Gastrointestinal Symptoms of and Psychosocial Changes in Inflammatory Bowel Disease: A Nursing-Led Cross-Sectional Study of Patients in Clinical Remission

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Instruments
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Characteristics of the Study Group
3.2. Characteristics Of Gastrointestinal Symptoms and Psychosocial Alterations among IBD Patients
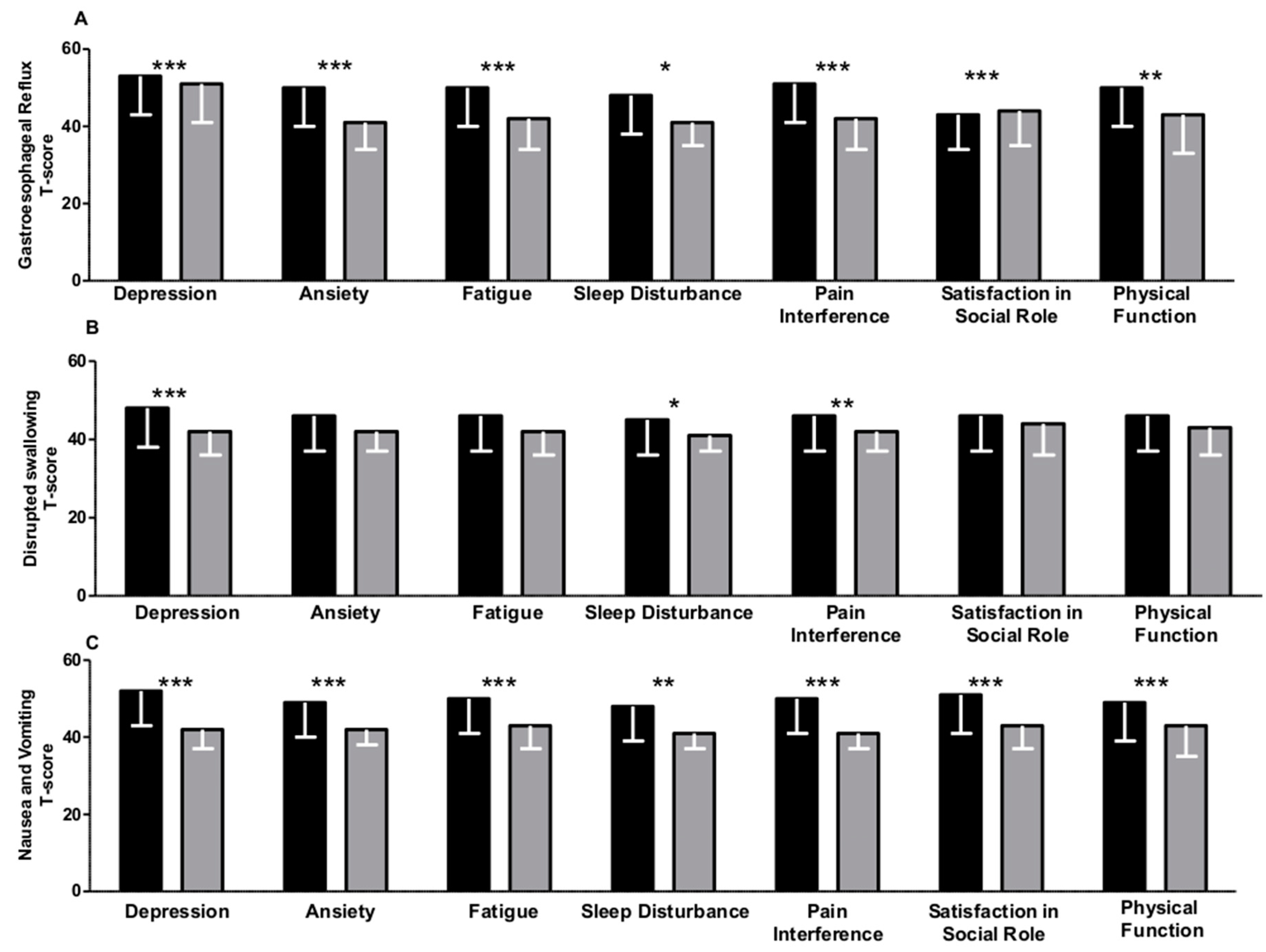
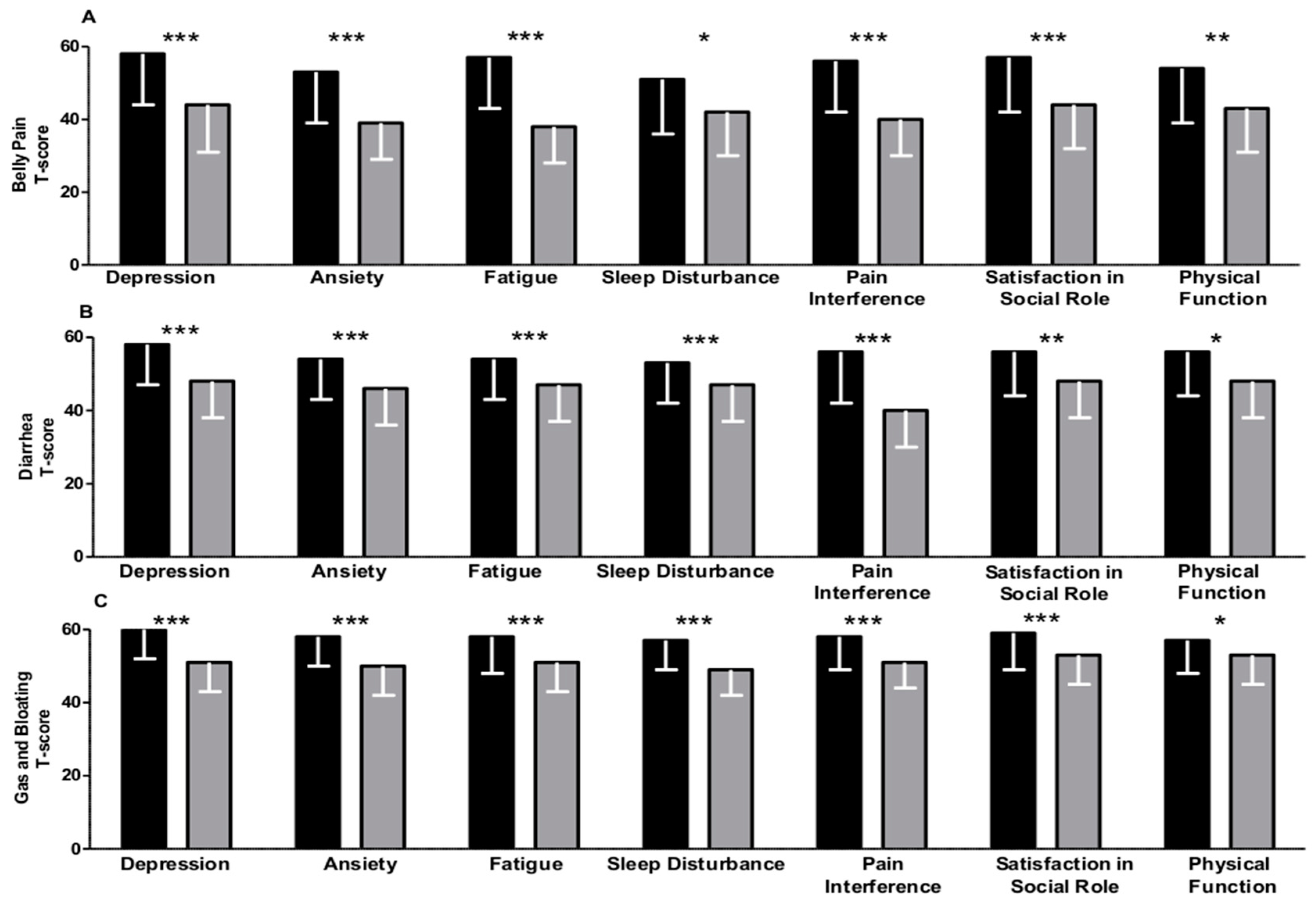
3.3. Gastrointestinal Symptoms Are Associated with Psychosocial Changes in IBD Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kemp, K.; Dibley, L.; Chauhan, U.; Greveson, K.; Jäghult, S.; Ashton, K.; Buckton, S.; Duncan, J.; Hartmann, P.; Ipenburg, N.; et al. 2nd N-ECCO Consensus Statements on the European Nursing Roles in Caring for Patients with Crohn’s Disease or Ulcerative Colitis. J. Crohn’s Colitis 2018, 12, 760–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devlen, J.; Beusterien, K.; Yen, L.; Ahmed, A.; Cheifetz, A.S.; Moss, A.C. The burden of inflammatory bowel disease: A patient-reported qualitative analysis and development of a conceptual model. Inflamm. Bowel Dis. 2014, 20, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Neuendorf, R.; Harding, A.; Stello, N.; Hanes, D.; Wahbeh, H. Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J. Psychosom. Res. 2016, 87, 70–80. [Google Scholar] [CrossRef]
- Taft, T.H.; Keefer, L.; Artz, C.; Bratten, J.; Jones, M.P. Perceptions of illness stigma in patients with inflammatory bowel disease and irritable bowel syndrome. Qual. Life Res. 2011, 20, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Dibley, L.; Norton, C.; Whitehead, E. The experience of stigma in inflammatory bowel disease: An interpretive (hermeneutic) phenomenological study. J. Adv. Nurs. 2018, 74, 838–851. [Google Scholar] [CrossRef] [PubMed]
- Wilburn, J.; Twiss, J.; Kemp, K.; McKenna, S.P. A qualitative study of the impact of Crohn’s disease from a patient’s perspective. Frontline Gastroenterol. 2017, 8, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, A.J.; Rowse, G.; Ryder, A.; Peach, E.J.; Corfe, B.M.; Lobo, A.J. Systematic review: Psychological morbidity in young people with inflammatory bowel disease-risk factors and impacts. Aliment. Pharm. 2016, 44, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.; Mitchell, R. Impact of inflammatory bowel disease on quality of life: Results of the European Federation of Crohn’s and Ulcerative Colitis Associations (EFCCA) patient survey. J. Crohn’s Colitis 2007, 1, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Haapamäki, J.; Turunen, U.; Roine, R.P.; Färkkilä, M.A.; Arkkila, P.E. Finnish patients with inflammatory bowel disease have fewer symptoms and are more satisfied with their treatment than patients in the previous European survey. Scand. J. Gastroenterol. 2008, 43, 821–830. [Google Scholar]
- Haapamäki, J.; Turunen, U.; Roine, R.P.; Färkkilä, M.A.; Arkkila, P.E. Impact of demographic factors, medication and symptoms on disease-specific quality of life in inflammatory bowel disease. Qual. Life Res. 2009, 18, 961–969. [Google Scholar] [CrossRef]
- Horváth, G.; Farkas, K.; Hollósi, R.; Nagy, F.; Szepes, Z.; Papp, M.; Palatka, K.; Miheller, P.; Lakatos, L.; Szamosi, T.; et al. Is there any association between impaired health-related quality of life and non-adherence to medical therapy in inflammatory bowel disease? Scand. J. Gastroenterol. 2012, 47, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Portela, F.; Lago, P.; Deus, J.; Cotter, J.; Cremers, I.; Vieira, A.; Peixe, P.; Caldeira, P.; Lopes, H.; et al. Inflammatory bowel disease: A patient’s and caregiver’s perspective. Dig. Dis. Sci. 2009, 54, 2671–2679. [Google Scholar] [CrossRef] [PubMed]
- van Langenberg, D.R.; Gibson, P.R. Systematic review: Fatigue in inflammatory bowel disease. Aliment. Pharm. 2010, 32, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Graff, L.A.; Vincent, N.; Walker, J.R.; Clara, I.; Carr, R.; Ediger, J.; Miller, N.; Rogala, L.; Rawsthorne, P.; Lix, L.; et al. A population-based study of fatigue and sleep difficulties in inflammatory bowel disease. Inflamm. Bowel. Dis. 2011, 17, 1882–1889. [Google Scholar] [CrossRef]
- Guthrie, E.; Jackson, J.; Shaffer, J.; Thompson, D.; Tomenson, B.; Creed, F. Psychological disorder and severity of inflammatory bowel disease predict health-related quality of life in ulcerative colitis and Crohn’s disease. Am. J. Gastroenterol. 2002, 97, 1994–1999. [Google Scholar] [CrossRef]
- Vidal, A.; Gómez-Gil, E.; Sans, M.; Portella, M.J.; Salamero, M.; Piqué, J.M.; Panés, J. Health-related quality of life in inflammatory bowel disease patients: The role of psychopathology and personality. Inflamm. Bowel. Dis. 2008, 14, 977–983. [Google Scholar] [CrossRef]
- Bojic, D.; Bodger, K.; Travis, S. Patient Reported Outcome Measures (PROMs) in Inflammatory Bowel Disease: New Data. J. Crohns Colitis 2017, 11, S576–S585. [Google Scholar] [CrossRef]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Med. Care 2007, 45, S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Spiegel, B.M.; Hays, R.D.; Bolus, R.; Melmed, G.Y.; Chang, L.; Whitman, C.; Khanna, P.P.; Paz, S.H.; Hays, T.; Reise, S.; et al. Development of the NIH Patient-Reported Outcomes Measurement Information System (PROMIS) gastrointestinal symptom scales. Am. J. Gastroenterol. 2014, 109, 1804–1814. [Google Scholar] [CrossRef] [Green Version]
- Kochar, B.; Martin, C.F.; Kappelman, M.D.; Spiegel, B.M.; Chen, W.; Sandler, R.S.; Long, M.D. Evaluation of Gastrointestinal Patient Reported Outcomes Measurement Information System (GI-PROMIS) Symptom Scales in Subjects With Inflammatory Bowel Diseases. Am. J. Gastroenterol. 2018, 113, 72–79. [Google Scholar] [CrossRef]
- Conley, S.; Proctor, D.D.; Jeon, S.; Sandler, R.S.; Redeker, N.S. Symptom clusters in adults with inflammatory bowel disease. Res. Nurs. Health 2017, 40, 424–434. [Google Scholar] [CrossRef]
- Conley, S.; Jeon, S.; Proctor, D.D.; Sandler, R.S.; Redeker, N.S. Longitudinal Changes in Symptom Cluster Membership in Inflammatory Bowel Disease. J. Nurs. Sch. 2018, 50, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, D.; Choi, S.; Garcia, S.; Cook, K.F.; Rosenbloom, S.; Lai, J.S.; Tatum, D.S.; Gershon, R. Setting standards for severity of common symptoms in oncology using the PROMIS item banks and expert judgment. Qual. Life Res. 2014, 23, 2651–2661. [Google Scholar] [CrossRef] [Green Version]
- Berrill, J.W.; Green, J.T.; Hood, K.; Campbell, A.K. Symptoms of irritable bowel syndrome in patients with inflammatory bowel disease: Examining the role of sub-clinical inflammation and the impact on clinical assessment of disease activity. Aliment. Pharm. 2013, 38, 44–51. [Google Scholar] [CrossRef]
- Ansari, R.; Attari, F.; Razjouyan, H.; Etemadi, A.; Amjadi, H.; Merat, S.; Malekzadeh, R. Ulcerative colitis and irritable bowel syndrome: Relationships with quality of life. Eur. J. Gastroenterol. Hepatol. 2008, 20, 46–50. [Google Scholar] [CrossRef]
- Spagnuolo, R.; Cosco, C.; Mancina, R.M.; Ruggiero, G.; Garieri, P.; Cosco, V.; Doldo, P. Beta-glucan, inositol and digestive enzymes improve quality of life of patients with inflammatory bowel disease and irritable bowel syndrome. Eur. Rev. Med. Pharm. Sci. 2017, 21, 102–107. [Google Scholar]



{kind=link}
{kind=link}
| N | 109 |
|---|---|
| Demographic and Anthropometric | |
| Age (years) | 50 (42–59) |
| Male gender, n (%) | 69 (62) |
| BMI (Kg/m2) | 25 (23–27) |
| Smoke, n (%) | 14 (13) |
| Disease characteristics | |
| Crohn’s disease, n (%) | 32 (29) |
| Ulcerative Colitis, n (%) | 78 (71) |
| Disease duration (years) | 12 (0–34) |
| CD (Harvey Bradshaw index) | 2 (0–5) |
| UC (full Mayo Score) | 1 (0–2) |
| Surgery, n (%) | 13 (12) |
| CD disease location, n (%)† | |
| Ileal | 15 (47) |
| Ileo-Colonic | 13 (41) |
| Other Upper GI | 4 (12) |
| UC disease location, n (%) ‡ | |
| Proctitis | 5 (6) |
| Proctosigmoiditis | 10 (13) |
| Left-side | 20 (26) |
| Pancolitis | 40 (51) |
| Medications, n (%) | |
| Mesalamine | 97 (84) |
| Steroids | 10 (9) |
| Thyopurine | 9 (8) |
| Biological | 16 (14) |
| N = 109 | Yes | Median t-Score ± SD |
|---|---|---|
| GI-PROMIS | ||
| Belly pain, n (%) | 56 (51) | 48 (33–58) |
| Gas and Bloating, n (%) | 79 (72) | 57 (47–62) |
| Diarrhea, n (%) | 61 (56) | 52 (39–59) |
| Gastroesophageal Reflux, n (%) | 45 (41) | 47 (36–52) |
| Disrupted Swallowing, n (%) | 20 (18) | 46 (40–49) |
| Nausea and Vomiting, n (%) | 33 (30) | 47 (40–55) |
| PROMIS | ||
| Depression, n (%) | 43 (39) | 48 (38–56) |
| Anxiety, n (%) | 76 (70) | 54 (45–62 |
| Fatigue, n (%) | 65 (60) | 53 (42–60) |
| Sleep Disturbance, n (%) | 87 (79) | 53 (46–54) |
| Pain interference, n (%) | 62 (56) | 55 (40–60) |
| Satisfaction with participation in social roles, n (%) | 46 (43) | 53 44–65) |
| Physical Function, n (%) | 47 (43) | 50 (43–60) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mancina, R.M.; Pagnotta, R.; Pagliuso, C.; Albi, V.; Bruno, D.; Garieri, P.; Doldo, P.; Spagnuolo, R. Gastrointestinal Symptoms of and Psychosocial Changes in Inflammatory Bowel Disease: A Nursing-Led Cross-Sectional Study of Patients in Clinical Remission. Medicina 2020, 56, 45. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56010045
Mancina RM, Pagnotta R, Pagliuso C, Albi V, Bruno D, Garieri P, Doldo P, Spagnuolo R. Gastrointestinal Symptoms of and Psychosocial Changes in Inflammatory Bowel Disease: A Nursing-Led Cross-Sectional Study of Patients in Clinical Remission. Medicina. 2020; 56(1):45. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56010045
Chicago/Turabian StyleMancina, Rosellina Margherita, Raffaele Pagnotta, Caterina Pagliuso, Vincenzo Albi, Daniela Bruno, Pietro Garieri, Patrizia Doldo, and Rocco Spagnuolo. 2020. "Gastrointestinal Symptoms of and Psychosocial Changes in Inflammatory Bowel Disease: A Nursing-Led Cross-Sectional Study of Patients in Clinical Remission" Medicina 56, no. 1: 45. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56010045