Use of Medicinal Cannabis and Synthetic Cannabinoids in Post-Traumatic Stress Disorder (PTSD): A Systematic Review

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
1.1. Post Traumatic Stress Disorder (PTSD)
1.2. Therapeutic Approaches for PTSD
1.3. Cannabis use in PTSD: A Coping Strategy?
1.4. Cannabis, Cannabinoids, and Their Role in PTSD
- (1)
- CB1 receptors are found in moderate to high levels throughout brain limbic structures, and have been shown to possess modulating properties on behaviors, including mood, stress, learning, and memory [4]: in fact, by activating the CB1 receptors in the amygdala, cannabis can potentially block the consolidation of aversive memories, fear, and anxiety; moreover, through stimulating CB1 receptors in the prefrontal cortex, cannabis may increase serotonin and, therefore, display antidepressant properties; finally, cannabis agonism on CB1 receptors in the hippocampus seems to improve neurogenesis, mood, and memory as well as causing decreases in hypervigilance, hyperarousal, and intrusive memories, effects which may contribute to the anxiolytic and antidepressant effects of cannabinoids [1,4,5,7]; conversely, animal studies have shown that a reduction in the number of CB1 receptors may be associated with heightened indices of anxiety and depression, especially if the disorder persists [4].
- (2)
- Stimulation of the limbic and paralimbic areas might decrease amygdala and hypothalamus activity, regulating the hypothalamic–pituitary axis and cortisol response, and, therefore, decreasing hypervigilance and hyperarousal [1,5]. Conversely, a low eCB tone contributes to amygdala hyperactivation as well as anxiety and hyperarousal symptoms characteristic of PTSD, including sleep disturbances, memory and cognitive impairments, depression, and suicidality [14]. Interestingly, a difference in gender has been evidenced, with males showing a higher degree of endocannabinoids released in response to a stressor and stronger physiological effects to cannabis compared to women [4,26,27];
- (3)
- (4)
- Cannabinoid modulation exerts effects on memory processes through alteration of the brain-derived neurotrophic factor (BDNF) concentrations in the hippocampus and the basolateral amygdala, as well as altering long-term potentiation in hippocampal neurons [27].
1.5. Therapeutic use of Synthetic Cannabinoids in PTSD
1.6. Aims of the Paper
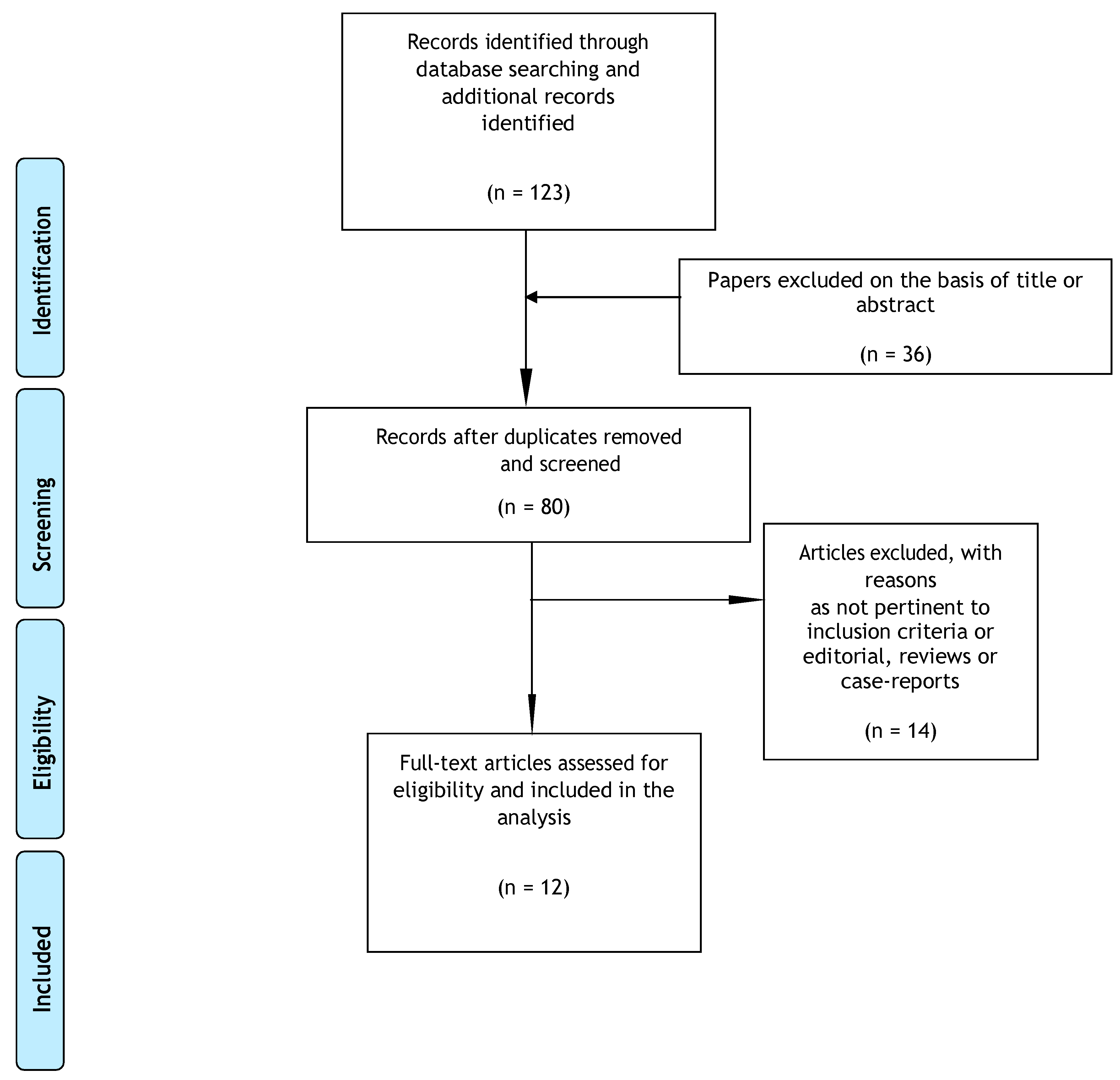
2. Methods
2.1. Search Sources and Strategies
2.2. Study Selection
2.3. Data Extraction and Management
2.4. Characteristics of Included Studies
3. Results
3.1. Medical Cannabis
3.2. THC
3.3. CBD
3.4. Nabilone
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Bitencourt, R.M.; Takahashi, R.N. Cannabidiol as a therapeutic alternative for post-traumatic stress disorder: From bench research to confirmation in human trials. Front. Neurosci. 2018, 12, 502. [Google Scholar] [CrossRef] [PubMed]
- Jurkus, R.; Day, H.L.L.; Guimares, F.S.; Lee, J.L.C.; Bertoglio, L.J.; Stevenson, C.W. Cannabidiol regulation of learned fear: Implications for treating anxiety-related disorders. Front. Pharmacol. 2016, 7, 454. [Google Scholar] [CrossRef] [PubMed]
- Shorter, D.; Hsieh, J.; Kosten, T.R. Pharmacologic management of comorbid post-traumatic stress disorder and addictions. Am. J. Addict. 2015, 24, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.R.; Cordell, E.; Sobin, S.M.; Neumeister, A. Recent Progress in Understanding the Pathophysiology of Post-Traumatic Stress Disorder Implications for Targeted Pharmacological Treatment. CNS Drugs 2013, 27, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Shishko, I.; Oliveira, R.; Moore, T.A.; Almeida, K. A review of medical marijuana for the treatment of post-traumatic stress disorder: Real symptom re-leaf or just high hopes? Ment. Health Clin. 2018, 8, 86–94. [Google Scholar] [CrossRef] [PubMed]
- NICE. National Institute for Health and Care Excellence. Guideline Post-Traumatic Stress Disorder. 2018. Available online: https://www.nice.org.uk/guidance/ng116/documents/draft-guideline-2 (accessed on 23 June 2019).
- Berardi, A.; Schelling, G.; Campolongo, P. The endocannabinoid system and Post Traumatic Stress Disorder (PTSD): From preclinical findings to innovative therapeutic approaches in clinical settings. Pharmacol. Res. 2016, 111, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Ostacher, M.J.; Cifu, A.S. Management of Post-Traumatic Stress Disorder. Available online: https://www.oregonpainguidance.org/wp-content/uploads/2018/02/JAMA-2019-Management-of-Posttraumatic-Stress-Disorder.pdf?x91687 (accessed on 23 June 2019).
- De Berardis, D.; Marini, S.; Serroni, N.; Iasevoli, F.; Tomasetti, C.; de Bartolomeis, A.; Mazza, M.; Tempesta, D.; Valchera, A.; Fornaro, M.; et al. Targeting the noradrenergic system in post-traumatic stress disorder: A systematic review and meta-analysis of prazosin trials. Curr. Drug Targets 2015, 16, 1094–1106. [Google Scholar] [CrossRef] [PubMed]
- De Silva, V.A.; Jayasekera, N.; Hanwella, R. Cannabis use among Navy personnel in Sri Lanka: A cross sectional study. BMC Res. Notes 2016, 9, 174. [Google Scholar] [CrossRef]
- Patel, S.; Hill, M.N.; Cheer, J.F.; Wotjak, C.T.; Holmes, A. The endocannabinoid system as a target for novel anxiolytic drugs. Neurosci. Biobehav. Rev. 2017, 76 Pt A, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Ruglass, L.M.; Shevorykin, A.; Radoncic, V.; Smith, K.M.Z.; Smith, P.H.; Galatzer-Levy, I.R.; Papini, S.; Hien, D.A. Impact of cannabis use on treatment outcomes among adults receiving cognitive-behavioral treatment for PTSD and substance use disorders. J. Clin. Med. 2017, 6, 14. [Google Scholar] [CrossRef]
- Schifano, F.; Papanti, G.D.; Corkery, J.M.; Orsolini, L. Post-traumatic stress and substance misuse; neurobiological and clinical pharmacological correlates. RAP 2018, 5, 50–58. [Google Scholar]
- Bonn-Miller, M.O.; Babson, K.A.; Vandrey, R. Using cannabis to help you sleep: Heightened frequency of medical cannabis use among those with PTSD. Drug Alcohol Depend. 2014, 136, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Bonn-Miller, M.O.; Harris, A.H.S.; Trafton, J.A. Prevalence of cannabis use disorder diagnoses among veterans in 2002, 2008, and 2009. Psychol. Serv. 2012, 9, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Bordieri, M.J.; Tull, M.T.; McDermott, M.J.; Gratz, K.L. The Moderating role of experiential avoidance in the relationship between post-traumatic stress disorder symptom severity and cannabis dependence. J. Contextual Behav. Sci. 2014, 3, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Earleywine, M.; Bolles, J.R. Marijuana, expectancies, and post-traumatic stress symptoms: A preliminary investigation. J. Psychoact. Drugs 2014, 46, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Trezza, V.; Campolongo, P. The endocannabinoid system as a possible target to treat both the cognitive and emotional features of post-traumatic stress disorder (PTSD). Front. Behav. Neurosci. 2013, 7, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonn-Miller, M.O.; Moos, R.H.; Boden, M.T.; Long, W.R.; Kimerling, R.; Trafton, J.A. The impact of post-traumatic stress disorder on cannabis quit success. Am. J. Drug Alcohol Abus. 2015, 41, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.K.; Bonar, E.E.; Ilgen, M.A.; Walton, M.A.; Perron, B.E.; Chermack, S.T. Factors associated with having amedical marijuana card among Veterans with recent substance use in VA outpatient treatment. Addict. Behav. 2016, 63, 132–136. [Google Scholar] [CrossRef]
- Gentes, E.L.; Schry, A.R.; Hicks, T.A.; Clancy, C.P.; Collie, C.F.; Kirby, A.C.; Dennis, M.F.; Hertzberg, M.A.; Beckham, J.C.; Calhoun, P.S. Prevalence and correlates of cannabis use in an outpatient VA posttraumatic stress disorder clinic. Psychol. Addict. Behav. 2016, 30, 415–421. [Google Scholar] [CrossRef]
- Buckner, J.D.; Jeffries, E.R.; Crosby, R.D.; Zvolensky, M.J.; Cavanaugh, C.E.; Wonderlich, S.A. The impact of PTSD clusters on cannabis use in a racially diverse trauma-exposed sample: An analysis from ecological momentary assessment. Am. J. Drug Alcohol Abuse 2018, 44, 532–542. [Google Scholar] [CrossRef]
- Elliott, L.; Golub, A.; Bennett, A.; Guarino, H. PTSD and cannabis-related coping among recent veterans in New York City. Contemp. Drug Probl. 2015, 42, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Pisanti, S.; Malfitano, A.M.; Ciaglia, E.; Lamberti, A.; Ranieri, R.; Cuomo, G.; Abate, M.; Faggiana, G.; Proto, M.C.; Fiore, D.; et al. Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacol. Ther. 2017, 175, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Elms, L.; Shannon, S.; Hughes, S.; Lewis, N. Cannabidiol in the treatment of Post-Traumatic Stress Disorder: A case series. J. Altern. Complement. Med. 2019, 25, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Ney, L.J.; Matthews, A.; Bruno, R.; Felmingham, K.L. Modulation of the endocannabinoid system by sex hormones: Implications for posttraumatic stress disorder. Neurosci. Biobehav. Rev. 2018, 94, 302–320. [Google Scholar] [CrossRef] [PubMed]
- Ney, L.J.; Matthews, A.; Bruno, R.; Felmingham, K.L. Cannabinoid interventions for PTSD: Where to next? Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 93, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.; Watson, D.; Robinson, J. Use of a synthetic cannabinoid in a correctional population for posttraumatic stress disorder related insomnia and nightmares, chronic pain, harm reduction, and other indications a retrospective evaluation. J. Clin. Psychopharmacol. 2014, 34, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Prud’homme, M.; Cata, R.; Jutras-Aswad, D. Cannabidiol as an intervention for addictive behaviors: A systematic review of the evidence. Subst. Abuse 2015, 9, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.L.C.; Bertoglio, L.J.; Guimarães, F.S.; Stevenson, C. Cannabidiol regulation of emotion and emotional memory processing: Relevance for treating anxiety-related and substance abuse disorders. Br. J. Pharmacol. 2017, 174, 3242–3256. [Google Scholar] [CrossRef]
- Korem, N.; Mizrachi Zer-Aviva, T.; Ganon-Elazar, E.; Abush, I.; Akirav, I. Targeting the endocannabinoid system to treat anxiety-related disorders. J. Basic Clin. Physiol. Pharmacol. 2016, 27, 193–202. [Google Scholar] [CrossRef]
- El-Solh, A.A. Management of nightmares in patients with posttraumatic stress disorder: Current perspectives. Nat. Sci. Sleep 2018, 10, 409–420. [Google Scholar] [CrossRef]
- Fraser, G.A. The use of a synthetic cannabinoid in the management of treatment-resistant nightmares in posttraumatic stress disorder (PTSD). CNS Neurosci. Ther. 2009, 15, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, 5th ed.; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochrane-handbook.org (accessed on 2 December 2015).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Bonn-Miller, M.O.; Boden, M.T.; Bucossi, M.M.; Babson, K.A. Self-reported cannabis use characteristics, patterns and helpfulness among medical cannabis users. Am. J. Drug Alcohol Abuse 2014, 40, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Greer, G.R.; Grob, C.S.; Halberstadt, A.L. PTSD symptom reports of patients evaluated for the New Mexico Medical Cannabis Program. J. Psychoact. Drugs 2014, 46, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, S.T.; Stefanovics, E.; Rosenheck, R.A. Marijuana use is associated with worse outcomes in symptom severity and violent behavior in patients with posttraumatic stress disorder. J. Clin. Psychiatry 2015, 76, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Tull, M.T.; McDermott, M.J.; Gratz, K.L. Marijuana dependence moderates the effect of posttraumatic stress disorder on trauma cue reactivity in substance dependent patients. Drug Alcohol Depend. 2016, 159, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Roitman, P.; Mechoulam, R.; Cooper-Kazaz, R.; Shalev, A. Preliminary, open-label, pilot study of add-on oral Delta9-tetrahydrocannabinol in chronic post-traumatic stress disorder. Clin. Drug Investig. 2014, 34, 587–591. [Google Scholar] [CrossRef]
- Johnson, M.J.; Pierce, J.D.; Mavandadi, S.; Klaus, J.; Defelice, D.; Ingram, E.; Oslin, D.W. Mental health symptom severity in cannabis using and non-using Veterans with probable PTSD. J. Affect. Disord. 2016, 190, 439–442. [Google Scholar] [CrossRef] [Green Version]
- Jetly, R.; Heber, A.; Fraser, G.; Boisvert, D. The efficacy of nabilone, a synthetic cannabinoid, in the treatment of PTSD-associated nightmares: A preliminary randomized, double-blind, placebo-controlled cross-over design study. Psychoneuroendocrinology 2015, 51, 585–588. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Goldstein, R.B.; Southwick, S.M.; Grant, B.F. Prevalence and Axis I comorbidity of full and partial posttraumatic stress disorder in the United States: Results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Anxiety Disord. 2011, 25, 456–465. [Google Scholar] [CrossRef] [Green Version]
- Bedard-Gilligan, M.; Garcia, N.; Zoellner, L.A.; Feeny, N.C. Alcohol, cannabis, and other drug use: Engagement and outcome in PTSD treatment. Psychol. Addict. Behav. 2018, 32, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Leeies, M.; Pagura, J.; Sareen, J.; Bolton, J.M. The use of alcohol and drugs to self-medicate symptoms of posttraumatic stress disorder. Depress. Anxiety 2010, 27, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Blanco, C.; Xu, Y.; Brady, K.; Pérez-Fuentes, G.; Okuda, M.; Wang, S. Comorbidity of posttraumatic stress disorder with alcohol dependence among U.S. adults: Results from National Epidemiological Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2013, 132, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; Kavanagh, D.; Young, R. Being stoned: A review of self-reported cannabis effects. Drug Alcohol Rev. 2003, 22, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Cougle, J.R.; Bonn-Miller, M.O.; Vujanovic, A.A.; Zvolensky, M.J.; Hawkins, K.A. Posttraumatic stress disorder and cannabis use in a nationally representative sample. Psychol. Addict. Behav. 2013, 25, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Blessing, E.M.; Steenkamp, M.M.; Manzanares, J.; Marmar, C.R. Cannabidiol as a potential treatment for anxiety disorders. Neurotherapeutics 2015, 12, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Shannon, S.; Oplia-Lehman, J. Effectiveness of cannabidiol oil for pediatric anxiety and insomnia as part of posttraumatic stress disorder: A case report. Perm. J. 2016, 20, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Soares, V.d.P.; Campos, A.C.; Bortoli VCd Zangrossi, H.; Guimarães, F.S.; Zuardi, A.W. Intra-dorsal periaqueductal gray administration of cannabidiol blocks paniclike response by activating 5-HT1A receptors. Behav. Brain Res. 2010, 213, 225–229. [Google Scholar] [CrossRef]
- Campos, A.C.; de Paula Soares, V.; Carvalho, M.C.; Ferreira, F.R.; Vicente, M.A.; Brandao, M.L.; Zuardi, A.W.; Zangrossi, H., Jr.; Guimaraes, F.S. Involvement of serotonin-mediated neurotransmission in the dorsal periaqueductal gray matter on cannabidiol chronic effects in paniclike responses in rats. Psychopharmacology 2013, 226, 13–24. [Google Scholar] [CrossRef]
- Mizrachi Zer-Aviv, T.; Segev, A.; Akirav, I. Cannabinoids and post-traumatic stress disorder: Clinical and preclinical evidence for treatment and prevention. Behav. Pharmacol. 2016, 27, 561–569. [Google Scholar] [CrossRef]
- Babson, K.A.; Sottile, J.; Morabito, D. Cannabis, Cannabinoids, and Sleep: A Review of the Literature. Curr. Psychiatry Rep. 2017, 19, 23. [Google Scholar] [CrossRef] [PubMed]
- Metrik, J.; Bassett, S.S.; Aston, E.R.; Jackson, K.M.; Borsari, B. Medicinal versus Recreational Cannabis Use among Returning Veterans. Transl. Issues Psychol. Sci. 2018, 4, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Patel, S. Cannabis for pain and posttraumatic stress disorder: More consensus than controversy or vice versa? Ann. Intern. Med. 2017, 167, 355–356. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study (Author(s), Year of Publication) | Sample Characteristics | Cannabinoid or Cannabis-Based Medicine Implicated | Control Group (If Any) | Dose (s) | ROA | Outcomes Measures Used | Main Findings |
|---|---|---|---|---|---|---|---|
| Bonn-Miller et al. (2014a) [14] | 170 patients at a medical cannabis dispensary in California | CBD + THC | Pts without PTSD | n.d. | n.d. | PCL-C CMMQ MSHQ AUDIT IDAS | Improvement of PTSD-related sleep disturbances but only 8/40 of PTSD subjects reported a reduction in PTSD symptoms. |
| Earleywine and Bolles (2014) [17] | 650 combat-exposed male veterans | THC | None | unknown | Smoked, at least once per week | PCL-M CES | Significant expectations of cannabis-induced relief from PTSD symptomatology, particularly for intrusion, hyperarousal, then avoidance, and numbing. |
| Elms et al. (2019) [25] | 11 PTSD outpatients | CBD | None | Flexible for 8 weeks | OS capsule or liquid spray once or twice per day based on severity of symptoms | PCL-5 | Decreased PTSD symptom severity at 8 weeks from baseline. |
| Cameron et al. (2014) [28] | 104 male inmates with serious mental illness | Nabilone | None | Mean initial dose: 1.4 mg daily (0.5-2 mg) Mean final dose: 5 mg daily (0.5-6 mg) | n.d. | PCL-C GAF | Significant improvement in PTSD-associated insomnia, nightmares, PTSD symptoms. |
| Fraser (2009) [33] | 47 patients with treatment-resistant PTSD | Nabilone | None | 0.5 mg titrated up to a max of 4 mg daily | OS 1 h prior to bedtime | Nightmare presence and intensity; hours of sleep | Reduction in nightmare intensity, subjective improvement in sleep time, quality of sleep, and reduction of daytime flashbacks and night sweats. |
| Bonn-Miller et al. (2014b) [36] | 217 patients at a medical cannabis dispensary in California | CBD + THC | Pts without PTSD | n.d. | n.d. | n.d. | Reduction of stress, anxiety, depression, and PTSD symptomatology. |
| Greer et al., (2014) [37] | 80 PTSD patients | CBD+THC | None | Unknown proportion | Smoked | CAPS | PTSD symptoms reduction. |
| Wilkinson et al. (2015) [38] | 2276 PTSD veterans admitted to intensive PTSD treatment programs and divided into a) never cannabis users; b) cannabis users stoppers; c) continuing cannabis users; d) cannabis use starters | CBD+THC | Comparing groups | n.d. | n.d. | ASI MISS for PTSD | Starting cannabis use worsened PTSD symptoms. Stopping cannabis use improved PTSD symptoms. At follow-up, stoppers and never cannabis users had lower levels of PTSD symptoms, and starters had the highest levels of violent behavior. |
| Tull et al. (2016) [39] | 202 subjects with and without PTSD with a co-occurring stimulant, cocaine or alcohol use disorder admitted to a SUD treatment facility | CBD + THC | Placebo | n.d. | n.d. | SCID-I CAPS MINI PANAS DUQ | Current PTSD was associated with greater subjective emotional reactivity to the trauma script only in subjects without cannabis use. Cannabis users (with and without PTSD) reported less subjective emotional reactivity than participants with PTSD but without cannabis use. |
| Roitman et al. (2014) [40] | 10 PTSD outpatients from Israel | THC | None | 2x2.5 mg daily titrated to 5 mg x 2 daily | OS 1 h after waking up and 2 h prior to bed | PSQI NFQ NES | Reduction in nightmares and improvement in sleep quality. |
| Johnson et al. (2016) [41] | 700 veterans enrolled in the primary care mental health integration program | THC | Placebo | n.d. | Smoked | TLFB ASSIST PCL-CPHQ-9 PQSIA BOMC | No association between cannabis use and less severe PTSD symptomatology. |
| Jetly et al. (2015) [42] | 10 male military personnel with PTSD | Nabilone | Placebo | 0.5 mg titrated to 3 mg | OS 1 h prior to bed | CAPS sleep items PTSD dream rating scale Sleep diary CGI-C WBQ | Reduction in nightmares. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsolini, L.; Chiappini, S.; Volpe, U.; De Berardis, D.; Latini, R.; Papanti, G.D.; Corkery, J.M. Use of Medicinal Cannabis and Synthetic Cannabinoids in Post-Traumatic Stress Disorder (PTSD): A Systematic Review. Medicina 2019, 55, 525. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090525
Orsolini L, Chiappini S, Volpe U, De Berardis D, Latini R, Papanti GD, Corkery JM. Use of Medicinal Cannabis and Synthetic Cannabinoids in Post-Traumatic Stress Disorder (PTSD): A Systematic Review. Medicina. 2019; 55(9):525. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090525
Chicago/Turabian StyleOrsolini, Laura, Stefania Chiappini, Umberto Volpe, Domenico De Berardis, Roberto Latini, Gabriele Duccio Papanti, and John Martin Corkery. 2019. "Use of Medicinal Cannabis and Synthetic Cannabinoids in Post-Traumatic Stress Disorder (PTSD): A Systematic Review" Medicina 55, no. 9: 525. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090525