The Influence of Gender and Year of Study on Stress Levels and Coping Strategies among Polish Dental

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
2.3. Statistical Procedures
3. Results
4. Discussion
Limitations of this Study
5. Conclusions
Practical Application
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Alzahem, A.M.; Van Der Molen, H.T.; De Boer, B.J. Effectiveness of a Dental Students Stress Management Program. Heal. Prof. Educ. 2015, 1, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Alzahem, A.M.; Van Der Molen, H.T.; Alaujan, A.H.; De Boer, B.J. Stress management in dental students: A systematic review. Adv. Med Educ. Pr. 2014, 5, 167–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitter, M.; Liedl, M.; Beck, J.; Rammelsberg, P. Chronic stress in medical and dental education. Med. Teach. 2008, 30, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Gorter, R.C.; Freeman, R.; Hammen, S.; Murtomaa, H.; Blinkhorn, A.; Humphris, G. Psychological stress and health in undergraduate dental students: Fifth year outcomes compared with first year baseline results from five European dental schools. Eur. J. Dent. Educ. 2008, 12, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Alzahem, A.M.; Van Der Molen, H.T.; Alaujan, A.H.; Schmidt, H.G.; Zamakhshary, M.H. Stress amongst dental students: A systematic review. Eur. J. Dent. Educ. 2011, 15, 8–18. [Google Scholar] [CrossRef]
- Birks, Y.; Mckendree, J.; Watt, I. Emotional intelligence and perceived stress in healthcare students: A multi-institutional, multi-professional survey. BMC Med. Educ. 2009, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Stecker, T. Well-being in an academic environment. Med. Educ. 2004, 38, 465–478. [Google Scholar] [CrossRef] [Green Version]
- Cahill, L. Why sex matters for neuroscience. Nat. Rev. Neurosci. 2006, 7, 477–484. [Google Scholar] [CrossRef]
- Cosgrove, K.P.; Mazure, C.M.; Staley, J.K. Evolving Knowledge of Sex Differences in Brain Structure, Function, and Chemistry. Biol. Psychiatry 2007, 62, 847–855. [Google Scholar] [CrossRef] [Green Version]
- Calvarese, M. The Effect of Gender on Stress Factors: An Exploratory Study among University Students. Soc. Sci. 2015, 4, 1177–1184. [Google Scholar] [CrossRef] [Green Version]
- Cohn, A.; Zeichner, A. Effects of masculine identity and gender role stress on aggression in men. Psychol. Men Masc. 2006, 7, 179–190. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Wong, J.G.W.S.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.-M.; Wong, P.-C.; Tsang, K.W.T.; Chua, S.E. Stress and Psychological Distress among SARS Survivors 1 Year after the Outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juczyn’ski, Z.; Ogiń ´ska-Bulik, N. Narze˛dzia Pomiaru Stresu I Radzenia Sobie Ze Stresem; Pracownia Testów Psychologicznych: Warsaw, Poland, 2009. [Google Scholar]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef]
- Debkowska, K.; Kłosiewicz-Górecka, U.; Szyman’ska, A.; Waz˙niewski, P.; Zybertowicz, K. Akademickos´C´Polskich Miast; Polski Instytut Ekonomiczny: Warsaw, Poland, 2019. [Google Scholar]
- Saddki, N.; Sukerman, N.; Mohamad, D. Association between Emotional Intelligence and Perceived Stress in Undergraduate Dental Students. Malays. J. Med Sci. 2017, 24, 59–68. [Google Scholar] [CrossRef]
- Jowkar, Z.; Masoumi, M.; Mahmoodian, H. Psychological Stress and Stressors among Clinical Dental Students at Shiraz School of Dentistry, Iran. Adv. Med Educ. Pr. 2020, 11, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, S.T.; Kritz-Silverstein, D. A Longitudinal Study of Stress in First-Year Dental Students. J. Dent. Educ. 2010, 74, 836–848. [Google Scholar] [CrossRef] [PubMed]
- Ersan, N.; Dölekoğlu, S.; Fişekçioğlu, E.; Ilgüy, M.; Oktay, I. Perceived sources and levels of stress, general self-efficacy and coping strategies in preclinical dental students. Psychol. Heal. Med. 2017, 23, 567–577. [Google Scholar] [CrossRef]
- Sánchez-Conde, P.; Beltrán-Velasco, A.I.; Clemente-Suárez, V.J. Influence of psychological profile in autonomic response of nursing students in their first hospital clinical stays. Physiol. Behav. 2019, 207, 99–103. [Google Scholar] [CrossRef]
- Cohen, S.; Williamson, G.M. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage: Newbury Park, CA, USA, 1988; pp. 31–67. [Google Scholar]
- Ciacci, C.; Carpinelli, L.; Savarese, G. Perceived stress and bruxism in university students. BMC Res. Notes 2016, 9, 514. [Google Scholar] [CrossRef] [Green Version]
- Al-Sowygh, Z.H. Academic distress, perceived stress and coping strategies among dental students in Saudi Arabia. Saudi Dent. J. 2013, 25, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinurova, E.; Dehart, R.M. Perceived Stress, Stressors, and Coping Mechanisms among PGY1 Pharmacy Residents. Am. J. Pharm. Educ. 2018, 82, 6574. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Adrados, A.; Fernández-Martínez, S.; Martínez-Pascual, B.; Gonzalez-De-Ramos, C.; Fernández-Elías, V.E.; Clemente-Suárez, V.J. Psychophysiological stress response of physiotherapy last year students in his final degree dissertation. Physiol. Behav. 2020, 222, 112928. [Google Scholar] [CrossRef] [PubMed]
- Uraz, A.; Tocak, Y.S.; Yozgatlıgil, C.; Cetiner, S.; Bal, B. Psychological Well-Being, Health, and Stress Sources in Turkish Dental Students. J. Dent. Educ. 2013, 77, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Alsaleh, S.; Almadi, E.; Al-Angari, N.S.; Al-Shehri, H.A.; Shukri, M.M. Survey of perceived stress-inducing problems among dental students, Saudi Arabia. Saudi Dent. J. 2010, 22, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Divaris, K.; Mafla, A.C.; Villa-Torres, L.; Sánchez-Molina, M.; Gallego-Gómez, C.L.; Vélez-Jaramillo, L.F.; Tamayo-Cardona, J.A.; Pérez-Cepeda, D.; Vergara-Mercado, M.L.; Simancas-Pallares, M.; et al. Psychological distress and its correlates among dental students: A survey of 17 Colombian dental schools. BMC Med. Educ. 2013, 13, 91. [Google Scholar] [CrossRef] [Green Version]
- Takayama, Y.; Miura, E.; Miura, K.; Ono, S.; Ohkubo, C. Condition of depressive symptoms among Japanese dental students. Odontology 2011, 99, 179–187. [Google Scholar] [CrossRef]
- Basudan, S.; Binanzan, N.; Alhassan, A. Depression, anxiety and stress in dental students. Int. J. Med. Educ. 2017, 8, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Pau, A.; Rowland, M.L.; Naidoo, S.; Abdulkadir, R.; Makrynika, E.; Moraru, R.; Huang, B.; Croucher, R. Emotional Intelligence and Perceived Stress in Dental Undergraduates: A Multinational Survey. J. Dent. Educ. 2007, 71, 197–204. [Google Scholar] [CrossRef]
- Pau, A.K.; Croucher, R. Emotional Intelligence and Perceived Stress in Dental Undergraduates. J. Dent. Educ. 2003, 67, 1023–1028. [Google Scholar] [CrossRef]
- Polychronopoulou, A.; Divaris, K. Perceived Sources of Stress among Greek Dental Students. J. Dent. Educ. 2005, 69, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Ghafoor, S.; Chaudhry, S.; Khan, J.S. Marital Status as a Stress Indicator in Postgraduate Dental Students. J. Pak. Med. Assoc. 2019, 70, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Mocny-Pachońska, K.; Łanowy, P.; Trzcionka, A.; Skaba, D.; Tanasiewicz, M. Gender related changes of empathy level among Polish dental students over the course of training. Medicine 2020, 99, e18470. [Google Scholar] [CrossRef] [PubMed]
- Mocny-Pachońska, K.; Doniec, R.; Trzcionka, A.; Pachoński, M.; Piaseczna, N.; Sieciński, S.; Osadcha, O.; Łanowy, P.; Tanasiewicz, M. Evaluating the stress-response of dental students to the dental school environment. PeerJ 2020, 8, e8981. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PSS-10 | 1–10 | Item Elimination | ||||
|---|---|---|---|---|---|---|
| Year | Group | α | αst | Rav | Item | α |
| I | Total | 0.851 | 0.850 | 0.361 | 7 | 0.855 |
| Female | 0.826 | 0.825 | 0.320 | 7 | 0.831 | |
| Male | 0.898 | 0.898 | 0.468 | 7 | 0.900 | |
| II | Total | 0.878 | 0.879 | 0.420 | 7 | 0.881 |
| Female | 0.881 | 0.880 | 0.424 | 7 | 0.887 | |
| Male | 0.860 | 0.863 | 0.386 | − | − | |
| III | Total | 0.834 | 0.831 | 0.330 | 4 | 0.835 |
| Female | 0.822 | 0.819 | 0.312 | 4 | 0.827 | |
| Male | 0.863 | 0.862 | 0.384 | 6 | 0.890 | |
| IV | Total | 0.862 | 0.864 | 0.388 | − | − |
| Female | 0.872 | 0.873 | 0.407 | 7 | 0.873 | |
| Male | 0.838 | 0.841 | 0.346 | 4 | 0.840 | |
| V | Total | 0.884 | 0.885 | 0.434 | 7 | 0.884 |
| Female | 0.843 | 0.841 | 0.346 | − | − | |
| Male | 0.906 | 0.911 | 0.505 | 10 | 0.913 | |
| I-V | Total | 0.865 | 0.865 | 0.391 | − | − |
| Female | 0.851 | 0.851 | 0.363 | 7 | 0.855 | |
| Male | 0.879 | 0.880 | 0.424 | − | − | |
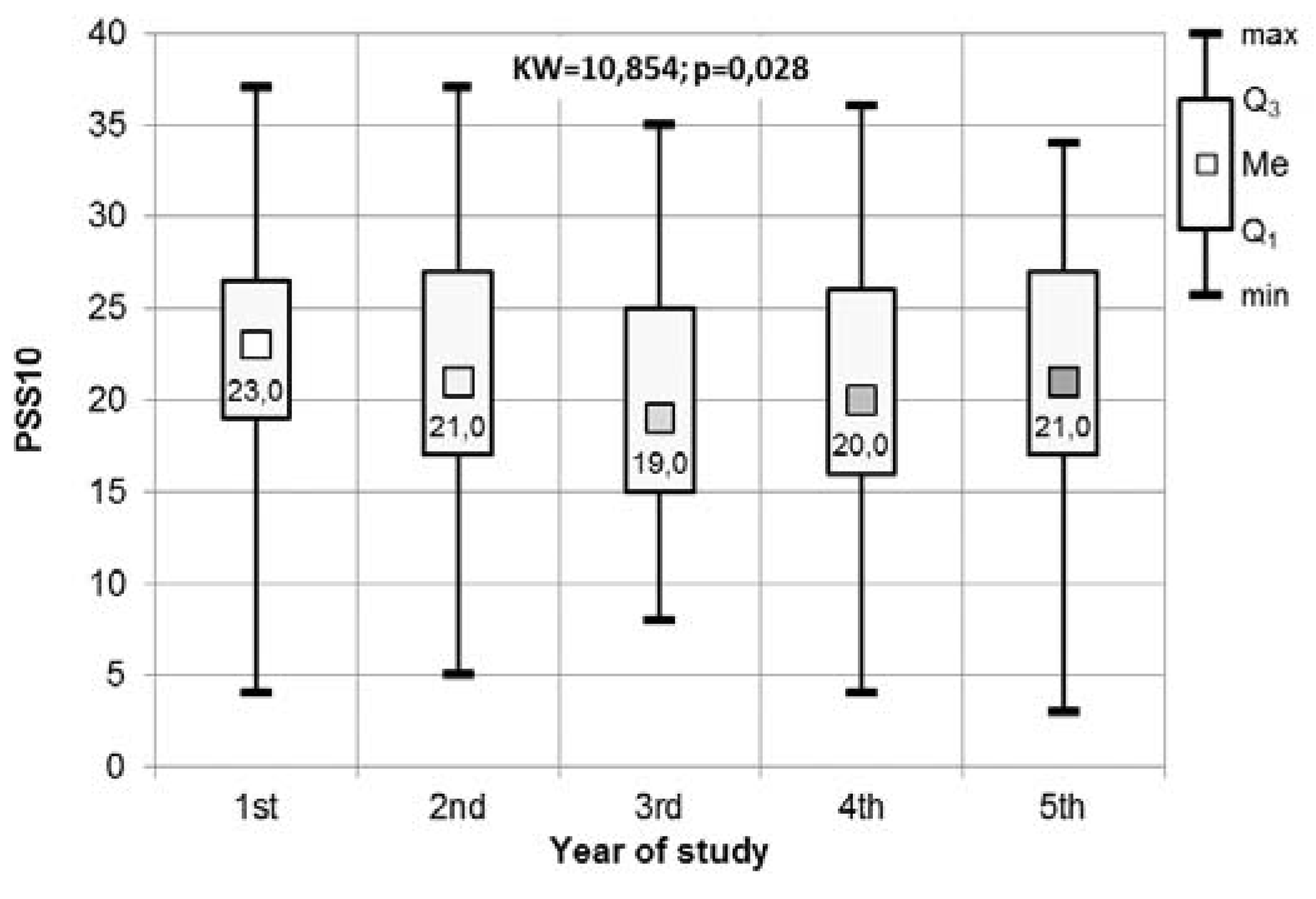
| Year of Study | ||||||
|---|---|---|---|---|---|---|
| PSS-10 | 1st | 2nd | 3rd | 4th | 5th | Total |
| Min | 4 | 5 | 8 | 4 | 3 | 3 |
| Q1 | 19 | 17 | 15 | 16 | 17 | 16.25 |
| Me | 23 | 21 | 19 | 20 | 21 | 21 |
| Q3 | 26.5 | 27 | 25 | 26 | 27 | 26 |
| Max | 37 | 37 | 35 | 36 | 34 | 37 |
| Dunn-Bonferroni | ||||||
| Conover | Year | I | II | III | IV | V |
| I | 0.47 | 0.008 | 0.12 | 0.83 | ||
| II | 0.08 | 0.50 | 1.00 | 1.00 | ||
| III | 0.01 | 0.08 | 1.00 | 0.30 | ||
| IV | 0.04 | 0.29 | 0.16 | 1.00 | ||
| V | 0.11 | 0.39 | 0.06 | 0.21 | ||
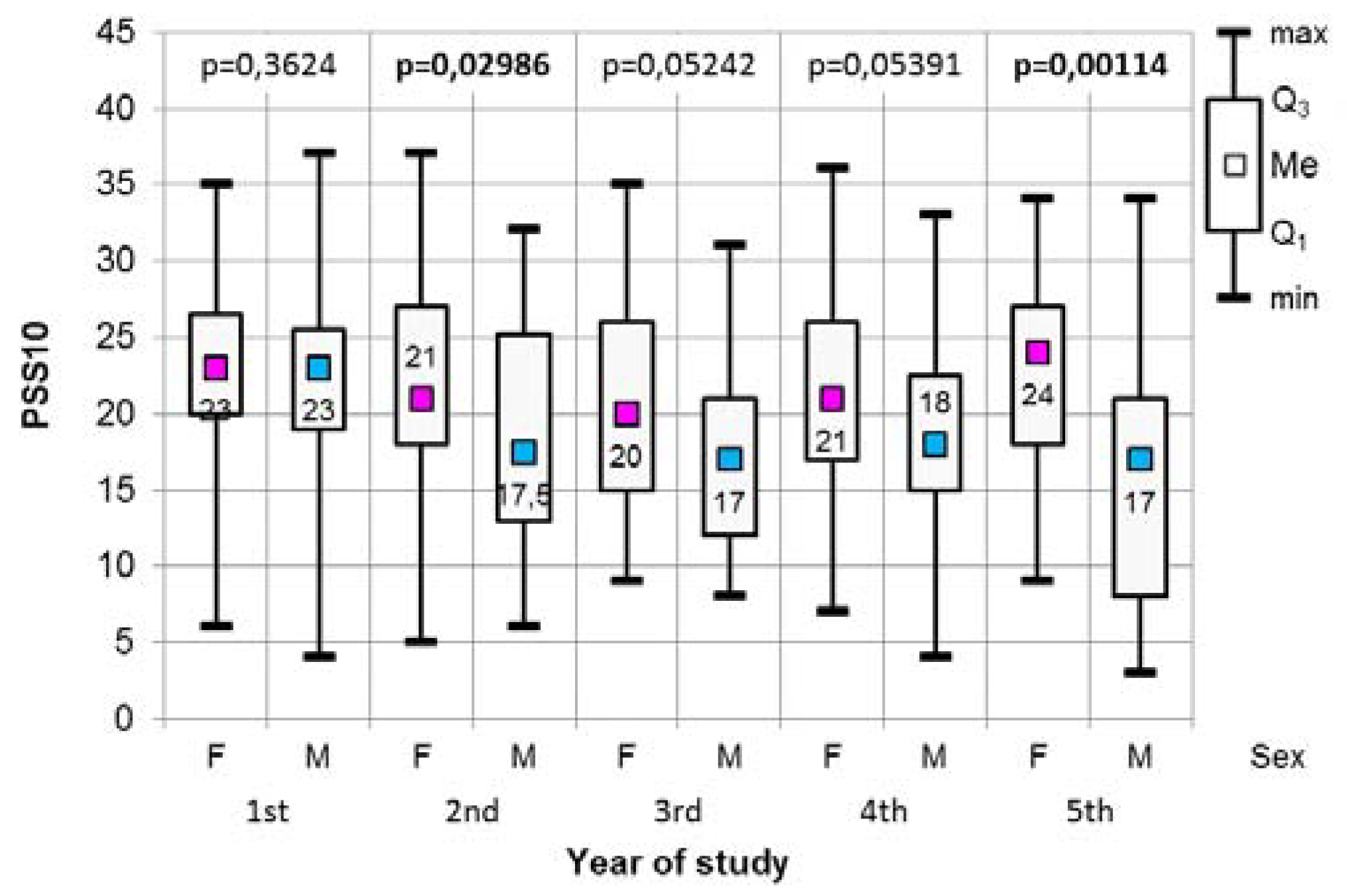
| Strategies | Female | Male | p | |
|---|---|---|---|---|
| First year of study | ||||
| 6: Turning to Religion | Median | 0.5 | 0.0 | 0.007 |
| Quartiles | 0.0–1.5 | 0.0–0.6 | ||
| Min-Max | 0.0–3.0 | 0.0–2.0 | ||
| 7: Seeking emotional support | Median | 2.5 | 2.0 | 0.046 |
| Quartiles | 1.5–2.5 | 1.5–2.5 | ||
| Min-Max | 0.0-3.0 | 0.0–3.0 | ||
| 8: Seeking instrumental support | Median | 2.0 | 2.0 | 0.045 |
| Quartiles | 1.5–3.0 | 1.0–2.0 | ||
| Min-Max | 0.0-3.0 | 0.5–3.0 | ||
| 9: Dealing with something else | Median | 2.0 | 1.5 | 0.029 |
| Quartiles | 1.0–2.0 | 1.0–1.6 | ||
| Min-Max | 0.0–3.0 | 0.0-2.5 | ||
| Second year of study | ||||
| 5: Sense of humor | Median | 1.0 | 1.3 | 0.033 |
| Quartiles | 0.5–1.5 | 0.5–2.0 | ||
| Min-Max | 0.0–3.0 | 0.0–3.0 | ||
| 8: Seeking instrumental support | Median | 2.0 | 1.8 | 0.018 |
| Quartiles | 1.5–2.5 | 1.0–2.5 | ||
| Min-Max | 0.5–3.0 | 0.5–2.5 | ||
| 11: Venting of emotions | Median | 1.5 | 1.5 | 0.005 |
| Quartiles | 1.5–2.0 | 1.0–1.6 | ||
| Min-Max | 0.0–3.0 | 0.5–3.0 | ||
| 12: Use of psychoactive substances | Median | 0.0 | 1.0 | 0.004 |
| Quartiles | 0.0–1.0 | 0.0–2.0 | ||
| Min-Max | 0.0–3.0 | 0.0-2.5 | ||
| 14: Self blame | Median | 2.0 | 1.25 | 0.046 |
| Quartiles | 1.0–2.0 | 1.0–2.0 | ||
| Min-Max | 0.0–3.0 | 0.0–2.5 | ||
| Third year of study | ||||
| 5: Sense of humor | Median | 1.0 | 1.5 | 0.043 |
| Quartiles | 0.5–1.5 | 0.6–2.0 | ||
| Min-Max | 0.0–3.0 | 0.0–2.5 | ||
| 10: Denial | Median | 0.5 | 0.25 | 0.029 |
| Quartiles | 0.0–0.5 | 0.0–1.0 | ||
| Min-Max | 0.0–3.0 | 0.0–2.0 | ||
| 14: Self blame | Median | 1.5 | 1.0 | 0.001 |
| Quartiles | 1.0–2.0 | 1.0–1.3 | ||
| Min-Max | 0.0–3.0 | 0.0–2.5 | ||
| Fourth year of study | ||||
| 6: Turning on Religion | Median | 1.0 | 0.0 | 0.04 |
| Quartiles | 0.0–1.8 | 0.0–1.7 | ||
| Min-Max | 0.0–3.0 | 0.0–3.0 | ||
| 7: Seeking emotional support | Median | 2.5 | 2.0 | 0.01 |
| Quartiles | 1.5–3.0 | 1.0–2.0 | ||
| Min-Max | 0.5–3.0 | 0.0–3.0 | ||
| 8: Seeking instrumental support | Median | 2.0 | 2.0 | 0.008 |
| Quartiles | 1.5–3.0 | 1.5–2.0 | ||
| Min-Max | 0.0–3.0 | 0.0–2.5 | ||
| 11: Venting of emotions | Median | 2.0 | 1.5 | 0.04 |
| Quartiles | 1.5–2.0 | 1.3–2.0 | ||
| Min-Max | 0.0–3.0 | 0.5–2.5 | ||
| Strategies | Year of Study | Total | |||||
|---|---|---|---|---|---|---|---|
| 1st | 2nd | 3rd | 4th | 5th | |||
| 1: Active coping | r* | −0.004 | 0.078 | 0.015 | −0.124 | −0.010 | −0.009 |
| p | 0.973 | 0.448 | 0.903 | 0.237 | 0.921 | 0.845 | |
| 2: Planning | r | 0.355 | –0.031 | −0.615 | 0.590 | 0.163 | 0.130 |
| p | 0.001 | 0.764 | <0.001 | <0.001 | 0.118 | 0.006 | |
| 3: Positive reappraisal | r | 0.026 | 0.203 | 0.281 | 0.137 | 0.327 | 0.199 |
| p | 0.807 | 0.046 | 0.018 | 0.190 | 0.001 | <0.001 | |
| 4: Acceptance | r | 0.304 | 0.256 | 0.337 | 0.337 | 0.220 | 0.279 |
| p | 0.003 | 0.011 | 0.004 | 0.001 | 0.034 | <0.001 | |
| 5: Sense of humor | r | 0.108 | 0.443 | 0.389 | 0.303 | 0.219 | 0.287 |
| p | 0.309 | <0.001 | 0.001 | 0.003 | 0.035 | <0.001 | |
| 6: Turning to Religion | r | 0.021 | 0.025 | 0.083 | −0.061 | 0.179 | 0.047 |
| p | 0.844 | 0.810 | 0.492 | 0.562 | 0.086 | 0.317 | |
| 7: Seeking emotional support | r | −0.048 | 0.090 | −0.093 | −0.145 | −0.089 | −0.053 |
| p | 0.651 | 0.377 | 0.439 | 0.165 | 0.398 | 0.261 | |
| 8: Seeking instrumental support | r | 0.228 | 0.274 | 0.248 | 0.061 | 0.142 | 0.185 |
| p | 0.030 | 0.006 | 0.037 | 0.562 | 0.175 | <0.001 | |
| 9: Dealing with something else | r | 0.047 | −0.071 | 0.169 | 0.167 | 0.279 | 0.121 |
| p | 0.656 | 0.486 | 0.158 | 0.110 | 0.007 | 0.011 | |
| 10: Denial | r | 0.105 | 0.135 | 0.069 | 0.071 | 0.153 | 0.116 |
| p | 0.320 | 0.184 | 0.568 | 0.497 | 0.144 | 0.014 | |
| 11: Venting of emotions | r | 0.216 | 0.183 | 0.140 | 0.267 | 0.209 | 0.205 |
| p | 0.040 | 0.072 | 0.244 | 0.010 | 0.044 | <0.001 | |
| 12: Use of psychoactive substances | r | 0.383 | 0.206 | 0.310 | 0.197 | 0.283 | 0.265 |
| p | <0.001 | 0.042 | 0.008 | 0.059 | 0.006 | <0.001 | |
| 13: Suppression of activities | r | 0.244 | −0.060 | 0.088 | 0.118 | 0.360 | 0.152 |
| p | 0.020 | 0.560 | 0.465 | 0.260 | <0.001 | 0.001 | |
| 14: Self blame | r | 0.272 | −0.040 | −0.165 | 0.277 | 0.321 | 0.160 |
| p | 0.009 | 0.694 | 0.170 | 0.007 | 0.002 | 0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mocny-Pachońska, K.; Trzcionka, A.; Doniec, R.J.; Sieciński, S.; Tanasiewicz, M. The Influence of Gender and Year of Study on Stress Levels and Coping Strategies among Polish Dental. Medicina 2020, 56, 531. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100531
Mocny-Pachońska K, Trzcionka A, Doniec RJ, Sieciński S, Tanasiewicz M. The Influence of Gender and Year of Study on Stress Levels and Coping Strategies among Polish Dental. Medicina. 2020; 56(10):531. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100531
Chicago/Turabian StyleMocny-Pachońska, Katarzyna, Agata Trzcionka, Rafał J. Doniec, Szymon Sieciński, and Marta Tanasiewicz. 2020. "The Influence of Gender and Year of Study on Stress Levels and Coping Strategies among Polish Dental" Medicina 56, no. 10: 531. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56100531