VUS) and (B) NOTCH3 gene mutations in exon 4 (C123Y, R169C, R182C, and C185Y).
Figure 3.
Anterior temporal pole involvement in prevalent NOTCH3 mutations compared to mutations in Exon 4. (A) NOTCH3 gene mutations of R75P, Y465C, R544C, and R1175W variants of unknown significance (VUS) and (B) NOTCH3 gene mutations in exon 4 (C123Y, R169C, R182C, and C185Y).

Figure 4.
‘Founder effect’ reported in many countries.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Baseline characteristics of patients with known NOTCH 3 mutations or novel variants of unknown significance (VUS).
Table 1.
Baseline characteristics of patients with known NOTCH 3 mutations or novel variants of unknown significance (VUS).
| Age/Sex | Nucleotide | Exon | Amino Acid | Risk Factors | Symptom | MRI/MRA | Location of IS | Location of HS | No. of MBs | Location of MBs | Modified Fazekas | White Matter Lesions | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 57/M | 224G>C | 3 | R75P | DL | IS | +/+ | Rt. pons | 12 | B,D,E | 3 | a1,b1,c | |
| 2 | 43/M | 224G>C | 3 | R75P | HTN, DL | IS | +/+ | Rt. MCA | 1 | A | 2 | c | |
| 3 | 43/F | 224G>C | 3 | R75P | HTN | HS | +/+ | Rt. BG | 0 | 1 | c | ||
| 4 | 56/F | 224C>T | 3 | R75P | – | +/+ | 0 | 1 | c | ||||
| 5 | 64/F | 224C>T | 3 | R75P | DL | IS | +/+ | Lt. CR | 16 | B,C,E | 3 | b1,c | |
| 6 | 57/F | 224G>A | 3 | R75Q* | HTN, DM, DL | IS | +/+ | Lt. thalamus | 9 | A,B,E | 2 | c | |
| 7 | 34/F | 328C>T | 3 | R110C | – | +/+ | 0 | 2 | a1,b1,c | ||||
| 8 | 44/M | 368G>A | 4 | C123Y | IS | +/+ | CR | 14 | C,D,E | 3 | a2, b1,c | ||
| 9 | 59/M | 505C>T | 4 | R169C | IS | +/+ | Cerebellum | 4 | B | 3 | a2,b2,c | ||
| 10 | 57/F | 544C>T | 4 | R182C | HTN | IS | +/+ | Lt. BG | 3 | B | 3 | a2,b2,c | |
| 11 | 62/F | 554G>A | 4 | C185Y | migraine | +/+ | 3 | a2,b2,c | |||||
| 12 | 62/F | 634T>G | 4 | C212G* | HTN | IS, migraine | +/+ | Lt. CR | 0 | 2 | a2, b1,c | ||
| 13 | 49/M | 778T>G | 5 | C260G | HTN, DL, SM | IS | +/+ | Rt. CR | 0 | 2 | a2,c | ||
| 14 | 60/F | 832T>C | 6 | C278R* | DL | IS | +/+ | pons | 24 | B,C,E | 3 | a2,b2,c | |
| 15 | 51/F | 1378G>T | 8 | G460C* | HTN | migraine | +/+ | 15 | A,B,C,D,E | 2 | a2, b1,c | ||
| 16 | 44/F | 1378G>T | 8 | G460C* | HTN, DL | migraine | +/+ | 0 | 2 | b1,c | |||
| 17 | 52/F | 1394A>G | 9 | Y465C | HTN | – | +/+ | 2 | B,E | 3 | b1,c | ||
| 18 | 30/F | 1394A>G | 9 | Y465C | migraine | −/− | N/A | N/A | N/A | N/A | N/A | N/A | |
| 19 | 52/F | 1394A>G | 9 | Y465C | DM | – | +/+ | 0 | 3 | c | |||
| 20 | 46/M | 1394A>G | 9 | Y465C | HS | +/+ | Lt. thalamus | 0 | 1 | c | |||
| 21 | 52/M | 160C>T | 11 | R54C | HTN | IS, HS | +/+ | Lt. pons | Lt. BG | 23 | B,C,D,E | 3 | a2,b2,c |
| 22 | 49/F | 160C>T | 11 | R54C | migraine | +/+ | 0 | 3 | a2,b2,c | ||||
| 23 | 70/F | 1624T>C | 11 | C542R* | IS, migraine | +/+ | Rt. thalamus | 11 | B,C,D,E | 3 | a2,b2,c | ||
| 24 | 50/F | 1624T>C | 11 | C542R* | – | +/− | N/A | N/A | N/A | N/A | |||
| 25 | 60/F | 1630C>T | 11 | R544C | – | +/+ | 0 | 2 | c | ||||
| 26 | 55/M | 1630C>T | 11 | R544C | HTN | migraine | −/− | N/A | N/A | N/A | N/A | N/A | c |
| 27 | 43/F | 1630C>T | 11 | R544C | DL | – (MMD) | +/+ | 1 | B | 1 | c | ||
| 28 | 62/F | 1630C>T | 11 | R544C | IS | +/+ | Lt.thalamus | 10 | B,E | 2 | a1,b1,c | ||
| 29 | 64/M | 1759C>T | 11 | R587C | HS | +/+ | Lt. thalamus | 2 | E | 2 | c | ||
| 30 | 55/M | 3182G>A | 20 | C1061Y | HTN, DL | IS | +/+ | Rt. MCA | 41 | A,B,C,D,E | 3 | a2,b2,c | |
| 31 | 53/M | 3226C>T | 20 | R1075C* | – | +/+ | 6 | B,E | 3 | a1,b2,c | |||
| 32 | 68/M | 3523C>T | 22 | R1175W* | HTN, DL, SM | – | +/+ | 0 | 3 | a2,b2,c | |||
| 33 | 46/F | 3523C>T | 22 | R1175W* | HTN, DM, DL | IS, HS | +/+ | Lt. MCA | Lt. CR | 0 | 1 | – | |
| 34 | 35/F | 3523C>T | 22 | R1175W* | HS, (MMD) | +/+ | Lt. BG | 0 | 0 | – |
Location of MBs: A, Basal ganglia; B, thalamus; C, cerebellum; D, brainstem; E, subcortex. White matter lesions: a1, anterior temporal lobe, unilateral; a2, anterior temporal lobe, bilateral; b1, external capsule, unilateral; b2, external capsule, bilateral; c, periventricular white matters. * Novel variants of unknown significance. † Three patients (number 17–19) are one family. Patient No. 18 was a daughter of patient No.17 and patient No. 19 was a sister of patient No.17. Patient No. 26 did not have brain MRI images, and MRI results from other hospitals were available only on chart records. Abbreviations: DL, dyslipidemia; HTN, hypertension; DM, diabetes mellitus; SM, smoking; IS, ischemic stroke; HS, hemorrhagic stroke; MMD, moyamoya disease; Rt, right; Lt, left; MCA, middle cerebral artery; CR, corona radiata; BG, basal ganglia; N/A, not applicable; MBs, microbleeds; MRI, magnetic resonance image.
Table 2.
Comparison of the different spectrum of NOTCH3, MRI features, and clinical presentations of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
Table 2.
Comparison of the different spectrum of NOTCH3, MRI features, and clinical presentations of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
| Study | Race | Number of Patients | Age of Onset (± SD) | Mutation of NOTCH3 | MRI Features | Clinical Presentations | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Stroke | Cognitive Impairment | Psychiatric Syndrome | Headaches | Seizures | ||||||
| This study | Korean | 34 | 52.5 ± 9.5 | Exon 2–6: 41.2% (R75P/Q*: 17.6%) Exon 11: 26.5% | AT: 50% EC: 55.9% | IS: 44.1% ICH: 17.6% | Not specified | 0 | 2.5% | 0 |
| Markus et al., 2002 [2] | British | 48 | 35.9 ± 14.6 | Exon 2–6: 93.8% | AT:89% EC: 93% | IS: 29.2% ICH: not specified | 2.1% | 8.3% | 54.2% | 4.2% |
| Desmond et al., 1999 [10] | American | 105 | 36.7 ± 12.9 | Not specified | Not specified | IS: 42.9% | 5.7% | 8.6% | 40% | 2.9% |
| Dotti et al., 2005 [12] | Italian | 28 | Not specified | Exon 2–6: 46.42% Exon 11: 21.4% | Not specified | Not specified | Not specified | Not specified | Not specified | Not specified |
| Lee et al., 2009 [5] | Han Chinese in Taiwan | 21 | 48.6 ± 13.8 | Exon 2–6: 28.6% Exon 11 (R544C): 47.6% | AT: 42% EC: 95.2% | IS: 52.4% ICH: 23.8% | 4.8% | 9.5% | 4.8% | 4.8% |
| Liu et al., 2015 [4] | Chinese mainland | 62 | 39.7 ± 8.03 | Exon 4: 59.6% Exon 3: 22.8% Exon 11: 3.5% | AT: 63.5%* EC: 69.2%* | IS or TIA: 75.8% | 11.3% | 3.2% | 8.1% | Not specified |
| Choi et al., 2006 [7] | Korean | 20 | 57.2 ± 10.2 | Exon 2–6 (R75P): 10% Exon 11: 85% (R544C: 75%) | AT: 20% EC: 90% | IS: 55% ICH: 25% | 15% | 0 | 10% | 0 |
| Choi et al., 2013 [17] | Korean | 73 | 62.7 ± 11.1 | Exon 2–6 (R75P): 2.7% Exon 11: 95.9% (R544C: 90.3%) | Not specified | IS: 42.5% ICH: 12.3% | Not specified | Not specified | Not specified | Not specified |
| Kim et al., 2006 [6] | Korean | 27 | 47.7 | Exon 2–6: 77.8% (R75P: 55.6%) Exon 11: 22.2% | AT: 22.2% EC: 51.9% | IS: 40.7% ICH: 33.3% | 18.5% | Depression 14.8% | 3.7% | 0 |
| Ueda et al., 2015 [8] | Japanese | 70 | Patients with R75P: 53.6 ± 6.9 Patients with other mutations: 44.2 ± 12 | Exon 3: 21% Exon 4: 69% | AT: 70.6%† EC: 76.5%† | IS or TIA: 69% | 31% | 20% | 33% | Not specified |
Abbreviations: SD, standard deviation; AT, anterior temporal; EC, external capsular; IS, ischemic; ICH, intracerebral hemorrhage. * Frequency was calculated among 52 patients with CADASIL Scale scores. † Frequency was calculated among 51 CADASIL patients with available MRI data.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kim, Y.; Lee, S.-H. Novel Characteristics of Race-Specific Genetic Functions in Korean CADASIL. Medicina 2019, 55, 521. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090521
AMA Style
Kim Y, Lee S-H. Novel Characteristics of Race-Specific Genetic Functions in Korean CADASIL. Medicina. 2019; 55(9):521. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090521
Chicago/Turabian StyleKim, Yerim, and Seung-Hoon Lee. 2019. "Novel Characteristics of Race-Specific Genetic Functions in Korean CADASIL" Medicina 55, no. 9: 521. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090521