Usefulness of Antioxidants as Adjuvant Therapy for Septic Shock: A Randomized Clinical Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
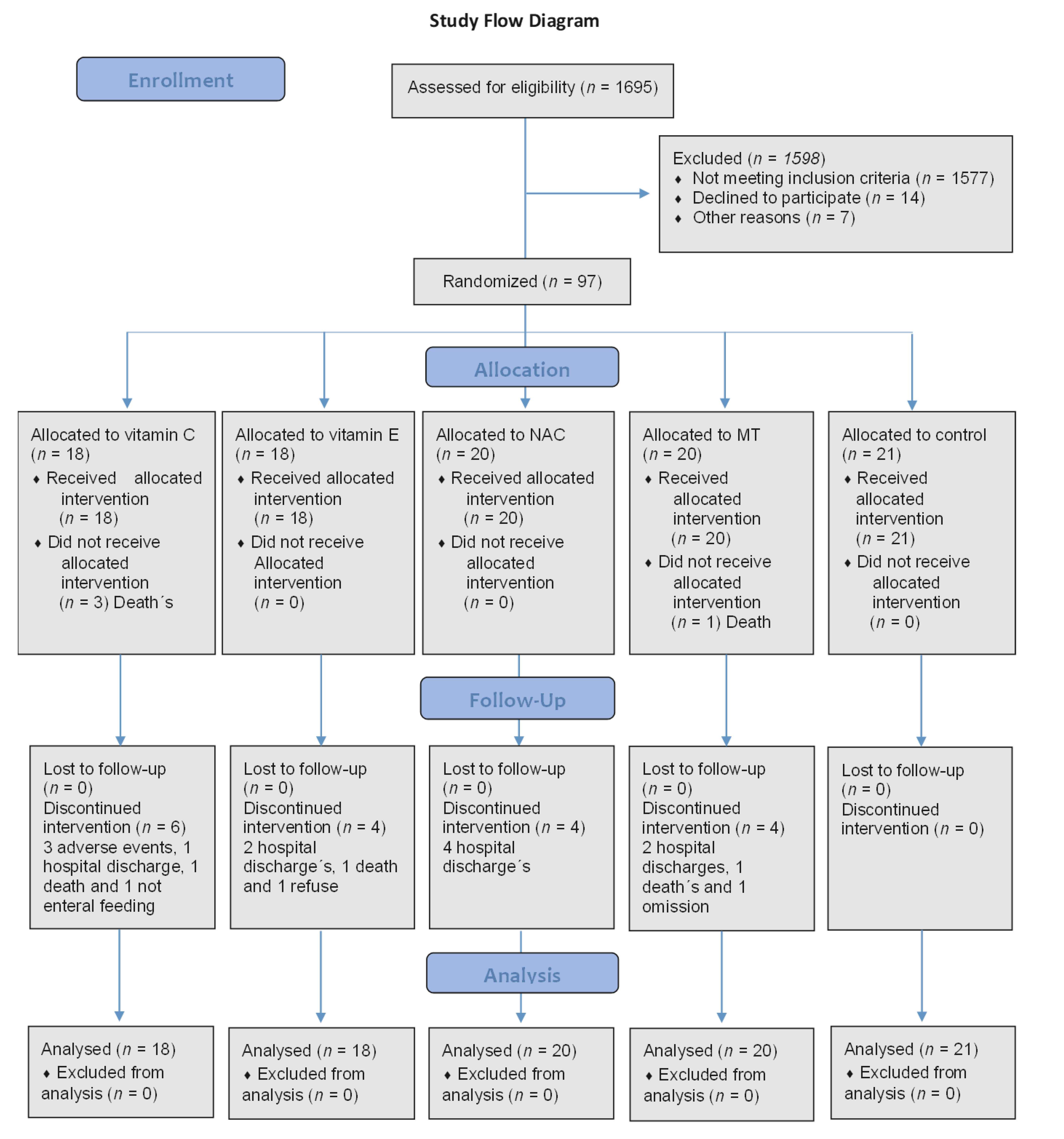
2.1. Study Population
2.2. Randomization, Masking, and Drug Administration
2.3. Standard Therapy at the ICU
2.4. Study Measurements and Procedures
2.5. Sampling for the Determination of Oxidative Stress and Antioxidant State
2.6. Sample Obtainment and Storage
2.7. Oxidative Stress Markers in Plasma
2.7.1. NO3−/NO2− Ratio
2.7.2. LPO Levels
2.7.3. GSH Concentration
2.7.4. Evaluation of TAC
2.7.5. Carbonylation Protein Concentration
2.7.6. Vitamin C Levels
2.8. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Treatments
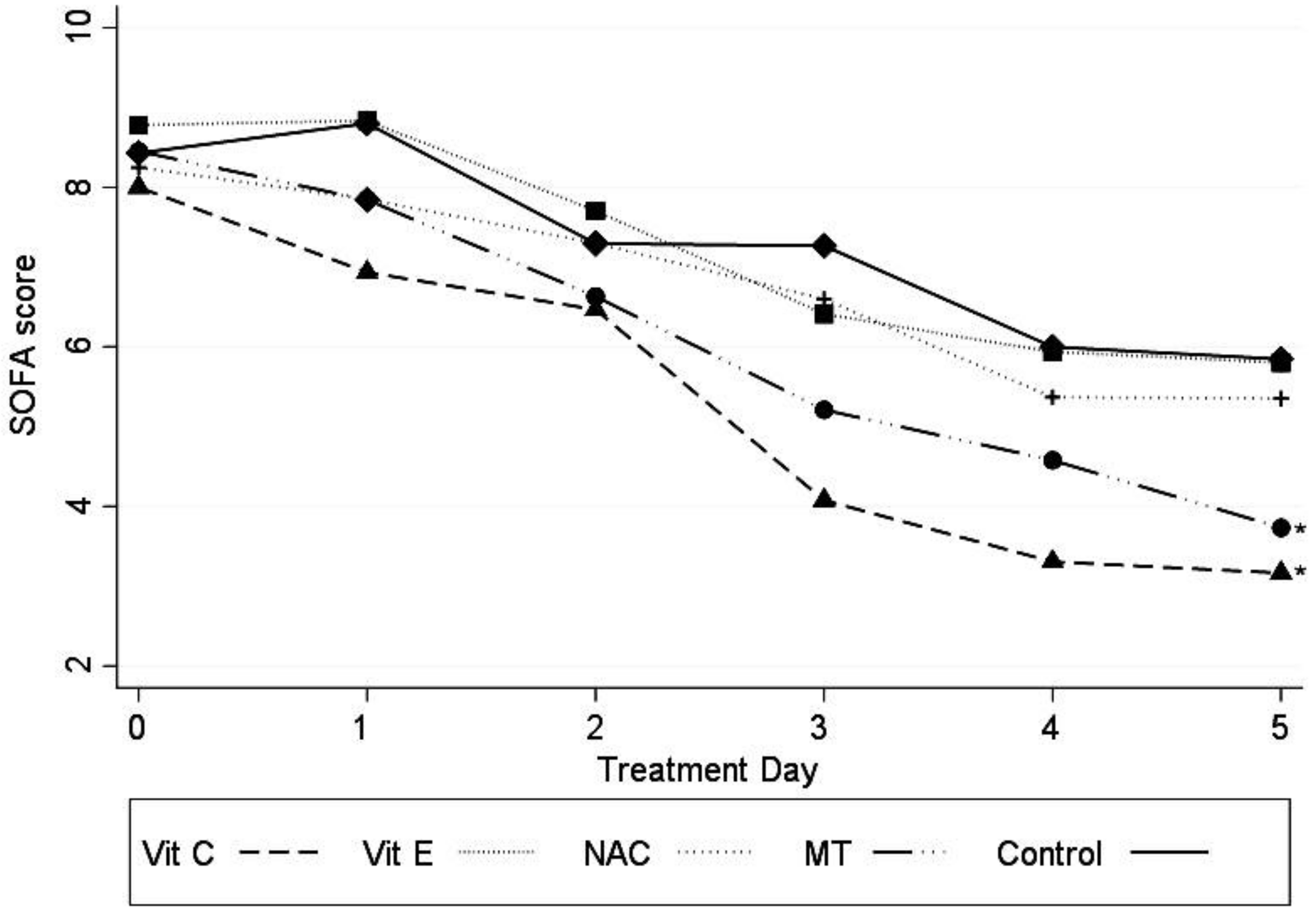
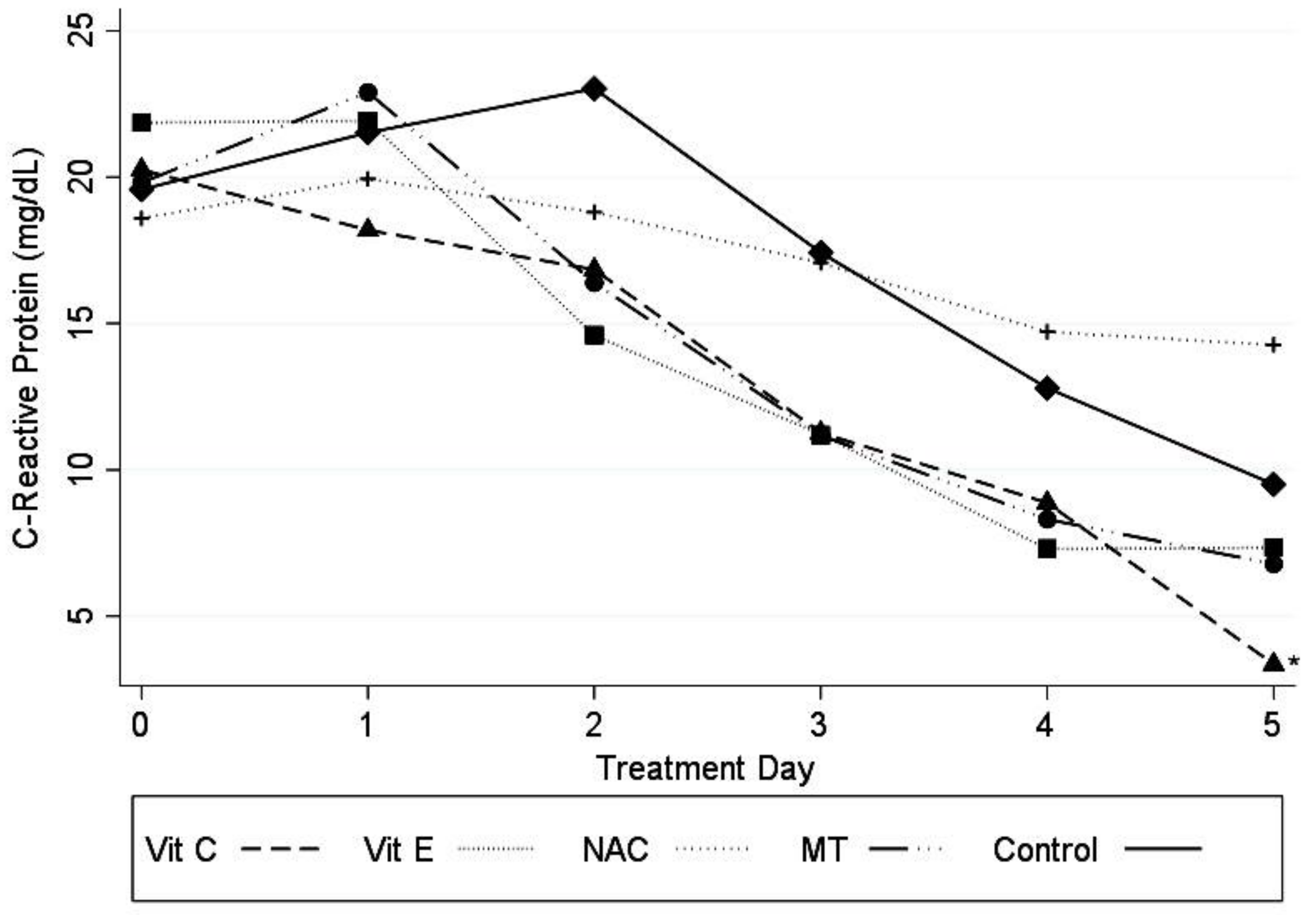
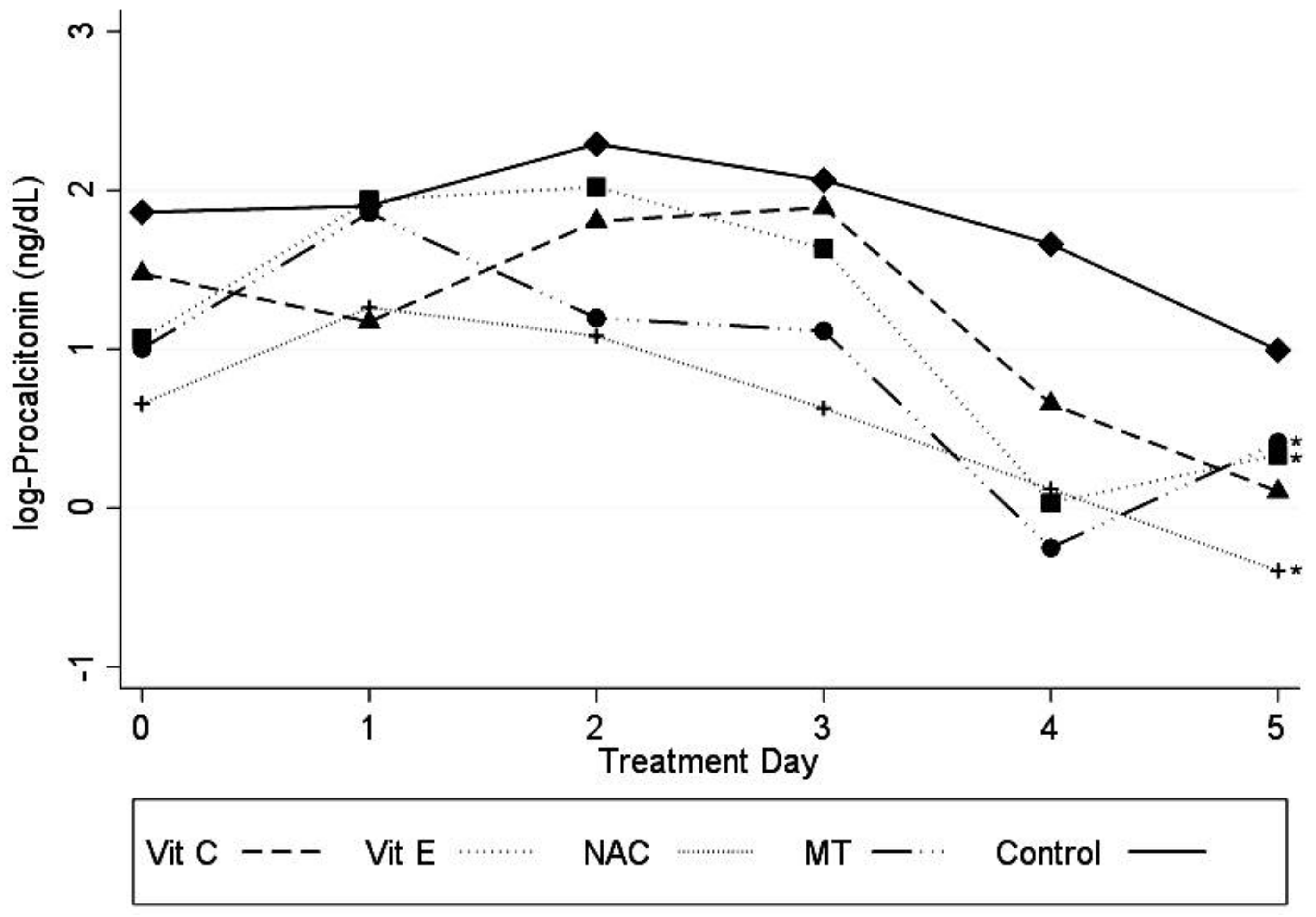
Primary Outcome
3.3. Undesired Side Effects
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Timsit, J.F.; Perner, A.; Bakker, J.; Bassetti, M.; Benoit, D.; Cecconi, M.; Curtis, J.R.; Doig, G.S.; Herridge, M.; Jaber, S.; et al. Year in review in intensive care Medicine 2014: III. Severe infections, septic shock, healthcare-associated infections, highly resistant bacteria, invasive fungal infections, severe viral infections, Ebola virus disease and paediatrics. Intensive. Care Med. 2015, 41, 575–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, J.C.; Vincent, J.L.; Guyatt, G.; Angus, D.C.; Abraham, E.; Bernard, G.; Bombardier, C.; Calandra, T.; Jørgensen, H.S.; Sylvester, R.; et al. Outcome measures for clinical research in sepsis: A report of the 2nd Cambridge Colloquium of the International Sepsis Forum. Crit. Care Med. 2005, 33, 1708–1716. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef]
- Pisoschi, A.M.; Pop, A. The role of antioxidants in the chemistry of oxidative stress: A review. Eur. J. Med. Chem. 2015, 97, 55–74. [Google Scholar] [CrossRef]
- Galley, H.F. Oxidative stress and mitochondrial dysfunction in sepsis. Br. J. Anaesth. 2011, 107, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crouser, E.D. Mitochondrial dysfunction in septic shock and multiple organ dysfunction syndrome. Mitochondrion 2004, 4, 729–741. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Guarner-Lans, V.; Soria-Castro, E.; Manzano-Pech, L.; Pérez-Torres, I. Is Antioxidant Therapy a Useful Complementary Measure for Covid-19 Treatment? An Algorithm for Its Application. Medicina 2020, 56, 386. [Google Scholar] [CrossRef] [PubMed]
- Chertoff, J. N-Acetylcysteine’s role in sepsis and potential benefit in patients with microcirculatory derangements. J. Intensive Care Med. 2018, 33, 87–96. [Google Scholar] [CrossRef]
- Rushworth, G.F.; Megson, I.L. Existing and potential therapeutic uses for N-acetylcysteine: The need for conversion to intracellular glutathione for antioxidant benefits. Pharmacol. Ther. 2014, 141, 150–159. [Google Scholar] [CrossRef]
- Rank, N.; Michel, C.; Haertel, C.; Lenhart, A.; Welte, M.; Meier-Hellmann, A.; Spies, C. N-acetylcysteine increases liver blood flow and improves liver function in septic shock patients: Results of a prospective, randomized, double-blind study. Crit. Care Med. 2000, 28, 3799–3807. [Google Scholar] [CrossRef]
- Spapen, H.D.; Diltoer, M.W.; Nguyen, D.N.; Hendrickx, I.; Huyghens, L.P. Effects of N-acetylcysteine on microalbuminuria and organ failure in acute severe sepsis: Results of a pilot study. Chest 2005, 127, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Calzetta, L.; Facciolo, F.; Rogliani, P.; Matera, M.G. Pharmacological investigation on the anti-oxidant and anti-inflammatory activity of N-acetylcysteine in an ex vivo model of COPD exacerbation. Respir. Res. 2017, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Paterson, R.L.; Galley, H.F.; Webster, N.R. The effect of N-acetylcysteine on nuclear factor-kappa B activation, interleukin-6, interleukin-8, and intercellular adhesion molecule-1 expression in patients with sepsis. Crit. Care Med. 2003, 31, 2574–2578. [Google Scholar] [CrossRef]
- Kim, J.C.; Hong, S.W.; Shim, J.K.; Yoo, K.J.; Chun, D.H.; Kwak, Y.L. Effect of N-acetylcysteine on pulmonary function in patients undergoing off-pump coronary artery bypass surgery. Acta Anaesthesiol. Scand. 2011, 55, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Oudemans-van, S.H.M. Vitamin C supplementation in the critically ill patient. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 193–201. [Google Scholar] [CrossRef]
- Spoelstra-de Man, A.M.E.; De Grooth, H.J.; Elbers, P.W.G.; Oudemans-van Straaten, H.M. Response to Adjuvant vitamin C in cardiac arrest patients undergoing renal replacement therapy: An appeal for a higher high-dose. Crit. Care 2018, 22, 350. [Google Scholar] [CrossRef] [Green Version]
- Fowler, A.A.; Syed, A.A.; Knowlson, S.; Sculthorpe, R.; Farthing, D.; DeWilde, C.; Farthing, C.A.; Larus, T.L.; Martin, E.; Brophy, D.F.; et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J. Transl. Med. 2014, 12, 32. [Google Scholar] [CrossRef] [Green Version]
- Traber, M.G.; Atkinson, J. Vitamin E, antioxidant and nothing more. Free. Radic. Biol. Med. 2007, 43, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Durant, R.; Klouche, K.; Delbosc, S.; Morena, M.; Amigues, L.; Beraud, J.J.; Canaud, B.; Cristol, J.P. Superoxide anion overproduction in sepsis: Effects of vitamin E and simvastatin. Shock 2004, 22, 34–39. [Google Scholar] [CrossRef]
- Galley, H.F.; Lowes, D.A.; Allen, L.; Cameron, G.; Aucott, L.S.; Webster, N.R. Melatonin as a potential therapy for sepsis: A phase I dose escalation study and an ex vivo whole blood model under conditions of sepsis. J. Pineal Res. 2014, 56, 427–438. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.M.; Chioléro, R.L. Antioxidant supplementation in sepsis and systemic inflammatory response syndrome. Crit. Care Med. 2007, 35, S584–S590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Sepsis definitions task force. Developing a new definition and assessing new clinical criteria for septic shock: For the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility, and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, Z.U.; Prasannan, P.; Moni, M.; Edathadathil, F.; Prasanna, P.; Menon, A.; Nair, S.; Greeshma, C.R.; Sathyapalan, D.T.; Menon, V.; et al. Vitamin C therapy for routine care in septic shock (ViCTOR) trial: Effect of intravenous vitamin C, thiamine, and hydrocortisone administration on inpatient mortality among patients with septic shock. Indian. J. Crit. Care. Med. 2020, 8, 653–661. [Google Scholar]
- Fowler, A.A.; Truwit, J.D.; Hite, R.D.; Morris, P.E.; DeWilde, C.; Priday, A.; Fisher, B.; Thacker, L.R.; Natarajan, R.; Brophy, D.F.; et al. Effect of vitamin c infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: The CITRIS-ALI randomized clinical trial. JAMA 2019, 322, 1261–1270. [Google Scholar] [CrossRef]
- Lowes, D.A.; Almawash, A.M.; Webster, N.R.; Reid, V.L.; Galley, H.F. Melatonin and structurally similar compounds have differing effects on inflammation and mitochondrial function in endothelial cells under conditions mimicking sepsis. Br. J. Anaesth. 2011, 107, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Howe, K.P.; Clochesy, J.M.; Goldstein, L.S.; Owen, H. Mechanical ventilation antioxidant trial. Am. J. Crit. Care 2015, 24, 440–445. [Google Scholar] [CrossRef] [Green Version]
- Soto, M.E.; Manzano-Pech, L.G.; Guarner-Lans, V.; Díaz-Galindo, J.A.; Vásquez, X.; Castrejón-Tellez, V.; Gamboa, R.; Huesca, C.; Fuentevilla-Alvárez, G.; Pérez-Torres, I. Oxidant/antioxidant profile in the thoracic aneurysm of patients with the Loeys-Dietz syndrome. Oxidative Med. Cell. Longev. 2020, 2020, 5392454. [Google Scholar] [CrossRef]
- Zhang, R.; Wang, X.; Ni, L.; Di, X.; Ma, B.; Niu, S.; Liu, C.; Reiter, R.J. COVID-19: Melatonin as a potential adjuvant treatment. Life Sci. 2020, 250, 117583. [Google Scholar] [CrossRef]
- Marik, P.E. Hydrocortisone, ascorbic acid and thiamine (HAT Therapy) for the treatment of sepsis. Focus on ascorbic acid. Nutrients 2018, 10, 1762. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Rosengrave, P.C.; Bayer, S.; Chambers, S.; Mehrtens, J.; Shaw, G.M. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care 2017, 21, 300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans-Olders, R.; Eintracht, S.; Hoffer, L.J. Metabolic origin of hypovitaminosis C in acutely hospitalized patients. Nutrition 2010, 26, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joo, Y.M.; Chae, M.K.; Hwang, S.Y.; Jin, S.C.; Lee, T.R.; Cha, W.C.; Jo, I.J.; Sim, M.S.; Song, K.J.; Jeong, Y.K.; et al. Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department. Clin. Exp. Emerg. Med. 2014, 1, 35–40. [Google Scholar] [CrossRef]
- Hwang, S.Y.; Park, J.E.; Jo, I.J.; Kim, S.; Chung, S.P.; Kong, T.; Shin, J.; Lee, H.J.; You, K.M.; Jo, Y.H.; et al. Combination therapy of vitamin C and thiamine for septic shock in a multicentre, double-blind, randomized, controlled study (ATESS): Study protocol for a randomized controlled trial. Trials 2019, 20, 420. [Google Scholar] [CrossRef]
- Mitchell, A.B.; Ryan, T.E.; Gillion, A.R.; Wells, L.D.; Muthiah, M.P. Vitamin C and thiamine for sepsis and septic shock. Am. J. Med. 2020, 133, 635–638. [Google Scholar] [CrossRef]
- Boretti, A.; Banik, B.K. Intravenous vitamin C for reduction of cytokines storm in acute respiratory distress syndrome. PharmaNutrition 2020, 12, 100190. [Google Scholar] [CrossRef]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of vitamin C, hydrocortisone, and thiamine vs hydrocortisone alone on time alive and free of vasopressor support among patients with septic shock: The Vitamins Randomized Clinical Trial. JAMA 2020, 323, 423–431. [Google Scholar] [CrossRef]
- Marik, P.E.; Khangoora, V.; Rivera, R. Hydrocortisone, vitamin C and thiamine for the treatment of severe sepsis and septic shock: A retrospective before-after study. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in influenza, Covid-19, and other viral infections. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef]
- Carrillo-Vico, A.; Lardone, P.J.; Naji, L.; Fernández-Santos, J.M.; Martín-Lacave, I.; Guerrero, J.M.; Calvo, J.R. Beneficial pleiotropic actions of melatonin in an experimental model of septic shock in mice: Regulation of pro-/anti-inflammatory cytokine network, protection against oxidative damage and anti-apoptotic effects. J. Pineal Res. 2005, 39, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Chiao, C.W.; Hsiao, G.; Chen, A.; Yen, M.H. Melatonin prevents endotoxin-induced circulatory failure in rats. J. Pineal Res. 2001, 30, 147–156. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, L.A.; Mistraletti, G.; Longhi, D.; Piva, I.R.; Marrazzo, F.; Villa, C.; Tozzi, M.; Paroni, R.; Finati, E.; Lapichino, G. Melatonin blood values and total antioxidant capacity in critically ill patients. Crit. Care 2014, 18, P436. [Google Scholar]
- Wang, H.; Wei, W.; Shen, Y.X.; Dong, C.; Zhang, L.L.; Wang, N.P.; Yue, L.; Xu, S.-Y. Protective effect of melatonin against liver injury in mice induced by Bacillus Calmette-Guerin plus lipopolysaccharide. World J. Gastroenterol. 2004, 10, 2690–2696. [Google Scholar] [CrossRef] [PubMed]
- Li, V.G.; Musumeci, T.; Pignatello, R.; Murabito, P.; Barbagallo, I.; Carbone, C.; Gullo, A.; Puglisi, G. Antioxidant potential of different melatonin-loaded nanomedicines in an experimental model of sepsis. Exp. Biol. Med. 2012, 237, 670–677. [Google Scholar]
- Sánchez-Barceló, E.J.; Mediavilla, M.D.; Tan, D.X.; Reiter, R.J. Clinical uses of melatonin: Evaluation of human trials. Curr. Med. Chem. 2010, 17, 2070–2095. [Google Scholar] [CrossRef]
- Lassnigg, A.; Punz, A.; Barker, R.; Keznickl, P.; Manhart, N.; Roth, E.; Hiesmayr, M. Influence of intravenous vitamin E supplementation in cardiac surgery on oxidative stress: A double-blinded, randomized, controlled study. Br. J. Anaesth. 2003, 90, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Prauchner, C.A. Oxidative stress in sepsis: Pathophysiological implications justifying antioxidant co-therapy. Burns 2017, 43, 471–485. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Vit C (n = 18) | Vit E (n = 18) | NAC (n = 20) | MT (n = 20) | C (n = 21) |
|---|---|---|---|---|---|
| Age (median, min–max) | 62 (22–95) | 65.5 (22–91) | 67.5 (18–95) | 62.5 (46–95) | 76 (51–89) |
| Weight kg (median, min–max) | 71 (33–112) | 71.5 (40–120) | 69.5 (39–95) | 67 (50–106) | 68 (50–105) |
| BM weight/height2 (median, min–max) | 25.4 (14.7–40.4) | 25 (15.1–41.4) | 22.45 (16.5–0.3) | 25.35 (17.3–52) | 25.4 (19.6–58) |
| Gender (%) | |||||
| Men | 6 (6.19) | 12 (12.37) | 11 (11.34) | 10 (10.31) | 10 (10.31) |
| Women | 12 (12.37) | 6 (6.19) | 9 (9.28) | 10 (10.31) | 11 (11.34) |
| Chronic health condition (%) | |||||
| Diabetes Mellitus | 4 (4.12) | 4 (4.12) | 3 (3.09) | 5 (5.15) | 6 (6.19) |
| Hypertension | 6 (6.19) | 8 (8.25) | 9 (9.28) | 7 (7.22) | 11 (11.34) |
| Cancer | 5 (5.15) | 9 (9.28) | 7 (7.22) | 7 (7.22) | 11 (11.34) |
| Chronic renal failure | 1 (1.03) | 2 (2.03) | 4 (4.12) | 3 (3.09) | 2 (2.06) |
| Admission source (%) | |||||
| Emergency department | 9 (9.28) | 12 (13.37) | 10 (10.31) | 14 (14.43) | 9 (9.28) |
| Operating room | 4 (4.12) | 2 (2.06) | 3 (3.09) | 2 (2.06) | 4 (4.12) |
| Inpatient ward transfer | 3 (3.09) | 4 (4.12) | 7 (7.22) | 4 (4.12) | 7 (7.22) |
| Other | 2 (2.06) | 0 | 0 | 0 | 1 (1.03) |
| Primary site of infection (%) | |||||
| Pulmonary | 7 (7.37) | 9 (9.97) | 9 (9.97) | 8 (8.42) | 6 (6.32) |
| Gastrointestinal | 7 (7.37) | 3 (3.16) | 4 (4.21) | 3 (3.16) | 9 (9.97) |
| Urinary | 2 (2.11) | 2 (2.11) | 5 (5.26) | 5 (5.26) | 3 (3.16) |
| CNS | 0 | 2 (2.11) | 0 | 0 | 1 (1.05) |
| Blood | 0 | 1 (1.05) | 0 | 2 (2.11) | 0 |
| Physiological variables 24 h | |||||
| before randomization | |||||
| (median, min–max) | |||||
| White blood cell count × 103/μL | 11 (5.1–39.9) | 10.8 (0.4–25.4) | 8.6 (0–32.5) | 11.7 (5.2–29.6) | 12 (0.9–49.8) |
| Platelet count × 103/μL | 256 (7–409) | 158 (10–363) | 155 (22–470) | 187.5 (29–543) | 225 (24–436) |
| Lactate (mmol/L) | 1.65 (0–4.8) | 2.1 (0.82–10.5) | 1.74 (0.99–7.8) | 2.27 (1–17) | 2.52 (1.1–12.4) |
| Serum creatinine (mg/dL) | 0.9 (0.5–5.5) | 1.35 (0.5–3.8) | 0.92 (0.5–6.6) | 1.27 (0.57–6.6) | 1.2 (0.5–5.2) |
| Bilirubin (mg/dL) | 0.75 (0.23–3.5) | 1.05 (0.35–4.4) | 0.80 (0.2–4) | 1.03 (0.17–3.7) | 1.15 (0.2–13.6) |
| PaO2/FiO2 (mmHg) | 168.5 (61–408) | 215 (39–271) | 146 (71–367) | 197 (57–261) | 197 (131–560) |
| C reactive protein (mg/dL) | 18.33 (1.9–1.4) | 20.12 (0.5–47) | 13.34 (0.02–6.7) | 21.75 (1.35–6.7) | 20.25 (1.36–5.3) |
| Procalcitonin (ng/dL) | 1.46 (0.16–321) | 2.92 (0.08–109) | 2.35 (0.06–95.5) | 2.32 (0.22–38.7) | 8.25 (0.08–100) |
| Intervention before randomization (%) | |||||
| Mechanical ventilation | 11 (11.58) | 9 (9.47) | 14 (14.47) | 12 (12.63) | 16 (16.84) |
| Vasopressors | 9 (9.38) | 7 (7.29) | 12 (12.50) | 9 (9.38) | 11 (11.46) |
| Norepinephrine | 0 | 1 (1.04) | 0 | 0 | 0 |
| Vasopressin | 8 (8.33) | 10 (10.42) | 8 (8.33) | 11 (11.46) | 10 (10.42) |
| Norepinephrine plus vasopressin | |||||
| Inotropes | |||||
| Dobutamine | 0 | 0 | 0 | 0 | 1 (1.04) |
| Levosimendan | 0 | 5 (5.21) | 1 (1.04) | 3 (3.13) | 5 (5.21) |
| Dopamine | 1 (1.04) | 0 | 0 | 1 (1.04) | 0 |
| Renal replacement Therapy | 1 (1.04) | 2 (2.08) | 2 (2.08) | 1 (1.04) | 3 (3.13) |
| Corticosteroid use before | |||||
| randomization during the study (%) | 6 (6.19) | 11 (11.34) | 9 (9.28) | 8 (8.25) | 10 (10.31) |
| SAPS II (median, min–max) | 38 (16–62) | 40 (24–73) | 38.5 (12–97) | 41.5 (13–73) | 40 (18–79) |
| APACHE III (median, min–max) | 13.5 (5–47) | 19 (11–33) | 14.5 (5–46) | 17 (6–39) | 15 (5–38) |
| SOFA score (median, min–max) | 8.5 (3–16) | 8.5 (5–14) | 8.5 (1–17) | 8 (3–14) | 8 (1–16) |
| Time from ICU admission to randomization hours (median, min–max) | 5 (1.5–70) | 6 (1–17) | 3 (1–140) | 9 (3–48) | - |
| Lipid Peroxidation (nM MDA/mL of Plasma) | |||
|---|---|---|---|
| Pre | Post | p | |
| Vit C (n = 18) | 3.44 (0.52–19.62) | 2.81 (0.23–8.70) | 0.14 |
| Vit E (n = 18) | 4.33 (1.25–15.25) | 3.24 (0.38–12.07) | 0.17 |
| NAC (n = 20) | 3.46 (0.23–9.49) | 3.46 (0.38–11.01) | 0.77 |
| MT (n = 20) | 2.13 (0.23–11.68) | 2.42 (0.23–7.11) | 0.04 |
| Control (n = 21) | 3.44 (0.52–9.49) | 3.90 (0.23–9.10) | 0.75 |
| NO3 + NO2 (µM/mL of plasma) | |||
| Pre | Post | p | |
| Vit C (n = 18) | 2.10 (0.98–2.73) | 1.49 (0.03–2.57) | <0.01 |
| Vit E (n = 18) | 1.79 (0.53–3.81) | 2.00 (0.76–5.65) | 0.36 |
| NAC (n = 20) | 2.43 (0.80–7.02) | 2.15 (0.01–8.16) | 0.81 |
| MT (n = 20) | 1.72 (0.67–4.77) | 1.32 (0.03–7.42) | 0.19 |
| Control (n = 21) | 2.25 (0.28–2.76) | 2.24 (0.01–7.22) | 0.97 |
| Total antioxidant capacity (nM/mL of plasma) | |||
| Pre | Post | p | |
| Vit C (n = 18) | 2226.2 (747.6–3053.4) | 2050.9 (966.6–2551.8) | 0.11 |
| Vit E (n = 18) | 2148.4 (886.3–3287.6) | 2223.1 (618.3–3841.9) | 0.90 |
| NAC (n = 20) | 1453.6 (621.5–2351.4) | 1951 (812.6–3528.7) | 0.05 |
| MT (n = 20) | 1999 (561.3–2519.2) | 1747.5 (456.5–2745.6) | 0.59 |
| Control (n = 21) | 2451.6 (1600–3467.1) | 2064.7 (312.4–3501) | 0.42 |
| Carbonylation (ng/mL of plasma) | |||
| Pre | Post | p | |
| Vit C (n = 18) | 48.85 (10.90–114.53) | 44.76 (12.72–98.17) | 0.59 |
| Vit E (n = 18) | 52.26 (27.27–137.25) | 42.723 (21.36–89.53) | 0.07 |
| NAC (n = 20) | 40.22 (22.27–89.99) | 41.13 (22.72–93.17) | 0.47 |
| MT (n = 20) | 74.76 (8.63–181.34) | 62.721 (29.99–142.25) | 0.40 |
| Control (n = 21) | 46.359 (9.99–106.80) | 44.08 (26.36–111.80) | 0.28 |
| GSH concentration (nM/mL of plasma) | |||
| Pre | Post | p | |
| Vit C (n = 18) | 0.10 (0.01–0.24) | 0.08 (0.01–0.20) | 0.50 |
| Vit E (n = 18) | 0.05 (0.00–0.30) | 0.07 (0.00–0.32) | 0.38 |
| NAC (n = 20) | 0.08 (0.00–0.54) | 0.10 (0.009–0.57) | 0.14 |
| MT (n = 20) | 0.07 (0.00–0.32) | 0.07 (0.010–0.51) | 0.64 |
| Control (n = 21) | 0.06 (0.03–0.20) | 0.05 (0.01–0.16) | 0.15 |
| Vit C (µM/mL of plasma) | |||
| Pre | Post | p | |
| Vit C (n = 18) | 0.17 (0.04–0.87) | 0.27 (0.06–0.99) | <0.01 |
| Vit E (n = 18) | 0.27 (0.08–0.99) | 0.26 (0.12–0.79) | 0.58 |
| NAC (n = 20) | 0.21 (0.09–0.61) | 0.18 (0.00–0.96) | 1.00 |
| MT (n = 20) | 0.21 (0.04–0.56) | 0.21 (0.04–0.43) | 0.83 |
| Control (n = 21) | 0.22 (0.08–0.77) | 0.19 (0.07–0.64) | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aisa-Alvarez, A.; Soto, M.E.; Guarner-Lans, V.; Camarena-Alejo, G.; Franco-Granillo, J.; Martínez-Rodríguez, E.A.; Gamboa Ávila, R.; Manzano Pech, L.; Pérez-Torres, I. Usefulness of Antioxidants as Adjuvant Therapy for Septic Shock: A Randomized Clinical Trial. Medicina 2020, 56, 619. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56110619
Aisa-Alvarez A, Soto ME, Guarner-Lans V, Camarena-Alejo G, Franco-Granillo J, Martínez-Rodríguez EA, Gamboa Ávila R, Manzano Pech L, Pérez-Torres I. Usefulness of Antioxidants as Adjuvant Therapy for Septic Shock: A Randomized Clinical Trial. Medicina. 2020; 56(11):619. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56110619
Chicago/Turabian StyleAisa-Alvarez, Alfredo, María Elena Soto, Verónica Guarner-Lans, Gilberto Camarena-Alejo, Juvenal Franco-Granillo, Enrique A. Martínez-Rodríguez, Ricardo Gamboa Ávila, Linaloe Manzano Pech, and Israel Pérez-Torres. 2020. "Usefulness of Antioxidants as Adjuvant Therapy for Septic Shock: A Randomized Clinical Trial" Medicina 56, no. 11: 619. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56110619