Five-Year Outcomes in Bariatric Surgery Patients


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
6. Limitations of Study
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Curtin, L.R. Prevalence and trends US adults 1999–2008. JAMA 2010, 303, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Barry, V.W.; Baruth, M.; Beets, M.W.; Durstine, J.L.; Liu, J.; Blair, S.N. Fitness vs. fatness on all-cause mortality: A meta-analysis. Prog. Cardiovasc. Dis. 2014, 56, 382–390. [Google Scholar] [CrossRef]
- Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900,000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [Green Version]
- Jia, H.; Lubetkin, E.I. The impact of obesity on health-related quality-of-life in the general adult US population. J. Public Health 2005, 27, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Bjelović, M. Hirurško lečenje klinički teške gojaznosti. Medicinski Glas. Inst. Štitastu Žlezdu Metab. Čigota 2005, 10, 25–34. [Google Scholar]
- Champion, J.K.; Williams, M. Small bowel obstruction and internal hernias after laparoscopic Roux-en-Y gastric bypass. Obes. Surg. 2003, 13, 596–600. [Google Scholar] [CrossRef]
- Buchwald, H.; Estok, R.; Fahrbach, K.; Banel, D.; Jensen, M.D.; Pories, W.J.; Bantle, J.P.; Sledge, I. Weight and type II diabetes after bariatric surgery: Systematic review and mata-analysis. Am. J. Med. 2009, 122, 248–256. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Morabito, A. Long-term prevention of mortality in morbid obesity through bariatric surgery. A systematic review and meta-analysis of trials performed with gastric banding and gastric bypass. Ann. Surg. 2011, 253, 484–487. [Google Scholar] [CrossRef]
- Chang, S.H.; Stoll, C.R.; Song, J.; Varela, J.E.; Eagon, C.J.; Colditz, G.A. The effectiveness and risks of bariatric surgery: An updated systematic review and meta-analysis, 2003–2012. JAMA Surg. 2014, 149, 275–287. [Google Scholar] [CrossRef] [Green Version]
- Flum, D.R.; Belle, S.H.; King, W.C.; Wahed, A.S.; Berk, P.; Chapman, W.; Pories, W.; Courcoulas, A.; McCloskey, C.; Mitchell, J.; et al. Perioperative safety in the longitudinal assessment of bariatric surgery. N. Engl. J. Med. 2009, 361, 445–454. [Google Scholar]
- Bamgbade, O.A.; Adeogun, B.O.; Abbas, K. Fast-track laparoscopic bypass surgery: Outcomes and lessons from a bariatric surgery service in the United Kingdom. Obes. Surg. 2012, 22, 398–402. [Google Scholar] [CrossRef]
- Nedeljković-Arsenović, O. Effects of Bariatric Surgery on Cardiopulmonary Functional Capacity in Morbidly Obese Patients. Ph.D. Dissertation, School of Medicine, University of Belgrade, Belgrade, Serbia, 2019. [Google Scholar]
- Nedeljkovic-Arsenovic, O.; Banovic, M.; Radenkovic, D.; Rancic, N.; Polovina, S.; Micic, D.; Nedeljkovic, I. The amount of weight loss six months after bariatric surgery: It makes a difference. Obes. Facts 2019, 12, 281–290. [Google Scholar] [CrossRef]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Torgerson, J.S.; Sjöström, L. The Swedish Obese Subjects (SOS) study: Rationale and results. Int. J. Obes. 2001, 25, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Adams, T.D.; Gress, R.E.; Smith, S.C.; Halverson, R.C.; Simper, S.C.; Rosamond, W.D.; Lamonte, M.J.; Stroup, A.M.; Hunt, S.C. Long-term mortality after gastric bypass surgery. N. Engl. J. Med. 2007, 357, 753–761. [Google Scholar] [CrossRef] [Green Version]
- Flum, D.R.; Dellinger, E.P. Impact of gastric bypass operation on survival: A population-based analysis. J. Am. Coll Surg. 2004, 199, 543–551. [Google Scholar] [CrossRef]
- Schauer, P.R.; Bhatt, D.L.; Kirwan, J.P.; Wolski, K.; Aminian, A.; Brethauer, S.A.; Navaneethan, S.D.; Singh, R.P.; Pothier, C.E.; Nissen, S.E.; et al. Bariatric surgery versus intensive medical therapy for diabetes—5-year outcomes. N. Engl. J. Med. 2017, 376, 641–651. [Google Scholar] [CrossRef] [Green Version]
- Christou, N.V.; Sampalis, J.S.; Liberman, M.; Look, D.; Auger, S.; McLean, A.P.; MacLean, L.D. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann. Surg. 2004, 240, 416–423. [Google Scholar] [CrossRef]
- Fontaine, K.R.; Allison, D.B. Does intentional weight loss affect mortality rate? Eat. Behav. 2001, 2, 87–95. [Google Scholar] [CrossRef]
- Williamson, D.F.; Thompson, T.J.; Thun, M.; Flanders, D.; Pamuk, E.; Byers, T. Intentional weight loss and mortality among overweight individuals with diabetes. Diabetes Care 2000, 23, 1499–1504. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.C.; Edwards, C.B.; Goodman, G.N.; Halversen, R.C.; Simper, S.C. Open vs laparoscopic Rouxen-Y gastric bypass: Comparison of operative morbidity and mortality. Obes. Surg. 2004, 14, 73–76. [Google Scholar] [CrossRef]
- Batsis, J.A.; Romero-Corral, A.; Collazo-Clavell, M.L.; Sarr, M.G.; Somers, V.K.; Lopez-Jimenez, F. Effect of bariatric surgery on the metabolic syndrome: A population-based, long-term controlled study. Mayo Clin. Proc. 2008, 83, 897–907. [Google Scholar] [CrossRef]
- Schauer, P.R.; Kashyap, S.R.; Wolski, K.; Brethauer, S.A.; Kirwan, J.P.; Pothier, C.E.; Thomas, S.; Abood, B.; Nissen, S.E.; Bhatt, D.L. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N. Engl. J. Med. 2012, 366, 1567–1576. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Blanco, D.; Funes-Romero, D.; Madiraju, S.; Perez-Quirante, F.; Lo Menzo, E.; Szomstein, S.; Rosenthal, R.J. Reduction of Framingham BMI score after rapid weight loss in severely obese subjects undergoing sleeve gastrectomy: A single institution experience. Surg. Endosc. 2018, 32, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Thaler, J.P.; Cummings, D.E. Minireview: Hormonal and metabolic mechanisms of diabetes remission after gastrointestinal surgery. Endocrinology 2009, 150, 2518–2525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patti, M.E.; McMahon, G.; Mun, E.C.; Bitton, A.; Holst, J.J.; Goldsmith, J.; Hanto, D.W.; Callery, M.; Arky, R.; Nose, V.; et al. Severe hypoglycaemia post-gastric bypass requiring partial pancreatectomy: Evidence for inappropriate insulin secretion and pancreatic islet hyperplasia. Diabetologia 2005, 48, 2236–2240. [Google Scholar] [CrossRef] [PubMed]
- Mosenzon, O.; Pollack, R.; Raz, I. Treatment of Type 2 Diabetes: From “Guidelines” to “Position Statements” and Back. Diabetes Care 2016, 39, 146–153. [Google Scholar] [CrossRef] [Green Version]
- Pories, W.J.; MacDonald, K.G., Jr.; Flickinger, E.G.; Dohm, G.L.; Sinha, M.K.; Barakat, H.A.; May, H.J.; Khazanie, P.; Swanson, M.S.; Morgan, E. Is type II diabetes mellitus (NIDDM) a surgical disease? Ann. Surg. 1992, 215, 633–642. [Google Scholar] [CrossRef] [Green Version]
- Buchwald, H.; Avidor, Y.; Braunwald, E.; Jensen, M.D.; Pories, W.; Fahrbach, K.; Schoelles, K. Bariatric surgery: A systematic review and meta-analysis. JAMA 2004, 292, 1724–1737. [Google Scholar] [CrossRef]
- Egberts, K.; Brown, W.A.; Brennan, L.; O’Brien, P.E. Does exercise improve weight loss after bariatric surgery? A systematic review. Obes. Surg. 2012, 22, 335–341. [Google Scholar] [CrossRef]
- Herring, L.Y.; Stevinson, C.; Davies, M.J.; Biddle, S.J.; Sutton, C.; Bowrey, D.; Carter, P. Changes in physical activity behaviour and physical function after bariatric surgery: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 250–261. [Google Scholar] [CrossRef] [Green Version]
- Olbers, T.; Beamish, A.J.; Gronowitz, E.; Flodmark, C.E.; Dahlgren, J.; Bruze, G.; Ekbom, K.; Friberg, P.; Göthberg, G.; Järvholm, K.; et al. Laparoscopic Roux-en-Y gastric bypass in adolescents with severe obesity: A prospective five-year Swedish nationwide study (AMOS). Lancet Diabetes Endocrinol. 2017, 5, 174–183. [Google Scholar] [CrossRef] [Green Version]
- Tsai, A.G.; Williamson, D.F.; Glick, H.A. Direct medical cost of overweight and obesity in the United States: A quantitative systematic review. Obes. Rev. 2011, 12, 50–61. [Google Scholar] [CrossRef]
- The Guardian. Global Cost of Obesity-Related Illness to Hit $1.2tn a Year from 2025. Available online: www.theguardian.com/society/2017/oct/10/treating-obesity-related-illness-will-cost-12tn-a-year-from-2025-experts-warn (accessed on 5 September 2020).
- Angrisani, L.; Cutolo, P.P.; Formisano, G.; Nosso, G.; Vitolo, G. Laparoscopic adjustable gastric banding versus Roux-en-Y gastric bypass: 10-year results of a prospective, randomized trial. Surg. Obes. Relat. Dis. 2013, 9, 405–413. [Google Scholar] [CrossRef]
- Abbatini, F.; Capoccia, D.; Casella, G.; Soricelli, E.; Leonetti, F.; Basso, N. Long-term remission of type 2 diabetes in morbidly obese patients after sleeve gastrectomy. Surg. Obes. Relat. Dis. 2013, 9, 498–502. [Google Scholar] [CrossRef]

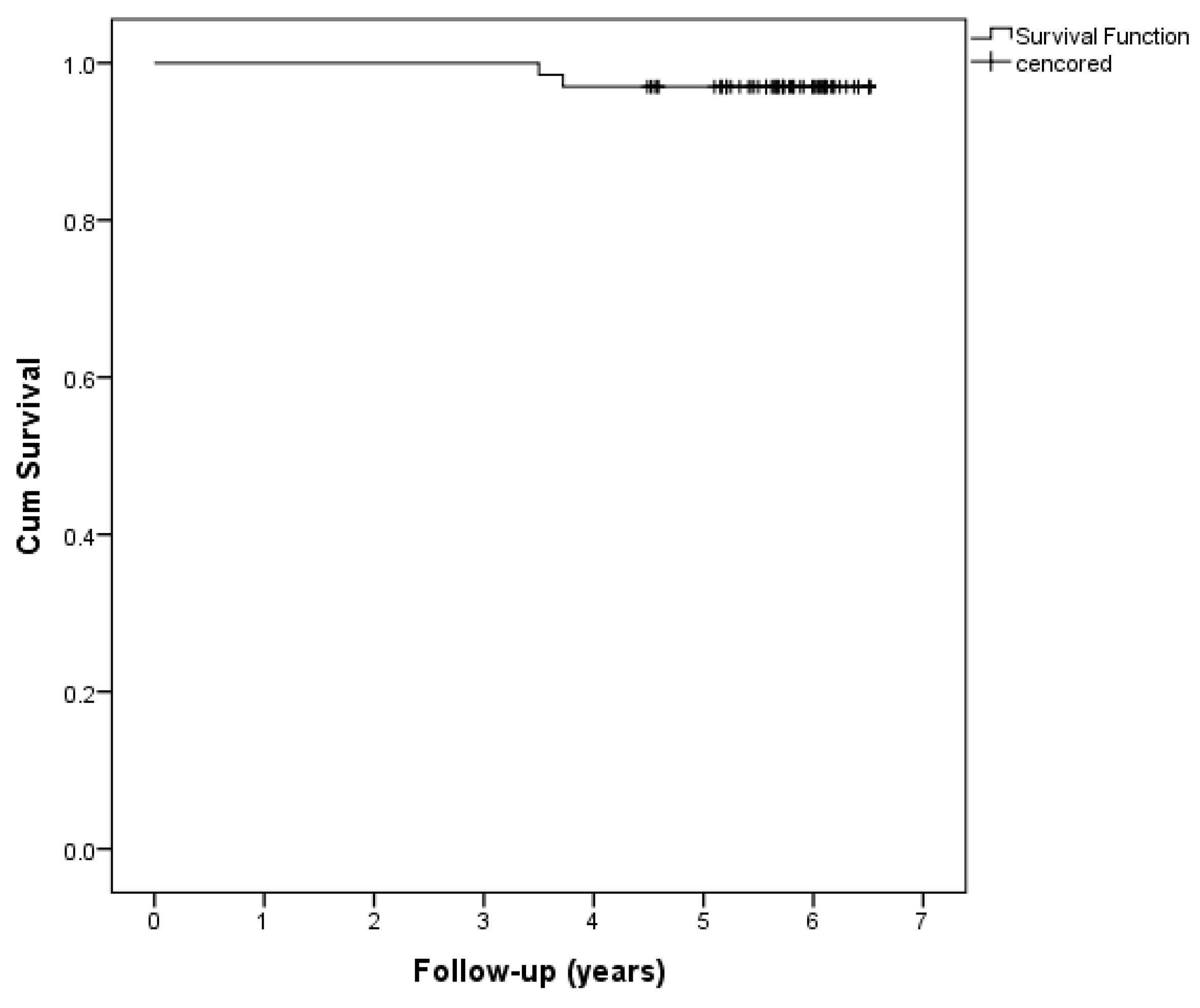
| One-year overall survival | 100% |
| Three-year overall survival | 100% |
| Five-year overall survival | 96.97% |



{kind=link}
{kind=link}
{kind=link}
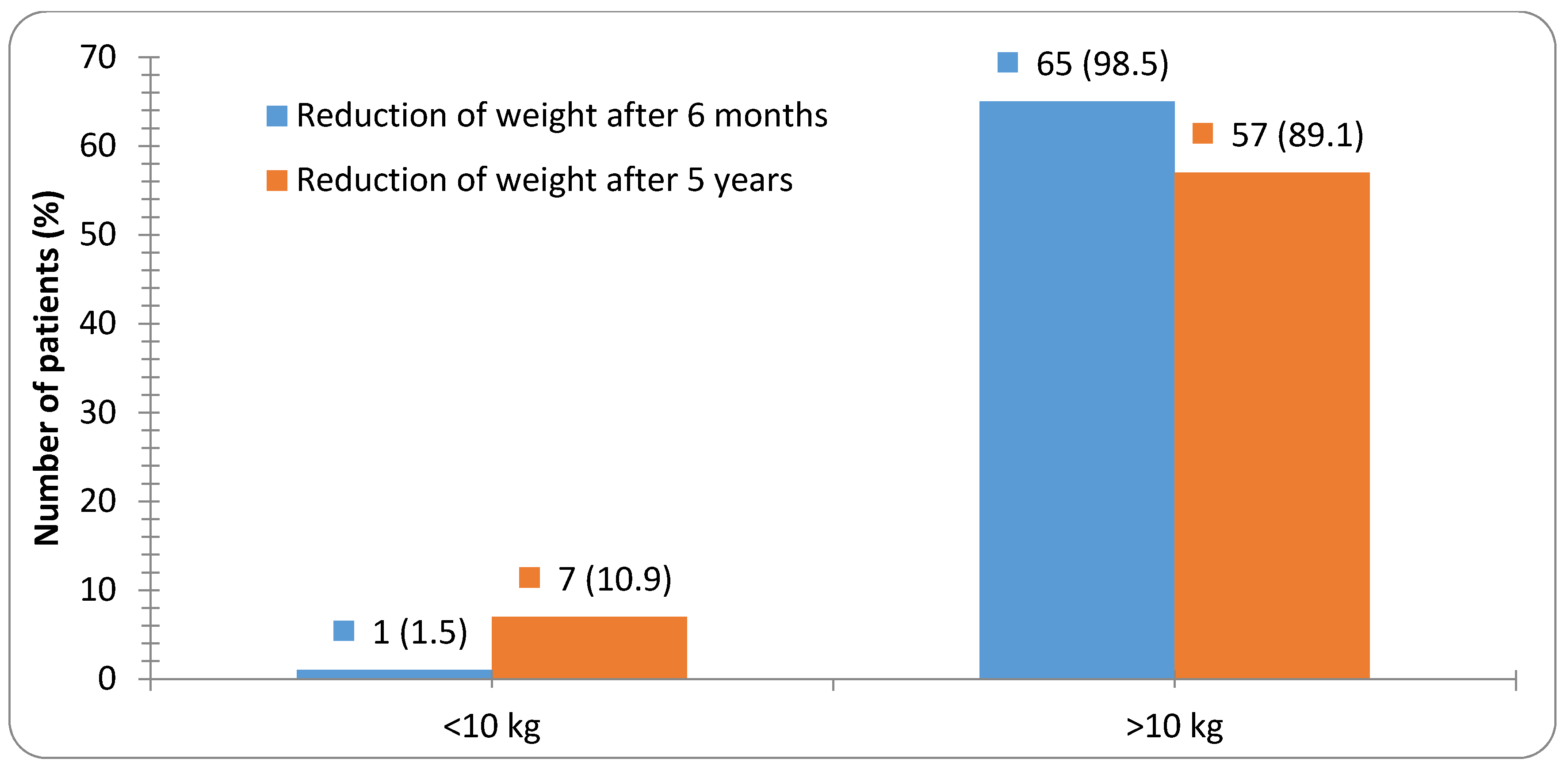
| Weight Loss | Five Years Versus Six Months after Surgery | p Value 1 | |
|---|---|---|---|
| No | Yes | ||
| 6 months (n = 64) | 2 | 62 | <0.001 |
| 5 years (n = 62) | 24 | 38 | |
| Number (%) | Before Surgery | Five Years after Surgery | p Value 1 |
|---|---|---|---|
| Co-morbidities: | |||
| Physical activity: active | 23 (34.8) | 46 (71.9) | <0.001 |
| Hypertension: yes | 29 (43.9) | 23 (35.9) | 0.452 |
| OSA: yes | 2 (3.0) | - | 0.490 |
| T2DM: yes | 24 (36.4) | 9 (14.1) | 0.005 |
| Hypercholesterolemia: yes | 6 (9.1) | 7 (10.6) | 1.000 |
| Hypertriglyceridemia: yes | 6 (9.1) | 5 (7.8) | 1.000 |
| Smoking: yes | 14 (21.2) | 22 (33.3) | 0.193 |
| Therapy: | |||
| Antihypertensive therapy: yes | 26 (39.4) | 21 (32.8) | 0.681 |
| Beta blockers: yes | 16 (24.2) | 10 (15.6) | 0.313 |
| Ca antagonist: yes | 11 (16.7) | 5 (7.8) | 0.204 |
| ACE inhibitors: yes | 17 (25.8) | 17 (26.6) | 1.000 |
| Antidiabetics: yes | 24 (36.4) | 10 (15.6) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nedeljkovic-Arsenovic, O.; Banovic, M.; Radenkovic, D.; Rancic, N.; Polovina, S.; Micic, D.; Nedeljkovic, I. Five-Year Outcomes in Bariatric Surgery Patients. Medicina 2020, 56, 669. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120669
Nedeljkovic-Arsenovic O, Banovic M, Radenkovic D, Rancic N, Polovina S, Micic D, Nedeljkovic I. Five-Year Outcomes in Bariatric Surgery Patients. Medicina. 2020; 56(12):669. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120669
Chicago/Turabian StyleNedeljkovic-Arsenovic, Olga, Marko Banovic, Dejan Radenkovic, Nemanja Rancic, Snezana Polovina, Dragan Micic, and Ivana Nedeljkovic. 2020. "Five-Year Outcomes in Bariatric Surgery Patients" Medicina 56, no. 12: 669. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120669