Evaluation of the Direct Economic Cost per Eradication Treatment Regimen against Helicobacter pylori Infection in Greece: Do National Health Policy-Makers Need to Care?

 , , , ,
, , , ,
Abstract
:1. Introduction
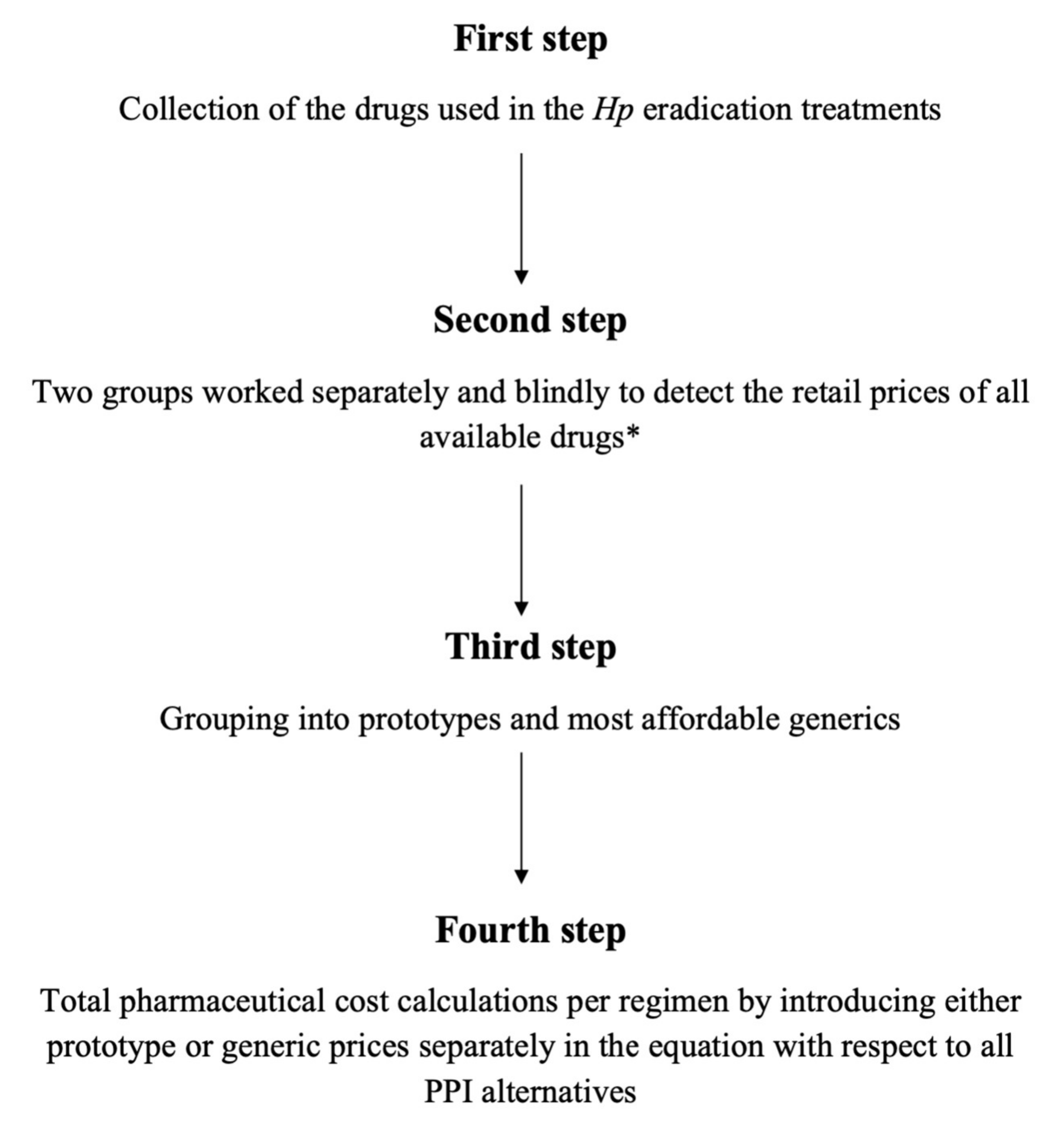
2. Materials and Methods
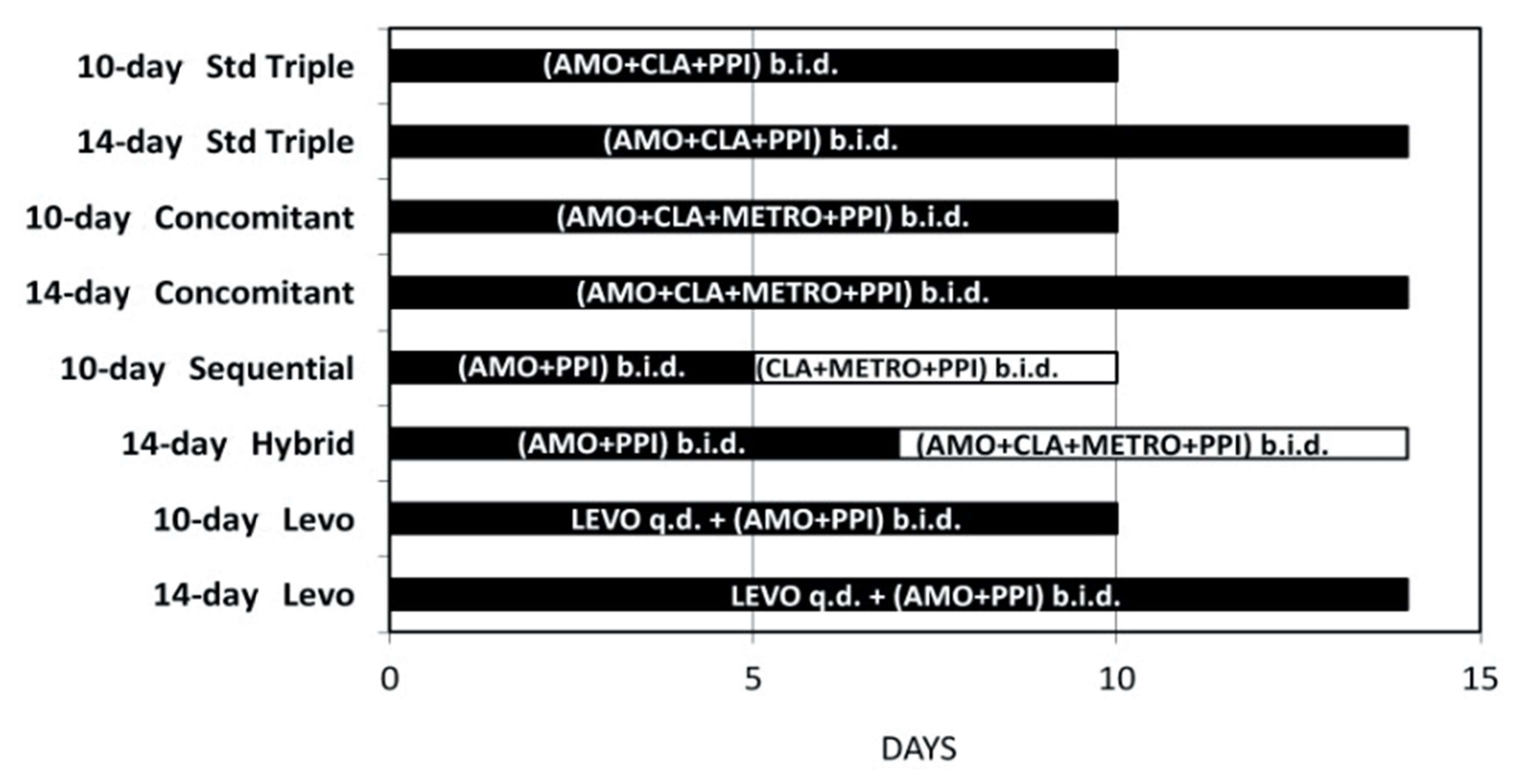
- First-line regimens:
- i.
- 10-day standard triple
- ii.
- 14-day standard triple,
- iii.
- 10-day sequential,
- iv.
- 14-day sequential,
- v.
- 10-day concomitant non-bismuth quadruple
- vi.
- 14-day concomitant non-bismuth quadruple,
- vii.
- 14-day hybrid,
- Second-line salvage regimens:
- i.
- 10-day levofloxacin-containing triple regimen,
- ii.
- 14-day levofloxacin-containing triple regimen.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zavras, D.; Zavras, A.I.; Kyriopoulos, I.-I.; Kyriopoulos, J. Economic crisis, austerity and unmet healthcare needs: The case of Greece. BMC Health Serv. Res. 2016, 16, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ifanti, A.A.; Argyriou, A.A.; Kalofonou, F.H.; Kalofonos, H.P. Financial crisis and austerity measures in Greece: Their impact on health promotion policies and public health care. Health Policy 2013, 113, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Expenditure for Selected Health Care Functions by Health Care Financing Schemes. EUROSTAT 2019. Available online: https://ec.europa.eu/eurostat/web/products-datasets/product?code=hlth_sha11_hchf (accessed on 30 August 2019).
- Wouters, O.J.; Kanavos, P.G.; Mckee, M. Comparing Generic Drug Markets in Europe and the United States: Prices, Volumes, and Spending. Milbank Q. 2017, 95, 554–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skaltsas, L.N.; Vasileiou, K.Z. Patients’ perceptions of generic drugs in Greece. Health Policy 2015, 119, 1406–1414. [Google Scholar] [CrossRef]
- Bonovas, S.; Nikolopoulos, G.K. High-burden epidemics in Greece in the era of economic crisis. Early signs of a public health tragedy. J. Prev. Med. Hyg. 2012, 53, 169–171. [Google Scholar]
- Eusebi, L.H.; Zagari, R.M.; Bazzoli, F. Epidemiology of Helicobacter pylori Infection. Helicobacter 2014, 19, 1–5. [Google Scholar] [CrossRef]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Mori, H. World trends for H. pylori eradication therapy and gastric cancer prevention strategy by H. pylori test-and-treat. J. Gastroenterol. 2018, 53, 354–361. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of helicobacter pylori infection-the Maastricht V/Florence consensus report. Gut 2016, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Doulberis, M.; Kotronis, G.; Thomann, R.; Polyzos, S.A.; Boziki, M.; Gialamprinou, D.; Deretzi, G.; Katsinelos, P.; Kountouras, J. Review: Impact of Helicobacter pylori on Alzheimer’s disease: What do we know so far? Helicobacter 2018, 23, e12454. [Google Scholar] [CrossRef]
- Franceschi, F.; Gasbarrini, A.; Polyzos, S.A.; Kountouras, J. Extragastric Diseases and Helicobacter pylori. Helicobacter 2015, 20 (Suppl. 1), 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzano, M.; Bisio, A.; Grassi, G. Helicobacter pylori and diabetes mellitus: A controversial relationship. Minerva Endocrinol. 2019, 44, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Zhang, R.; Ni, P.; Chen, S.; Duan, G. Helicobacter pylori Infection and Psoriasis: A Systematic Review and Meta-Analysis. Medicina 2019, 26, 645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsolaki, F.; Gogaki, E.; Sakkias, F.; Skatharoudi, C.; Lopatatzidi, C.; Tsoulopoulos, V.; Lampoura, S.; Topouzis, F.; Tsolaki, M.; Kountouras, J. Helicobacter pylori infection and primary open-angle glaucoma: Is there a connection? Clin. Ophthalmol. 2012, 6, 45–47. [Google Scholar] [CrossRef] [Green Version]
- Shen, X.; Yang, H.; Wu, Y.; Zhang, D.; Jiang, H. Meta-analysis: Association of Helicobacter pylori infection with Parkinson’s diseases. Helicobacter 2017, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Georgopoulos, S.D.; Xirouchakis, E.; Martinez-Gonzales, B.; Zampeli, E.; Grivas, E.; Spiliadi, C.; Sotiropoulou, M.; Petraki, K.; Zografos, K.; Laoudi, F.; et al. Randomized clinical trial comparing ten day concomitant and sequential therapies for Helicobacter pylori eradication in a high clarithromycin resistance area. Eur. J. Intern. Med. 2016, 32, 84–90. [Google Scholar] [CrossRef]
- Karamanolis, G.P.; Daikos, G.L.; Xouris, D.; Goukos, D.; Delladetsima, I.; Ladas, S.D. The evolution of helicobacter pylori antibiotics resistance over 10 years in Greece. Digestion 2014, 90, 229–231. [Google Scholar] [CrossRef]
- Galinos Pharmaceutical Guide 2019. Available online: https://www.galinos.gr/ (accessed on 17 September 2019).
- National Organization for Medicines 2019. Available online: https://www.eof.gr/web/guest/home (accessed on 17 September 2019).
- De Francesco, V.; Bellesia, A.; Ridola, L.; Manta, R.; Zullo, A. First-line therapies for Helicobacter pylori eradication: A critical reappraisal of updated guidelines. Ann. Gastroenterol. 2017, 30, 373–379. [Google Scholar] [CrossRef]
- Apostolopoulos, P.; Koumoutsos, I.; Ekmektzoglou, K.; Dogantzis, P.; Vlachou, E.; Kalantzis, C.; Tsibouris, P.; Alexandrakis, G. Concomitant versus sequential therapy for the treatment of Helicobacter pylori infection: A Greek randomized prospective study. Scand. J. Gastroenterol. 2016, 51, 145–151. [Google Scholar] [CrossRef]
- Georgopoulos, S.; Papastergiou, V.; Xirouchakis, E.; Laudi, F.; Papantoniou, N.; Lisgos, P.; Spiliadi, C.; Fragou, P.; Skorda, L.; Karatapanis, S. Evaluation of a Four-drug, Three-antibiotic, Nonbismuth-containing “Concomitant” Therapy as First-line Helicobacter pylori Eradication Regimen in Greece. Helicobacter 2012, 17, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Porowska, B.; De Angelis, M.; Oliva, A. Antibiotic susceptibility, heteroresistance, and updated treatment strategies in helicobacter pylori infection. Drug Des. Dev. Ther. 2017, 11, 2209–2220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallone, C.A.; Moss, S.F.; Malfertheiner, P. Reconciliation of Recent Helicobacter pylori Treatment Guidelines in a Time of Increasing Resistance to Antibiotics. Gastroenterology 2019. [Google Scholar] [CrossRef] [PubMed]
- Papastergiou, V.; Georgopoulos, S.D.; Karatapanis, S. Treatment of Helicobacter pylori infection: Meeting the challenge of antimicrobial resistance. World J. Gastroenterol. 2014, 20, 9898–9911. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, R.; Zagari, R.M.; Zhang, S.; Saracco, G.M.; Moss, S.F. Pharmacological considerations and step-by-step proposal for the treatment of Helicobacter pylori infection in the year 2018. Minerva Gastroenterol. Dietol. 2018, 64, 310–321. [Google Scholar] [CrossRef] [Green Version]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimoyama, T.; Chinda, D.; Sawada, Y.; Komai, K.; Chiba, H.; Saito, Y.; Sasaki, Y.; Matsuzaka, M.; Fukuda, S. Randomized Trial Comparing Esomeprazole and Rabeprazole in First-line Eradication Therapy for Helicobacter pylori Infection based on the Serum Levels of Pepsinogens. Intern. Med. 2017, 56, 1621–1627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, Y.; Manson, J.; Govan, L.; Harbour, R.; Bennison, J.; Watson, E.; Wu, O. Pharmacological regimens for eradication of Helicobacter pylori: An overview of systematic reviews and network meta-analysis. BMC Gastroenterol. 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Gonzalez, B.; Georgopoulos, S.; Michopoulos, S.; Karayiannis, Y.; Liatsos, C.; Megraud, F.; Sgouras, D.N.; Mentis, A.F. Multicenter survey of antimicrobial resistance in helicobacter pylori isolates in Greece—Trends of resistance 1998–2018. XXXIInd Int. Work. Helicobacter Microbiota Inflamm. Cancer 2019, 24, e12647. [Google Scholar] [CrossRef]
- Liatsos, C.; Georgopoulos, S.D. Helicobacter pylori best treatment approach: Should a national consensus be the best consensus? Ann. Gastroenterol. 2017, 30, 704–706. [Google Scholar] [CrossRef]
- Isaksen, V.J. The impact of the financial crisis on European attitudes toward immigration. Comp. Migr. Stud. 2019, 7, 24. [Google Scholar] [CrossRef]
- Cavounidis, J. The migration experience of Greece and the impact of the economic crisis on its migrant and native populations. Eur. J. Public Health 2018, 28, 20–23. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Eradication Treatment Regimens | Pharmaceutical Cost per Regimen in Euros (€) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prototype-Based Regimens * | Generic-Based Regimens * | |||||||||||||
| O | E (20 mg) | E (40 mg) | P | R | L | CL | O | E (20 mg) | E (40 mg) | P ** | R | L | CL | |
| First Line Regimens | ||||||||||||||
| 10-day standard triple | 37.77 | 32.74 | 33.86 | 28.09 | 34.56 | 38.28 | 38.59 | 26.35 | 23.09 | 23.94 | 21.15 | 24.98 | 26.30 | - |
| 14-day standard triple | 54.77 | 49.74 | 50.86 | 45.09 | 51.56 | 55.28 | 55.59 | 37.41 | 34.15 | 35.00 | 32.21 | 36.04 | 37.36 | - |
| 10-day sequential | 38.57 | 33.54 | 34.66 | 28.89 | 35.36 | 39.08 | 39.39 | 27.15 | 23.89 | 24.74 | 21.95 | 25.78 | 27.10 | - |
| 14-day sequential | 54.00 | 46.96 | 48.52 | 40.45 | 49.50 | 54.71 | 55.15 | 38.01 | 33.45 | 34.64 | 30.73 | 36.09 | 37.94 | |
| 10-day concomitant non-bismuth quadruple | 42.55 | 37.52 | 38.64 | 32.87 | 39.34 | 43.06 | 43.37 | 31.13 | 27.87 | 28.72 | 25.93 | 29.76 | 31.08 | - |
| 14-day concomitant non-bismuth quadruple | 59.55 | 54.52 | 55.64 | 49.87 | 56.34 | 60.06 | 60.37 | 42.19 | 38.93 | 39.78 | 36.99 | 40.82 | 42.14 | - |
| 14-day hybrid | 42.55 | 37.52 | 38.64 | 32.87 | 39.34 | 43.06 | 43.37 | 31.13 | 27.87 | 28.72 | 25.93 | 29.76 | 31.08 | - |
| Second Line Salvage Regimens | ||||||||||||||
| 10-day levofloxacin-containing triple regimen | 31.03 | 26.00 | 27.12 | 21.35 | 27.82 | 31.54 | 31.85 | 21.16 | 17.90 | 18.75 | 15.96 | 19.79 | 21.11 | - |
| 14-day levofloxacin-containing triple regimen | 36.16 | 31.13 | 32.15 | 26.48 | 32.95 | 36.67 | 36.98 | 25.21 | 21.95 | 22.80 | 20.01 | 23.84 | 25.16 | - |
| Eradication Treatment Regimens | Mean Cost in Euros (€) | Price Difference in Euros (€) |
|---|---|---|
| First Line Regimens | ||
| 10-day standard triple | 29.98 | 17.44 |
| 14-day standard triple | 44.24 | 23.38 |
| 10-day sequential | 30.78 | 17.44 |
| 14-day sequential | 43.09 | 24.42 |
| 10-day concomitant non-bismuth quadruple | 34.76 | 17.44 |
| 14-day concomitant non-bismuth quadruple | 49.02 | 23.38 |
| 14-day hybrid | 34.76 | 17.44 |
| Second Line Salvage Regimens | ||
| 10-day levofloxacin-containing triple regimen | 23.72 | 15.89 |
| 14-day levofloxacin-containing triple regimen | 28.58 | 16.96 |
| Intervention | Cost in Euros (€) |
|---|---|
| Esophagogastroduodenoscopy | 77 |
| Serum anti-Hp antibodies | 13.60 |
| C13 Urea Breath Test (Helicobacter Test INFAI®) | 30.36 |
| Gastric histology using Giemsa stain | 27.76 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liatsos, C.; Papaefthymiou, A.; Kyriakos, N.; Giakoumis, M.; Kountouras, J.; Galanopoulos, M.; Apostolopoulos, P.; Georgopoulos, S.D.; Mavrogiannis, C.; Exadaktylos, A.K.; et al. Evaluation of the Direct Economic Cost per Eradication Treatment Regimen against Helicobacter pylori Infection in Greece: Do National Health Policy-Makers Need to Care? Medicina 2020, 56, 133. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030133
Liatsos C, Papaefthymiou A, Kyriakos N, Giakoumis M, Kountouras J, Galanopoulos M, Apostolopoulos P, Georgopoulos SD, Mavrogiannis C, Exadaktylos AK, et al. Evaluation of the Direct Economic Cost per Eradication Treatment Regimen against Helicobacter pylori Infection in Greece: Do National Health Policy-Makers Need to Care? Medicina. 2020; 56(3):133. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030133
Chicago/Turabian StyleLiatsos, Christos, Apostolis Papaefthymiou, Nikolaos Kyriakos, Marios Giakoumis, Jannis Kountouras, Michail Galanopoulos, Periklis Apostolopoulos, Sotirios D. Georgopoulos, Christos Mavrogiannis, Aristomenis K. Exadaktylos, and et al. 2020. "Evaluation of the Direct Economic Cost per Eradication Treatment Regimen against Helicobacter pylori Infection in Greece: Do National Health Policy-Makers Need to Care?" Medicina 56, no. 3: 133. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56030133