Oral Administration of Cannabis and Δ-9-tetrahydrocannabinol (THC) Preparations: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
1.1. Cannabinoids
1.2. Therapeutic Uses of Cannabis
1.3. Oral Cannabis and THC and other Routes of Administration
1.4. Oral Cannabinoid Preparations
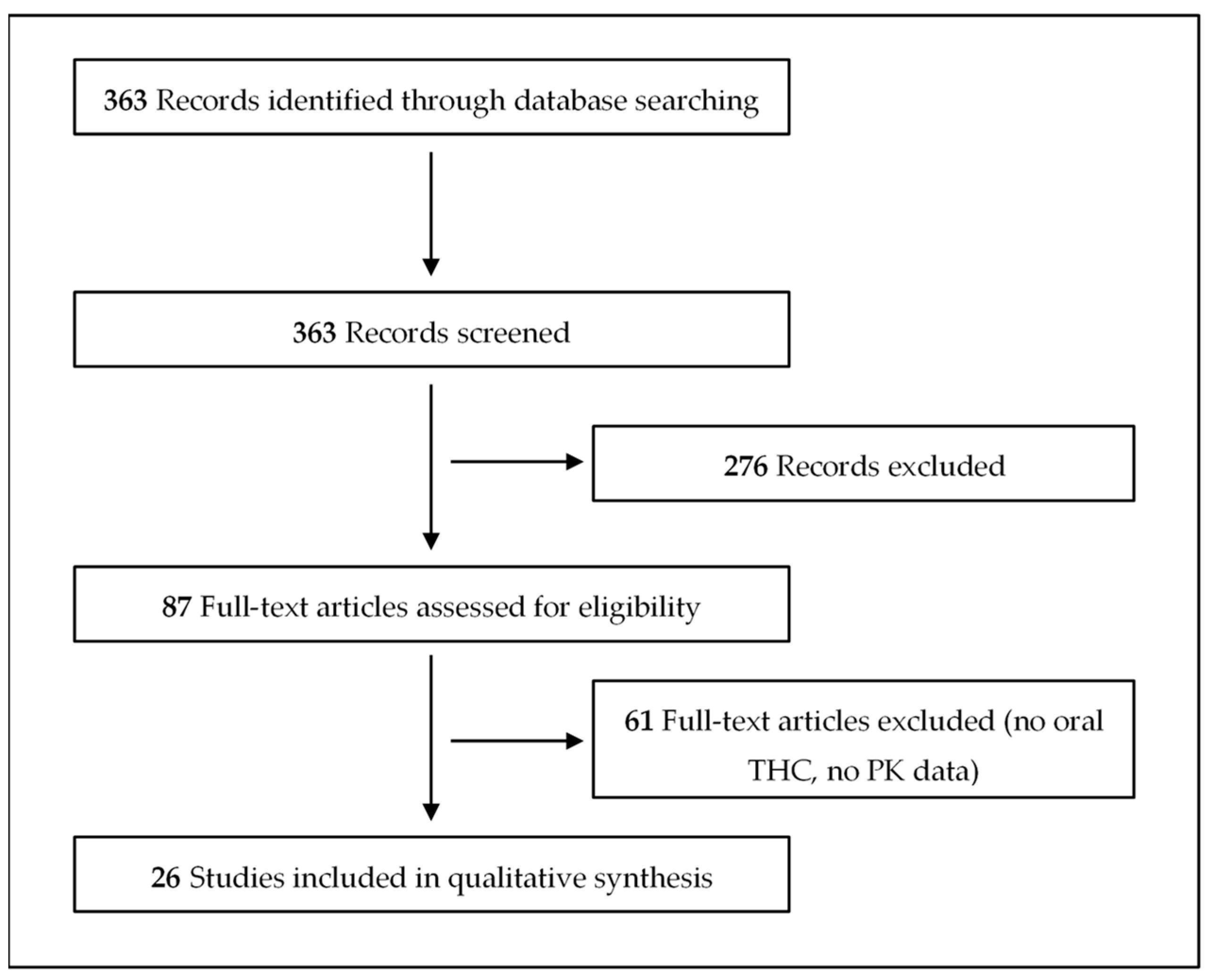
2. Materials and Methods
3. Results
3.1. Capsules
3.2. Oil
3.3. Decoctions
3.4. Tablets
3.5. Baked Goods
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations Office on Drugs and Crime (UNODC). World Drug Report 2019. Available online: https://wdr.unodc.org/wdr2019/index.html. (accessed on 5 April 2020).
- Morales, P.; Hurst, D.P.; Reggio, P.H. Molecular Targets of the Phytocannabinoids: A Complex Picture. Prog. Chem. Org. Nat. Prod. 2017, 103, 103–131. [Google Scholar] [PubMed] [Green Version]
- ElSohly, M.A.; Radwan, M.M.; Gul, W.; Chandra, S.; Galal, A. Phytochemistry of Cannabis sativa L. Prog. Chem. Org. Nat. Prod. 2017, 103, 1–36. [Google Scholar] [PubMed]
- Kaur, R.; Ambwani, S.R.; Singh, S. Endocannabinoid System: A Multi-Facet Therapeutic Target. Curr. Clin. Pharmacol. 2016, 11, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Maccarrone, M.; Maldonado, R.; Casas, M.; Henze, T.; Centonze, D. Cannabinoids therapeutic use: What is our current understanding following the introduction of THC, THC:CBD oromucosal spray and others? Expert Rev. Clin. Pharmacol. 2017, 10, 443–455. [Google Scholar] [CrossRef]
- Andre, C.M.; Hausman, J.F.; Guerriero, G. Cannabis sativa: The Plant of the Thousand and One Molecules. Front. Plant. Sci. 2016, 7, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisanti, S.; Malfitano, A.M.; Ciaglia, E.; Lamberti, A.; Ranieri, R.; Cuomo, G.; Abate, M.; Faggiana, G.; Proto, M.C.; Fiore, D.; et al. Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacol. Ther. 2017, 175, 133–150. [Google Scholar] [CrossRef]
- Mannucci, C.; Navarra, M.; Calapai, F.; Spagnolo, E.V.; Busardò, F.P.; Cas, R.D.; Ippolito, F.M.; Calapai, G. Neurological Aspects of Medical Use of Cannabidiol. CNS Neurol. Disord. Drug Targets 2017, 16, 541–553. [Google Scholar] [CrossRef] [Green Version]
- Laprairie, R.B.; Bagher, A.M.; Kelly, M.E.M.; Denovan-Wright, E.M. Cannabidiol Is a Negative Allosteric Modulator of the Cannabinoid CB1 Receptor. Br. J. Pharmacol. 2015, 172, 4790–4805. [Google Scholar] [CrossRef] [Green Version]
- Mueller, J.K.; Reuter, A.R.; Lange, B.; Schaefer, A.; Hanke, F.; Pahlisch, F.; Schaefer, C.; Schmidt, A.-M.; Woelfl, T.; Enning, F.; et al. Effects and interaction of delta-9-tetrahydrocannabidiol and cannabidiol on psychopathology, neurocognition, and endocannabinoids in serum of healthy volunteers: Influence on psychopathology. Neuropsychopharmacology 2016, 41, S589. [Google Scholar]
- Morgan, C.J.A.; Freeman, T.P.; Hindocha, C.; Schafer, G.; Gardner, C.; Curran, H.V. Individual and combined effects of acute delta-9tetrahydrocannabinol and cannabidiol on psychotomimetic symptoms and memory function. Transl. Psychiatry 2018, 8, 181. [Google Scholar] [CrossRef]
- Hindley, G.; Beck, K.; Borgan, F.; Ginestet, C.E.; McCutcheon, R.; Kleinloog, D.; Ganesh, S.; Radhakrishnan, R.; D'Souza, D.C.; Howes, O.D. Psychiatric symptoms caused by cannabis constituents: A systematic review and meta-analysis. Lancet Psychiatry 2020, 7, 344–353. [Google Scholar] [CrossRef]
- Arkell, T.R.; Lintzeris, N.; Kevin, R.C.; Ramaekers, J.G.; Vandrey, R.; Irwin, C.; Haber, P.S.; McGregor, I.S. Cannabidiol (CBD) content in vaporized cannabis does not prevent tetrahydrocannabinol (THC)-induced impairment of driving and cognition. Psychopharmacology 2019, 236, 2713–2724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papaseit, E.; Pérez-Mañá, C.; Pérez-Acevedo, A.P.; Hladun, O.; Torres-Moreno, M.C.; Muga, R.; Torrens, M.; Farré, M. Cannabinoids: From pot to lab. Int. J. Med. Sci. 2018, 6, 1286–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazekamp, A.; Heerdink, E.R. The prevalence and incidence of medicinal cannabis on prescription in The Netherlands. Eur. J. Clin. Pharmacol. 2013, 69, 1575–1580. [Google Scholar] [CrossRef]
- de Hoop, B.; Heerdink, E.R.; Hazekamp, A. Medicinal Cannabis on Prescription in The Netherlands: Statistics for 2003–2016. Cannabis Cannabinoid Res. 2018, 3, 54–55. [Google Scholar] [CrossRef] [Green Version]
- Shiplo, S.; Asbridge, M.; Leatherdale, S.T.; Hammond, D. Medical cannabis use in Canada: Vapourization and modes of delivery. Harm Reduct. J. 2016, 13, 30. [Google Scholar] [CrossRef] [Green Version]
- Boehnke, K.F.; Scott, J.R.; Litinas, E.; Sisley, S.; Clauw, D.J.; Goesling, J.; Williams, D.A. Cannabis Use Preferences and Decision-making Among a Cross-sectional Cohort of Medical Cannabis Patients with Chronic Pain. J. Pain 2019, 20, 1362–1372. [Google Scholar] [CrossRef]
- Bouso, J.C.; Jiménez-Garrido, D.; Ona, G.; Woźnica, D.; Dos Santos, R.G.; Hallak, J.E.C.; Paranhos, B.A.P.B.; de Almeida Mendes, F.; Yonamine, M.; Alcázar-Córcoles, M.Á.; et al. Quality of life, mental health, personality, and patterns of use in self-medicated cannabis users with chronic diseases: A 12-month longitudinal study. Phytother Res. 2020, 1–8. [Google Scholar] [CrossRef]
- Jett, J.; Stone, E.; Warren, G.; Cummings, K.M. Cannabis Use, Lung Cancer, and Related Issues. J. Thorac. Oncol. 2018, 3, 480–487. [Google Scholar] [CrossRef] [Green Version]
- Abeles, M.; Popofsky, S.; Wen, A.; Valsamis, C.; Webb, A.; Halaby, C.; Pirzada, M. Vaping-associated lung injury caused by inhalation of cannabis oil. Pediatr. Pulmonol. 2020, 55, 226–228. [Google Scholar] [CrossRef]
- Thakrar, P.D.; Boyd, K.P.; Swanson, C.P.; Wideburg, E.; Kumbhar, S.S. E-cigarette, or vaping, product use-associated lung injury in adolescents: A review of imaging features. Pediatr. Radiol. 2020, 50, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Duffy, B.; Li, L.; Lu, S.; Durocher, L.; Dittmar, M.; Delaney-Baldwin, E.; Panawennage, D.; LeMaster, D.; Navarette, K.; Spink, D. Analysis of Cannabinoid-Containing Fluids in Illicit Vaping Cartridges Recovered from Pulmonary Injury Patients: Identification of Vitamin E Acetate as a Major Diluent. Toxics 2020, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Brunetti, P.; Pichini, S.; Pacifici, R.; Busardó, F.P.; del Rio, A. Herbal preparations of medical cannabis: A Vademecum for prescribing doctors. Medicina 2020, 56, 237. [Google Scholar] [CrossRef]
- Levinsohn, E.A.; Hill, K.P. Clinical uses of cannabis and cannabinoids in the United States. J. Neurol. Sci. 2020, 411, 116717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Moreno, M.C.; Papaseit, E.; Torrens, M.; Farré, M. Assessment of Efficacy and Tolerability of Medicinal Cannabinoids in Patients with Multiple Sclerosis: A Systematic Review and Meta-analysis. JAMA Netw. Open 2018, 1, e183485. [Google Scholar] [CrossRef] [Green Version]
- EMCDDA (European Monitoring Centre for Drugs and Drug Addiction). Medical Use of Cannabis and Cannabinoids. December 2018. Available online: http://www.emcdda.europa.eu/publications/rapid-communications/medical-use-of-cannabis-and-cannabinoids-questions-and-answers-for-policymaking_en. (accessed on 5 April 2020).
- Bedrocan Medicinal Cannabis. Available online: https://www.bedrocan.com/ (accessed on 5 April 2020).
- Ministero della Salute. Decreto 9 novembre 2015: Funzioni di Organismo Statale per la Cannabis previsto dagli articoli 23 e 28 della convenzione unica sugli stupefacenti del 1961, come modificata nel 1972. Available online: https://www.gazzettaufficiale.it/eli/id/2015/11/30/15A08888/sg (accessed on 5 April 2020).
- Pacifici, R.; Marchei, E.; Salvatore, F.; Guandalini, L.; Busardò, F.P.; Pichini, S. Evaluation of cannabinoids concentration and stability in standardized preparations of cannabis tea and cannabis oil by ultra-high performance liquid chromatography tandem mass spectrometry. Clin. Chem. Lab. Med. 2017, 55, 1555–1563. [Google Scholar] [CrossRef]
- Pacifici, R.; Marchei, E.; Salvatore, F.; Guandalini, L.; Busardò, F.P.; Pichini, S. Stability of cannabinoids in cannabis FM1 flowering tops and oil preparation evaluated by ultra-high performance liquid chromatography tandem mass spectrometry. Clin. Chem. Lab. Med. 2019, 57, e165–e168. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. La produzione nazionale di sostanze attive di origine vegetale a base di Cannabis. Available online: http://www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=4588&area=sostanzeStupefacenti&menu=organismo (accessed on 5 April 2020).
- Cannimed Medical Cannabis. Available online: https://www.cannimed.ca/ (accessed on 5 April 2020).
- Romano, L.L.; Hazekamp, A. Cannabis Oil: Chemical evaluation of an upcoming cannabis-based medicine. Cannabinoids 2013, 1, 1–11. [Google Scholar]
- Monte, A.A.; Shelton, S.K.; Mills, E.; Saben, J.; Hopkinson, A.; Sonn, B.; Devivo, M.; Chang, T.; Fox, J.; Brevik, C.; et al. Acute Illness Associated with Cannabis Use, by Route of Exposure: An Observational Study. Mol. Med. 2019, 116, 229. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Wall, M.E.; Sadler, B.M.; Brine, D.; Taylor, H.; Perez-Reyes, M. Metabolism, disposition, and kinetics of delta-9-tetrahydrocannabinol in men and women. Clin. Pharmacol. Ther. 1983, 34, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Haney, M.; Bisaga, A.; Foltin, R.W. Interaction between naltrexone and oral THC in heavy marijuana smokers. Psychopharmacology 2003, 166, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Naef, M.; Curatolo, M.; Petersen-Felix, S.; Arendt-Nielsen, L.; Zbinden, A.; Brenneisen, R. The analgesic effect of oral delta-9-tetrahydrocannabinol (THC), morphine, and a THC-morphine combination in healthy subjects under experimental pain conditions. Pain 2003, 105, 79–88. [Google Scholar] [CrossRef]
- Guy, G.W.; Robson, P.J. A Phase I, Open Label, Four-Way Crossover Study to Compare the Pharmacokinetic Profiles of a Single Dose of 20 mg of a Cannabis Based Medicine Extract (CBME) Administered on 3 Different Areas of the Buccal Mucosa and to Investigate the Pharmacokinetics of CBME per Oral in Healthy Male and Female Volunteers (GWPK0112). J. Cannabis Ther. 2004, 3, 79–120. [Google Scholar]
- Ménétrey, A.; Augsburger, M.; Favrat, B.; Pin, M.A.; Rothuizen, L.E.; Appenzeller, M.; Buclin, T.; Mangin, P.; Giroud, C. Assessment of driving capability through the use of clinical and psychomotor tests in relation to blood cannabinoids levels following oral administration of 20 mg dronabinol or of a cannabis decoction made with 20 or 60 mg Delta9-THC. J. Anal. Toxicol. 2005, 29, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadulski, T.; Sporkert, F.; Schnelle, M.; Stadelmann, A.M.; Roser, P.; Schefter, T.; Pragst, F. Simultaneous and sensitive analysis of THC, 11-OH-THC, THC-COOH, CBD, and CBN by GC-MS in plasma after oral application of small doses of THC and cannabis extract. J. Anal. Toxicol. 2005, 29, 782–789. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, R.S.; Gustafson, R.A.; Barnes, A.; Nebro, W.; Moolchan, E.T.; Huestis, M.A. Delta(9)-tetrahydrocannabinol, 11-hydroxy-delta(9)-tetrahydrocannabinol and 11-nor-9-carboxy-delta(9)-tetrahydrocannabinol in human plasma after controlled oral administration of cannabinoids. Ther. Drug Monit. 2006, 28, 545–551. [Google Scholar] [CrossRef]
- Schwilke, E.W.; Schwope, D.M.; Karschner, E.L.; Lowe, R.H.; Darwin, W.D.; Kelly, D.L.; Goodwin, R.S.; Gorelick, D.A.; Huestis, M.A. Delta9-tetrahydrocannabinol (THC), 11-hydroxy-THC, and 11-nor-9-carboxy-THC plasma pharmacokinetics during and after continuous high-dose oral THC. Clin. Chem. 2009, 55, 2180–2189. [Google Scholar] [CrossRef] [Green Version]
- Karschner, E.L.; Darwin, W.D.; Goodwin, R.S.; Wright, S.; Huestis, M.A. Plasma cannabinoid pharmacokinetics following controlled oral delta9-tetrahydrocannabinol and oromucosal cannabis extract administration. Clin. Chem. 2011, 57, 66–75. [Google Scholar] [CrossRef]
- Karschner, E.L.; Schwope, D.M.; Schwilke, E.W.; Goodwin, R.S.; Kelly, D.L.; Gorelick, D.A.; Huestis, M.A. Predictive model accuracy in estimating last Δ9-tetrahydrocannabinol (THC) intake from plasma and whole blood cannabinoid concentrations in chronic, daily cannabis smokers administered subchronic oral THC. Drug Alcohol Depend. 2012, 125, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Martin-Santos, R.; Crippa, J.A.; Batalla, A.; Bhattacharyya, S.; Atakan, Z.; Borgwardt, S.; Allen, P.; Seal, M.; Langohr, K.; Farre, M.; et al. Acute effects of a single, oral dose of d9-tetrahydrocannabinol (THC) and cannabidiol (CBD) administration in healthy volunteers. Curr. Pharm. Des. 2012, 18, 4966–4979. [Google Scholar] [CrossRef]
- Eichler, M.; Spinedi, L.; Unfer-Grauwiler, S.; Bodmer, M.; Surber, C.; Luedi, M.; Drewe, J. Heat exposure of Cannabis sativa extracts affects the pharmacokinetic and metabolic profile in healthy male subjects. Planta Med. 2012, 78, 686–691. [Google Scholar] [CrossRef] [Green Version]
- Lile, J.A.; Kelly, T.H.; Charnigo, R.J.; Stinchcomb, A.L.; Hays, L.R. Pharmacokinetic and pharmacodynamic profile of supratherapeutic oral doses of Δ(9)-THC in cannabis users. J. Clin. Pharmacol. 2013, 53, 680–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, N.; Kramer, W.G.; Khurana, V.; Cognata Smith, C.; Vetticaden, S. Bioavailability study of dronabinol oral solution versus dronabinol capsules in healthy volunteers. Clin. Pharmacol. 2016, 12, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherniakov, I.; Izgelov, D.; Barasch, D.; Davidson, E.; Domb, A.J.; Hoffman, A. Piperine-pro-nanolipospheres as a novel oral delivery system of cannabinoids: Pharmacokinetic evaluation in healthy volunteers in comparison to buccal spray administration. J. Control. Release 2017, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pellesi, L.; Licata, M.; Verri, P.; Vandelli, D.; Palazzoli, F.; Marchesi, F.; Cainazzo, M.M.; Pini, L.A.; Guerzoni, S. Pharmacokinetics and tolerability of oral cannabis preparations in patients with medication overuse headache (MOH)-a pilot study. Eur J. Clin. Pharmacol. 2018, 74, 1427–1436. [Google Scholar] [CrossRef]
- Pichini, S.; Mannocchi, G.; Gottardi, M.; Pérez-Acevedo, A.P.; Poyatos, L.; Papaseit, E.; Pérez-Mañá, C.; Farré, M.; Pacifici, R.; Busardò, F.P. Fast and sensitive UHPLC-MS/MS analysis of cannabinoids and their acid precursors in pharmaceutical preparations of medical cannabis and their metabolites in conventional and non-conventional biological matrices of treated individual. Talanta 2020, 209, 120537. [Google Scholar] [CrossRef]
- Timpone, J.G.; Wright, D.J.; Li, N.; Egorin, M.J.; Enama, M.E.; Mayers, J.; Galetto, G. The safety and pharmacokinetics of single-agent and combination therapy with megestrol acetate and dronabinol for the treatment of HIV wasting syndrome. The DATRI 004 Study Group. Division of AIDS Treatment Research Initiative. AIDS Res. Hum. Retroviruses 1997, 13, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Klumpers, L.E.; Beumer, T.L.; van Hasselt, J.G.; Lipplaa, A.; Karger, L.B.; Kleinloog, H.D.; Freijer, J.I.; de Kam, M.L.; van Gerven, J.M. Novel Δ-(9)-tetrahydrocannabinol formulation Namisol® has beneficial pharmacokinetics and promising pharmacodynamic effects. Br. J. Clin. Pharmacol. 2012, 74, 42–53. [Google Scholar] [CrossRef]
- Ahmed, A.I.; van den Elsen, G.A.; Colbers, A.; van der Marck, M.A.; Burger, D.M.; Feuth, T.B.; Rikkert, M.G.; Kramers, C. Safety and pharmacokinetics of oral delta-9-tetrahydrocannabinol in healthy older subjects: A randomized controlled trial. Eur. Neuropsychopharmacol. 2014, 24, 1475–1482. [Google Scholar] [CrossRef]
- de Vries, M.; Van Rijckevorsel, D.C.; Vissers, K.C.; Wilder-Smith, O.H.; Van Goor, H. Single dose delta-9-tetrahydrocannabinol in chronic pancreatitis patients: Analgesic efficacy, pharmacokinetics and tolerability. Br. J. Clin. Pharmacol. 2016, 81, 525–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohlsson, A.; Lindgren, J.E.; Wahlen, A.; Agurell, S.; Hollister, L.E.; Gillespie, H.K. Plasma delta-9 tetrahydrocannabinol concentrations and clinical effects after oral and intravenous administration and smoking. Clin. Pharmacol. Ther. 1980, 28, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Wachtel, S.R.; ElSohly, M.A.; Ross, S.A.; Ambre, J.; de Wit, H. Comparison of the subjective effects of Delta(9)-tetrahydrocannabinol and marijuana in humans. Psychopharmacology 2002, 161, 331–339. [Google Scholar] [PubMed]
- Newmeyer, M.N.; Swortwood, M.J.; Barnes, A.J.; Abulseoud, O.A.; Scheidweiler, K.B.; Huestis, M.A. Free and Glucuronide Whole Blood Cannabinoids' Pharmacokinetics after Controlled Smoked, Vaporized, and Oral Cannabis Administration in Frequent and Occasional Cannabis Users: Identification of Recent Cannabis Intake. Clin. Chem. 2016, 62, 1579–1592. [Google Scholar] [CrossRef] [Green Version]
- Newmeyer, M.N.; Swortwood, M.J.; Andersson, M.; Abulseoud, O.A.; Scheidweiler, K.B.; Huestis, M.A. Cannabis Edibles: Blood and Oral Fluid Cannabinoid Pharmacokinetics and Evaluation of Oral Fluid Screening Devices for Predicting Δ9-Tetrahydrocannabinol in Blood and Oral Fluid following Cannabis Brownie Administration. Clin. Chem. 2017, 63, 647–662. [Google Scholar] [CrossRef]
- Vandrey, R.; Herrmann, E.S.; Mitchell, J.M.; Bigelow, G.E.; Flegel, R.; LoDico, C.; Cone, E.J. Pharmacokinetic Profile of Oral Cannabis in Humans: Blood and Oral Fluid Disposition and Relation to Pharmacodynamic Outcomes. J. Anal. Toxicol. 2017, 41, 83–99. [Google Scholar] [CrossRef]
- Badowski, M.E. A review of oral cannabinoids and medical marijuana for the treatment of chemotherapy-induced nausea and vomiting: A focus on pharmacokinetic variability and pharmacodynamics. Cancer Chemother. Pharmacol. 2017, 80, 441–449. [Google Scholar] [CrossRef] [Green Version]
- Millar, S.A.; Stone, N.L.; Yates, A.S.; O’Sullivan, S.E. A Systematic Review on the Pharmacokinetics of Cannabidiol in Humans. Front. Pharmacol. 2018, 9, 1365. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| References | Study Design | Participants | Route of Administration | Formulation | Dose | Cmax (ng/mL) Mean ± SD, Median (Range) | Tmax (h) | Pharmacological Effects |
|---|---|---|---|---|---|---|---|---|
| Wall et al., 1983 [37] | OL, NP | 6 M, 6 F | Oral | Capsules | 20 mg THC (men) | Men | Men | Effects were not assessed. |
| THC: 14 ± 9.7 b | THC: 2.5 | |||||||
| 11-OH-THC: 6.6 ± 3.4 b | 11-OH-THC: 2.0 | |||||||
| 15 mg THC (women) | Women | Women | ||||||
| THC: 9.4 ± 4.5 b | THC: 1.75 | |||||||
| 11-OH-THC: 5.9 ± 2.8 b | 11-OH-THC: 1.75 | |||||||
| Intravenous (infusion pump) | Human serum albumin | 4 mg THC (men) | Men | Men | ||||
| THC: 71 ± 34 b | THC: 0.42 | |||||||
| 11-OH-THC: 3.7 ± 2.3 b | 11-OH-THC: 0.5 | |||||||
| 2.2 mg THC (women) | Women | Women | ||||||
| THC: 85 ± 26 b | THC: 0.17 | |||||||
| 11-OH-THC: 3.8 ± 2.8 b | 11-OH-THC: 0.33 | |||||||
| Haney et al., 2003 [38] | R, DB, P, C | 7 M Cannabis smokers | Oral | Capsules (Marinol®) | 30 mg THC29, Placebo naltrexone | THC: 29.9 ± 9.5 b | THC: 4 b | Subjective effects Increase in ratings of Good Drug Effect, High, and Stimulated. Vital effects Decreased HR. Worsened psychomotor performance. |
| THC-COOH: 121.9 ± 43.5 b | THC-COOH: 2 b | |||||||
| Oral | Capsules (Marinol®) | 30 mg THC 50 mg naltrexone | THC: 21.2 ± 8.6 b | THC: 2 b | ||||
| THC-COOH: 139.0 ± 36.2 b | THC-COOH: 3 b | |||||||
| Naef et al., 2003 [39] | R, DB, P, C | 6 M, 6 F Cannabis naïve | Oral | Capsules (Marinol®) | 20 mg THC | THC: 7.2 ± 6.9 b, e | THC: 1-2 b, e | Subjective effects Psychotropic and somatic side-effects were common but usually mild. Paint tests No significant reduction in pain. |
| 11-OH-THC: 19.7 ± 6.9 b, e | 11-OH-THC: 2 b, e | |||||||
| 11-COOH-THC: 241.4 ± 73. b, e | 11-COOH-THC: 2–4 b, e | |||||||
| Oral | Capsules | 20 mg THC 30 mg morphine HCl | THC: 6.7 ± 7.3 b, e | - | ||||
| 11-OH-THC: 7.9 ± 8.3 b, e | - | |||||||
| 11-COOH-THC: 134.7 ± 65.12 b, e | - | |||||||
| Oral | Capsules (placebo) | 30 mg morphine HCl | ||||||
| Oral | Capsules (placebo) | |||||||
| Guy et al., 2004 [40] | R, OL, C followed by an NR oral dose | 6 M, 6 F Previous experience of cannabis use | Oral | Capsules | 10 mg THC 10 mg CBD | THC: 6.35 ± 3.12 (3.04–4.55) | THC: 1.05 ± 0.65 (0.5–2.75) | Effects were not assessed. |
| CBD: 2.47 ± 2.23 (0.47–7.55) | CBD: 1.27 ± 0.84 (0.5–3) | |||||||
| 11-OH-THC: 7.87 ± 2.96 (4.79–13.64) | 11-OH-THC: 1.36 ± 0.63 (0.75–3) | |||||||
| Sublingual | Liquid spray (Sativex®) | 10 mg THC 10 mg CBD | THC: 5.54 ± 3.35 (1.14–12.13) | THC: 1.63 ± 0.59 (1–3) | ||||
| CBD: 2.50 ± 1.83 (0.27–6.55) | CBD: 1.63 ± 0.68 (0.75–3) | |||||||
| 11-OH-THC: 6.24 ± 2.74 (2.67–10.77) | 11-OH-THC: 1.58 ± 0.44 (1–2.75) | |||||||
| Buccal | Liquid spray (Sativex®) | 10 mg THC 10 mg CBD | THC: 6.14 ± 5.37 (0.88–19.78) | THC: 2.40 ± 1.08 (1–4.5) | ||||
| CBD: 3.02 ± 3.15 (0.29–9.91) | CBD: 2.78 ± 1.31 (1–4.5) | |||||||
| 11-OH-THC: 6.13 ± 2.88 (1.83–11.25) | 11-OH-THC: 2.40 ± 1.17 (1–4.5) | |||||||
| Oro-pharyngeal | Liquid spray (Sativex®) | 10 mg THC 10 mg CBD | THC: 6.11 ± 4.00 (1.94–15.68) | THC: 2.23 ± 1.52 (0.75–5) | ||||
| CBD: 2.61 ± 1.91 (0.41–6.36) | CBD: 2.04 ± 1.13 (0.75–5) | |||||||
| 11-OH-THC: 6.45 ± 2.91 (2.95–13.49) | 11-OH-THC: 2.40 ± 1.22 (1.25–5) | |||||||
| Menetrey et al., 2005 [41] | See also Table 2 for results on capsules and decoction administration. | |||||||
| Nadulski et al., 2005 [42] | DB, P, C | 24 | Oral | Capsules | 10 mg THC 5.4 mg CBD | THC: 4.05 (1.18–10.27) | THC: 0.93 (0.55–2.08) | Effects were not assessed. |
| CBD: 0.95 (0.30–2.57) | CBD: 0.99 (0.5–2) | |||||||
| 11-OH-THC: 4.88 (1.83–12.34) | 11-OH-THC: 1.67 (0.62–2.17) | |||||||
| THC-COOH:35.46 (19.2–70.6) | THC-COOH: 1.92 (1.08–3.83) | |||||||
| Oral | Capsules | 10 mg THC | THC: 3.20 (0.67–7.99) | THC: 1.06 (0.5–3.05) | ||||
| 11-OH-THC: 4.48 (1.12–11.14) | 11-OH-THC: 1.5 (0.5–3.17) | |||||||
| THC-COOH: 32.9 (12.03–57.63) | THC-COOH: 2.07 (0.62–3.92) | |||||||
| Oral | Capsules | Placebo | ||||||
| Goodwin et al., 2006 [43] | See also Table 2 for results on capsules and oil administration. | |||||||
| Schwilke et al., 2009 [44] | NR, OL, NP, MD | 6 M Daily smokers (positive in cannabinoids, smoked within the previous 24 h) | Oral | Capsules (Marinol®) | Escalating total daily doses (40-120 mg) for 7 days First dose 20 mg THC | After 1st dose (single dose): | After 1st dose: | Effects were not assessed. |
| THC: 12.4 ± 3.4 | THC: 2.8 (0.33) | |||||||
| 11-OH-THC: 8.2 ± 2.0 | 11-OH-THC: 2.5 (0.18) | |||||||
| THC-COOH: 75.8 ± 9.4 | THC-COOH: 3.3 (0.56) | |||||||
| Karschner et al., 2011 [45] | R, DB, P, DD | 6 M, 3 F Cannabis smokers | Oral | Capsules (dronabinol) | 5 mg THC | THC: 4.7 ± 0.9, 4.6 (1.4–10.4) | THC: 3.2 ± 0.3, 3.1 (1.5–4.5) | Effects were not assessed. |
| 11-OH-THC: 3.0 ± 0.4, 2.6 (1.8–5.9) | 11-OH-THC: 3.3 ± 0.4, 3.3 (1.5–5.6) | |||||||
| THC-COOH: 69.3 ± 17.6, 57.1 (15.9–179.7) | THC-COOH: 4.4 ± 0.5, 4.3 (2.7–7.5) | |||||||
| Oral | Capsules (dronabinol) | 15 mg THC | THC: 14.3 ± 2.7, 11.2 (3.3–28.5) | THC: 3.4 ± 0.5, 3.4 (1.2–5.5) | ||||
| 11-OH-THC: 11.1 ± 2.0, 9.3 (3.6–19.5) | 11-OH-THC: 3.4 ± 0.4, 3.6 (1.0–5.5) | |||||||
| THC-COOH: 133.6 ± 36.3, 102.1 (44.5–409.0) | THC-COOH: 4.9 ± 0.5, 5.5 (2.4–7.5) | |||||||
| Sublingual | Spray (Sativex®) | 5.4 mg THC 5.0 mg CBD | THC: 5.1 ± 1.0, 5.1 (1.2–9.6) | THC: 3.3 ± 0.3, 3.5 (1.2–4.5) | ||||
| CBD: 1.6 ± 0.4, 1.2 (0.6–3.9) | CBD: 3.7 ± 0.5, 3.6 (1.0–5.5) | |||||||
| 11-OH-THC: 4.2 ± 0.7, 3.7 (2.1– 7.5) | 11-OH-THC: 3.6 ± 0.6, 3.3 (1.0–7.5) | |||||||
| THC-COOH: 108.0 ± 30.5, 79.8 (19.1–281.6) | THC-COOH: 4.4 ± 0.7, 4.5 (1.2–7.5) | |||||||
| Sublingual | Spray (Sativex®) | 16.2 mg THC 15.0 mg CBD | THC: 15.3 ± 3.4, 14.5 (3.2–38.2) | THC: 4.0 ± 0.5, 4.5 (1.2–5.6) | ||||
| CBD: 6.7 ± 2.0, 3.7 (2.0–20.5) | CBD: 4.0 ± 0.5, 4.5 (1.2–5.6) | |||||||
| 11-OH-THC: 8.4 ± 1.2, 7.6 (3.8–13.7) | 11-OH-THC: 3.9 ± 0.5, 3.7 (1.2–5.6) | |||||||
| THC-COOH: 126.6 ± 25.9, 92.4 (55.9–304.1) | THC-COOH: 4.8 ± 0.3, 5.0 (2.6–5.6) | |||||||
| Karschner et al., 2012 [46] | NR, OL, NP, MD | 10 M Daily smokers (positive cannabinoids, smoked within the previous 24 h) | Oral | Capsules (Marinol®) | Escalating total daily doses (40-120 mg) for 7 days Each dose of 20 mg THC | After 1st dose (single dose): | After 1st dose: | Effects were not assessed. |
| THC: 8.7 ± 4.8, 6.4 (4.1–17.5) | THC: 3.0 ± 0.9, 3.0 (2.0–4.0) | |||||||
| 11-OH-THC: 4.0 ± 2.1, 3.4 (1.8–7.8) | 11-OH-THC: 2.8 ± 0.9, 3.0 (2.0–5.0) | |||||||
| THC-COOH: 38.4 ± 15.9, 36.6 (19.7–68.7) | THC-COOH: 3.1 ± 1.0, 3.0 (2.0–5.0) | |||||||
| Martin-santos et al., 2012 [47] | R, DB, P, C | 16 M Previous experience of cannabis use (less than 15 times in their lifetime) | Oral | Capsules | 10 mg THC | THC: 0.67 ± 0.66 b THC-COOH: ≈ 5.6 b, d 11-OH-THC: ≈ 0.73 b, d | THC: 2 h b | Subjective effects Significant changes in PANSS, anxiety (STAI-S), dysphoria (ARCI), sedation (VAMS, ARCI), and the level of subjective intoxication (ASI, ARCI). Vital effects Significant increase in HR No significant differences in SBP and DBP. |
| Oral | Capsules | 600 mg CBD | ||||||
| Oral | Capsules (placebo) | |||||||
| Eichler et al., 2012 [48] | R, DB, C | 9 M Non smokers | Oral | Capsules (Marinol®) | 20 mg THC | THC: 1.03 ± 1.65, 0.48 e, g | THC: 1.06 ± 0.19, 1.0 e | Subjective effects Mild psychotropic effects, with no significant differences between treatments. |
| CBD: 0.00 ± 0.00, 0.0 e, g | CBD: NA | |||||||
| 11-OH-THC: 0.99 ± 0.63, 0.84 e, g | 11-OH-THC: 1.67 ± 0.51, 2.0 e | |||||||
| THC-COOH: 7.13 ± 5.64, 7.61 e, g | THC-COOH: 1.78 ± 0.96, 2.0 e | |||||||
| CBN: 0.64 ± 0.72, 0.37 e, g | CBN: 1.06 ± 0.57, 1.0 e | |||||||
| Oral | Capsules (extract from heated Herba Cannabis) | 17.6 mg THC 27.8 mg CBD | THC: 0.42 ± 0.39, 0.25 e, g | THC: 0.78 ± 0.27, 1.0 e | ||||
| CBD: 0.30 ± 0.21, 0.27 e, g | CBD: 0.83 ± 0.51, 0.5 e | |||||||
| 11-OH-THC: 0.73 ± 0.69, 0.50 e, g | 11-OH-THC: 1.44 ± 0.69, 2.0 e | |||||||
| THC-COOH: 5.81 ± 7.59, 3.46 e, g | THC-COOH: 2.89 ± 1.05, 2.0 e | |||||||
| CBN: 0.60 ± 0.36, 0.56 e, g | CBN: 0.94 ± 0.45, 1.0 e | |||||||
| Oral | Capsules (extract from unheated Herba Cannabis) | 10.4 mg THC 14.8 mg CBD | THC: 1.02 ± 0.78, 0.71 e, g | THC: 1.17 ± 0.66, 1.0 e | ||||
| CBD: 1.24 ± 0.87, 0.96 e, g | CBD: 1.17 ± 1.17, 1.0 e | |||||||
| 11-OH-THC: 0.57 ± 0.42, 0.50 e, g | 11-OH-THC: 1.00 ± 0.42, 1.0 e | |||||||
| THC-COOH: 1.94 ± 1.11, 2.28 e, g | THC-COOH: 2.11 ± 0.78, 2.0 e | |||||||
| CBN: 0.54 ± 0.30, 0.58 e, g | CBN: 1.00 ± 0.42, 1.0 e | |||||||
| Lile JA et al., 2013 [49] | B, P, C | 4 M, 3 F Only 5 completed all doses Regular cannabis use | Oral | Capsules (Marinol®) | 15 mg THC | THC: ≈5 d | THC: 3 d | Vital effects Increase in HR. SBP decreased after 30 mg dose but increased after 75 and 90 mg doses. No changes in DBP. Decrease in finger temperature. Psychomotor performance Worsened psychomotor performance. |
| 11-OH-THC: ≈2-3 d | 11-OH-THC: 3 d | |||||||
| Oral | Capsules (Marinol®) | 30 mg THC | THC: ≈10 d | THC: 3 d | ||||
| 11-OH-THC: ≈5 d | 11-OH-THC: 3 d | |||||||
| Oral | Capsules (Marinol®) | 45 mg THC | THC: ≈17–18 d | THC: 2.5 d | ||||
| 11-OH-THC: ≈8–9 d | 11-OH-THC: 2 d | |||||||
| Oral | Capsules (Marinol®) | 60 mg THC | THC: ≈45 d | THC: 3.5 d | ||||
| 11-OH-THC: ≈11 d | 11-OH-THC: 3 d | |||||||
| Oral | Capsules (Marinol®) | 75 mg THC | THC: ≈42–43 d | THC: 4 d | ||||
| 11-OH-THC: ≈12–13 d | 11-OH-THC: 4 d | |||||||
| Oral | Capsules (Marinol®) | 90 mg THC | THC: ≈53 d | THC: 4 d | ||||
| 11-OH-THC: ≈20 d | 11-OH-THC: 4 d | |||||||
| Oral | Capsules (placebo) | |||||||
| Parikh et al., 2016 [50] | R, OL, C | 51 MF No cannabis use in the previous 90 days | Oral | Oral solution (Dronabinol) | 4.25 mg THC | THC Replicate 1: 1.81 ± 1.26 | THC Replicate 1: 1.50 (0.50–4.00) | Effects were not assessed. |
| THC Replicate 2: 2.08 ± 1.30 | THC Replicate 2: 1.00 (0.50–3.02) | |||||||
| 11-OH-THC Replicate 1: 2.53 ± 1.38 | 11-OH-THC Replicate 1: 1.50 (0.75–4.00) | |||||||
| 11-OH-THC Replicate 2: 3.01 ± 1.56 | 11-OH-THC Replicate 2: 1.50 (0.50–3.02) | |||||||
| Oral | Capsules (Dronabinol) | 5 mg THC | THC Replicate 1: 2.20 ± 1.51 THC Replicate 2: 2.61 ± 1.69 11-OH-THC Replicate: 3.28 ± 1.78 11-11-OH-THC Replicate 2: 3.98 ± 2.51 | THC Replicate 1: 1.00 (0.50–6.00) THC Replicate 2: 1.50 (0.50–6.00) 11-OH-THC Replicate 1: 1.60 (0.75–6.00) 11-OH-THC Replicate 2: 1.50 (0.50–6.00) | ||||
| Cherniakov et al., 2017 [51] | OL, C | 9 M Not exposed within the previous 4 weeks | Sublingual | Spray (Sativex®) | 10.8 mg THC 10.0 mg CBD | THC: 1.8 ± 0.2 | THC: 2 (1–4) | Effects were not assessed. |
| CBD: 0.5 ± 0.1 | CBD: 3 (1–5) | |||||||
| Oral | THC-CBD-piperine-PNL capsule | 10.8 mg THC 10.0 mg CBD | THC: 5.4 ± 0.01 | THC: 1 (1–1.5) | ||||
| CBD: 2.1 ± 0.4 | CBD: 1 (0.5–1.5) | |||||||
| References | Study Design | Participants | Route of Administration | Formulation | Dose | Cmax (ng/mL) Mean ± SD, Median (Range) | Tmax (h) | Pharmacological Effects |
|---|---|---|---|---|---|---|---|---|
| Menetrey et al., 2005 [41] | R, DB, P, C | 8 M Occasional cannabis smokers | Oral | Milk decoction | 16.5 mg THC | THC: 3.8 (1.5–8.3) b | THC: 1 b | Subjective effects Prototypical effects of THC with a strong feeling of highness. Vital effects Slight to moderate conjunctival reddening. Slight to moderate tachycardia Increase of HR after decoction. |
| 11-OH-THC: 4.7 (2.9–7.0) b | 11-OH-THC: 1 b | |||||||
| THC-COOH: 27.8 (14.1–42.4) b | THC-COOH: 4 b | |||||||
| Oral | Milk decoction | 45.7 mg THC | THC: 8.4 (3.9–13.1) b | THC: 1 b | ||||
| 11-OH-THC: 12.8 (3.4–24.7) b | 11-OH-THC: 2.5 b | |||||||
| THC-COOH: 66.2 (29.0–99) b | THC-COOH: 2.5 b | |||||||
| Oral | Capsules (Marinol®) | 20 mg THC | THC: 2.8 (nd–5.6) b | THC: 1 b | ||||
| 11-OH-THC: 3.9 (1.4–8.5) b | 11-OH-THC: 4 b | |||||||
| THC-COOH: 27.8 (5.4–55.4) b | THC-COOH: 5.5 b | |||||||
| Oral | Decoction (placebo) | 0.8 mg THC | ||||||
| Oral | Capsules (placebo) | |||||||
| Goodwin et al., 2006 [43] | R, DB, P, DD, MD (5 days) | 6 Previous experience of cannabis use | Oral | Hemp oil | 0.39 mg THC/day (tablespoon) | THC: 0 f (0.0–0.0) | THC: 0.0 f (0.0–0.0) | Subjective effects Mild prototypical effects of THC. Vital effects No difference in BP, HR, and respiratory rate. |
| 11-OH-THC: 0 f (0.0–0.0) | 11-OH-THC: 0.0 f (0.0–0.0) | |||||||
| THC-COOH: 1.1 f (0.0–3.1) | THC-COOH: 49.7 f (4.5–121) | |||||||
| Oral | Capsules (hemp oil) | 0.47 mg THC/day | THC: 0.0 f (0.0–0.0) | THC: 0.0 f (0.0–0.0) | ||||
| 11-OH-THC: 0.0 f (0.0–0.0) | 11-OH-THC: 0.0 f (0.0–0.0) | |||||||
| THC-COOH: 1.4 f (0.0–2.6) | THC-COOH: 65.3 f (11.0–107) | |||||||
| Oral | Capsules (dronabinol) | 7.5 mg THC/day | THC: 1.5 f (0.6–3.8) | THC: 57.6 f (6.5–107) | ||||
| 11-OH-THC: 1.6 f (0.0–2.6) | 11-OH-THC: 85.9 f (1.5–107) | |||||||
| THC-COOH: 19.8 f (10.6–43.0) | THC-COOH: 107 f (107–107) | |||||||
| Oral | Hemp oil | 14,8 mg THC/day | THC: 2.1 f (0.7–6.1) | THC: 56.5 f (9–107) | ||||
| 11-OH-THC: 1.7 f (0.0–5.6) | 11-OH-THC: 28.6 f (6.5–107) | |||||||
| THC-COOH: 12.7 f (11.0–15.2) | THC-COOH: 91.5 f (11.5–121) | |||||||
| Oral | Placebo | |||||||
| Pellesi et al., 2018 [52] | OL, C | 6 M, 7 F Patients with medication overuse headaches | Oral | Decoction | 1.85 ± 1.6 mg THC | THC: 1.38 ± 0.75 | THC: 1.28 ± 0.51 | Subjective effects Intensity of subjective effects was similar in both formulations. Increased drowsiness after cannabis oil administration. Vital effects No changes in BP and HR. |
| 2.22 ± 0.66 mg THCA-A | THCA: 48.92 ± 26.34 | THCA: 1.22 ± 0.26 | ||||||
| 1.93 ± 1.17 mg CBD | CBD: 4.39 ± 3.01 | CBD: 0.56 ± 0.17 | ||||||
| 8.82 ± 2.02 mg CBDA | CBDA: 74.61 ± 25.15 | CBDA: 0.83 ± 0.35 | ||||||
| Oral | Oil | 2.2 mg THC | THC: 3.29 ± 1.39 | THC: 1.28 ± 0.36 | ||||
| 2.3 mg THCA-A | THCA: 65.36 ± 20.40 | THCA: 1.33 ± 0.35 | ||||||
| 2.4 mg CBD | CBD: 3.14 ± 2.58 | CBD:1 ± 0.25 | ||||||
| 4.4 mg CBDA | CBDA: 55.03 ± 29.45 | CBDA: 1.06 ± 0.3 | ||||||
| Pichini et al., 2020 [53] | NR, OL, NP Pilot | 1 M | Oral | Decoction | 0.36 mg THC 1.6 mg THCA-A 0.42 mg CBD 4 mg CBDA | Blood | Blood | Effects were not reported. |
| THC: 1.0 | THC: 2.0 | |||||||
| THCA-A: 72.4 | THCA-A: 2.0 | |||||||
| CBD: 1.5 | CBD: 3.0 | |||||||
| CBDA: 94.3 | CBDA: 0.5 | |||||||
| 11-OH-THC: 1.2 | 11-OH-THC: 2.0 | |||||||
| THC-COOH: 17.1 | THC-COOH: 3.0 | |||||||
| THC-COOH-GLUC: 40.2 | THC-COOH-GLUC: 4.0 | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 0.2 | THC: 0.5 | |||||||
| THCA-A: 5.1 | THCA-A: 0.5 | |||||||
| CBD: 0.8 | CBD: 0.5 | |||||||
| CBDA: 145.2 | CBDA: 0.5 | |||||||
| Oral | Oil | 0.95 mg THC 1.5 mg THCA-A 0.86 mg CBD 2.8 mg CBDA | Blood | Blood | ||||
| THC: 0.5 | THC: 2.0 | |||||||
| THCA: 40.3 | THCA-A: 2.0 | |||||||
| CBD: 0.3 | CBD: 2.0 | |||||||
| CBDA: 32.4 | CBDA: 1.5 | |||||||
| 11-OH-THC: 0.7 | 11-OH-THC: 2.0 | |||||||
| THC-COOH: 4.3 | THC-COOH: 2.0 | |||||||
| THC-COOH-GLUC: 7.7 | THC-COOH-GLUC: 3.0 | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 0.2 | THC: 2 | |||||||
| THCA: 1.0 | THCA-A: 2 | |||||||
| CBD: 0.6 | CBD: 2 | |||||||
| CBDA: 14.3 | CBDA: 1 |
| References | Study Design | Participants | Route of Administration | Formulation | Dose | Cmax (ng/mL) Mean ± SD, Median (Range) | Tmax (h) | Pharmacological Effects |
|---|---|---|---|---|---|---|---|---|
| Timpone et al., 1997 [54] | R, OL | 7 M/F 4 M/F 9 M/F Patients with HIV wasting syndrome | Oral | Tablets (Marinol®) | 2.5 mg THC | Data from all 20 patients | Data from all 20 patients | Subjective effects Increase in VAS for hunger. No differences in VAS for mood and nausea. |
| Oral | Tablets (Marinol®) | 2.5 mg THC 750 mg megestrol | THC: 2.01 c (0.58–12.48) | THC: 2.07 b (0.66–8.26) | ||||
| Oral | Tablets (Marinol®) | 2.5 mg THC 250 mg megestrol | 11-OH-THC: 4.61 c (0.52–37.5) | 11-OH-THC: 2.07 b (0.49–8.00) | ||||
| Klumpers et al., 2011 [55] | R, DB, DD, P, C | 4 M, 5 F (in panel 1, 13 subjects) Previous experience of cannabis use (maximum 1 use per week) | Sublingual | Tablets (Namisol®) | 5.0 mg THC | 2.30 ± 1.01 e | 1.24 ± 0.65 e | Subjective effects Highest oral doses increased body sway and VAS for calmness, external perception, and feeling high and decreased VAS for alertness. Vital effects No significant differences in PD parameters between oral and sublingual administration. Significant increase in HR. |
| Oral | Tablets (Namisol®) | 5.0 mg THC | 2.92 ± 1.49 e | 0.93 ± 0.68 e | ||||
| Oral | Tablets (Namisol®) | 6.5 mg THC | 4.43 ± 1.86 e | 0.66 ± 0.13 e | ||||
| Oral | Tablets (Namisol®) | 8.0 mg THC | 4.69 ± 2.91 e | 0.73 ± 0.19 e | ||||
| Oral | Tablets (placebo) | |||||||
| Ahmed et al., 2014 [56] | R, DB, P, DD, C | 6 M, 5 F | Oral | Tablets (Namisol®) | 3 mg THC | 1.42 (0.53–3.48) | 0.92 (0.67–0.92) | Subjective effects No subjective effects (exc. 4 subjects “felt high”) Vital effects Mild PD effects. No changes in SBP, DBP, and HR. Psychomotor performance No changes in psychomotor performance. |
| Oral | Tablets (Namisol®) | 5 mg THC | 3.15 (1.54–6.95) | 0.92 (0.67–0.92) | ||||
| Oral | Tablets (Namisol®) | 6.5 mg THC | 4.57 (2.11–8.65) | 0.67 (0.67–0.92) | ||||
| Oral | Tablets (placebo) | |||||||
| De Vries et al., 2016 [57] | R, DB, P, C | 15 M, 9 F Patients diagnosed with chronic pancreatitis No cannabis use in previous year | Oral | Tablets (Namisol®) | 8 mg THC | THC: 4.01 ± 3.39 | 2.05 + 1.47 | Subjective effects No differences in subjective effects (alertness, mood, calmness, or balance) between treatments. Anxiousness, somnolence, dry mouth, dizziness, and euphoric mood after THC administration. Vital effects No changes in SBP and DBP. THC induced an increase in HR compared to diazepam. |
| 11-OH-THC: 4.38 ± 1.50 | 2.26 ± 1.29 | |||||||
| Oral | Tablet (active placebo) | 5 mg diazepam to non-opioid group/10 mg diazepam to opioid group |
| References | Study Design | Participants | Route of Administration | Formulation | Dose | Cmax (ng/mL) Mean ± SD, Median (Range) | Tmax (h) | Pharmacological Effects |
|---|---|---|---|---|---|---|---|---|
| Ohlsson et al., 1980 [58] | R, OL, NP, C | 11 M Previous experience of cannabis use (from infrequent to frequent use) | Smoked | Cigarette | 19 mg THC (ad libitum) (mean = 13.0 mg) | 77, 33–118 a | Subjective effects Increase in high effect. Vital effects Increase in HR. Conjunctival reddening | |
| Oral | Chocolate cookie | 20 mg THC | 4.4–11 a | 1–1.5 | ||||
| Intravenous | Normal saline ethanolic solution | 5 mg THC | 219, 161–316 a | |||||
| Watchel et al., 2002 [59] | DB, P, C | 7 M, 5 F 7 M, 6 F Previous experience of cannabis use | Oral | Cannabis (plant) brownie | 8.4 mg THC | ≈ 4.1 b, d | 3 b, d | Subjective effects Both drugs increased VAS sedation and ARCI PCAG scale scores, and decreased the ARCI BG scale scores at higher doses. Cannabis in high doses increased VAS for sedation, drowsiness, and tiredness. THC in high doses increased ARCI A scale scores, MBG (euphoria), and LSD (dysphoria). Vital effects No effects on physiological or behavioral measures. |
| Oral | Cannabis (plant) brownie | 16.9 mg THC | ≈ 6.8 b, d | 2.5 b, d | ||||
| Oral | THC (synthetic) brownie | 8.4 mg THC | ≈ 4.8 b, d | 2.5 b, d | ||||
| Oral | THC (synthetic) brownie | 16.9 mg THC | ≈ 9 b, d | 2.5 b, d | ||||
| Smoked | Cannabis (plant) cigarette | 8.4 mg THC | ≈ 36 b, d | 0.08 b, d | ||||
| Smoked | Cannabis (plant) cigarette | 16.9 mg THC | ≈ 60 b, d | 0.08 b, d | ||||
| Smoked | THC (synthetic) cigarette | 8.4 mg THC | ≈ 31 b, d | 0.08 b, d | ||||
| Smoked | THC (synthetic) cigarette | 16.9 mg THC | ≈ 56 b, d | 0.08 b, d | ||||
| Oral | Brownie (placebo) | |||||||
| Smoked | Cigarette (placebo) | |||||||
| Newmeyer et al., 2016 [60] | R, DB, P, DD, C | 9 M, 2 F frequent smokers 6 M, 3 F occasional smokers | Oral | Brownie | 50.6 mg THC (ad libitum) 1.5 mg CBD 3.3 mg CBN | Frequent smokers | Frequent smokers | Effects were not described. |
| THC: 15.3, 14.3 (1.4–32.4) | THC: 2.5, 2.5 (1.5–3.5) | |||||||
| 11-OH-THC: 7.3, 6.2 (0.9–13.7) | 11-OH-THC: 2.3, 2.5 (1.5–3.5) | |||||||
| THC-COOH: 36.4, 35.3 (4.3–99.4) | THC-COOH: 2.7, 2.5 (2.5–3.5) | |||||||
| THCV-COOH: 2.1, 2.0 (1.1–3.4) | THCV-COOH: 3.0, 3.0 (2.5–3.5) | |||||||
| THC-COOH-gluc: 53.0, 57.1 (10.3–75.7) | THCOOH-gluc: 3.4, 3.5 (1.5–5.0) | |||||||
| Occasional smokers | Occasional smokers | |||||||
| THC: 10.3, 10.1 (3.6–22.5) | THC: 2.3, 2.5 (1.5–3.5) | |||||||
| 11-OH-THC: 5.5, 5.1 (2.4–11.0) | 11-OH-THC: 2.4, 2.5 (1.5–3.5) | |||||||
| THC-COOH: 39.8, 37.8 (12.5–70.4) | THC-COOH: 2.9, 3.5 (1.5–3.5) | |||||||
| THCV-COOH: 1.9, 1.9 (1.1–2.7) | THCV-COOH: 2.6, 2.5 (1.5–3.5) | |||||||
| THC-COOH-gluc: 124, 124 (70.9–178) | THC-COOH-gluc: 4.7, 5.0 (3.5–5.0) | |||||||
| Smoked | Cigarette | 50.6 mg THC (ad libitum) 1.5 mg CBD 3.3 mg CBN | Frequent smokers | Frequent smokers | ||||
| THC: 151, 114 (51.6–467) | THC: 0.12, 0.13 (0.00–0.17) | |||||||
| 11-OH-THC: 9.0, 6.5 (1.9–30.2) | 11-OH-THC: 0.21, 0.20 (0.10–0.50) | |||||||
| THC-COOH: 23.5, 20.0 (5.7–64.9) | THC-COOH: 0.28, 0.25 (0.00–0.50) | |||||||
| THCV-COOH: 2.4, 2.4 (1.8–3.1) | THCV-COOH: 0.22, 0.23 (0.17–0.25) | |||||||
| THC-COOH-gluc: 25.8, 14.1 (5.0–70.7) | THC-COOH-gluc: 1.1, 0.5 (0.0–3.5) | |||||||
| Occasional smokers | Occasional smokers | |||||||
| THC: 51.6, 44.4 (1.3–174) | THC: 0.11, 0.10 (0.07–0.17) | |||||||
| 11-OH-THC: 2.8, 1.9 (0.5–8.7) | 11-OH-THC: 0.22, 0.19 (0.10–0.50) | |||||||
| THC-COOH: 8.4, 7.4 (0.7–17.5) | THC-COOH: 0.31, 0.25 (0.10–0.50) | |||||||
| THCV-COOH: - | THCVCOOH: - | |||||||
| THC-COOH-gluc: 19.4, 21.4 (11.8–25.0) | THC-COOH-gluc: 2.1, 1.5 (1.5–3.5) | |||||||
| Inhaled | Vaporizer Volcano | 50.6 mg THC (ad libitum) 1.5 mg CBD 3.3 mg CBN | Frequent smokers | Frequent smokers | ||||
| THC: 84.7, 83.1 (23.5–169) | THC: 0.09, 0.10 (0.03–0.17) | |||||||
| 11-OH-THC: 4.8, 4.2 (1.6–9.8) | 11-OH-THC: 0.19, 0.17 (0.10–0.50) | |||||||
| THC-COOH: 13.0, 12.5 (4.1–31.3) | THC-COOH: 0.25, 0.25 (0.13–0.50) | |||||||
| THCV-COOH: 1.7, 1.8 (1.2–2.1) | THCV-COOH: 0.52, 0.21 (0.17–1.5) | |||||||
| THC-COOH-gluc: 10.9, 10.6 (0.8–23.8) | THC-COOH-gluc: 1.8, 1.5 (0.03–3.5) | |||||||
| Occasional smokers | Occasional smokers | |||||||
| THC: 47.8, 34.8 (5.2–137) | THC: 0.11, 0.10 (0.03–0.17) | |||||||
| 11-OH-THC: 2.0, 1.6 (0.7–3.5) | 11-OH-THC: 0.15, 0.15 (0.10–0.20) | |||||||
| THC-COOH: 7.2, 5.3 (1.4–15.9) | THC-COOH: 0.33, 0.25 (0.20–0.50) | |||||||
| THCV-COOH: - | THCV-COOH: - | |||||||
| THC-COOH-gluc: 15.1, 16.1 (5.3–23.7) | THC-COOH-gluc: 1.9, 2.5 (0.5–2.5) | |||||||
| Oral | Brownie (placebo) | |||||||
| Smoked | Cigarette (placebo) | |||||||
| Inhaled | Vaporizer (placebo) | |||||||
| Newmeyer et al., 2017 [61] | Optional dosing session under the same clinical protocol followed in Newmeyer et al., 2016 | 9 M frequent smokers 5 M, 2 F occasional smokers | Oral | Brownie | 50.6 mg THC 1.5 mg CBD 3.3 mg CBN (ad libitum) | Frequent smokers | Frequent smokers | Effects were not assessed. |
| Blood | Blood | |||||||
| THC: 16.2, 12.8 (5.3–34.6) | THC: 2.5, 3.5 (1.0–3.5) | |||||||
| 11-OH-THC: 58.4, 50.0 (27.8–152) | 11-OH-THC: 2.8, 3.5 (1.0–3.5) | |||||||
| THC-COOH: 58.4, 50.0 (27.8–152) | THC-COOH: 3.3, 3.5 (1.5–3.5) | |||||||
| THCV-COOH: 1.9, 1.6 (1.1–3.9) | THCV-COOH: 3.1, 3.5 (1.5–3.5) | |||||||
| THC-COOH-gluc: 68.5, 61.2 (50.6–110) | THC-COOH-gluc: 4.8, 5.0 (3.5–8.0) | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 573, 464 (39.3–2111) | THC: 0.33 | |||||||
| 11-OH-THC: 0.6, 0.7 (0.2–1.2) | 11-OH-THC: 0.40, 0.33 (0.33–1.0) | |||||||
| THC-COOH: 285, 186 (123–849) | THC-COOH: 12, 5 (3.5–48) | |||||||
| THCV-COOH: 7.4, 6.8 (1.3–19.4) | THCV-COOH: 0.33 | |||||||
| Occasional smokers | Occasional smokers | |||||||
| Blood | Blood | |||||||
| THC: 8.2, 8.6 (3.2–14.3) | THC: 2.2, 1.5 (1.0–5.0) | |||||||
| 11-OH-THC: 5.6, 5.2 (4.1–8.6) | 11-OH-THC: 2.6, 3.5 (1.5–3.5) | |||||||
| THC-COOH: 39.7, 38.2 (26.5–61.2) | THC-COOH: 3.2, 3.5 (1.5–3.5) | |||||||
| THCV-COOH: 1.6, 1.6 (1.1–2.1) | THCVCOOH: 2.3, 1.5 (1.0–3.5) | |||||||
| THC-COOH-gluc: 86.2, 73.5 (43.1–183) | THCOOH-gluc: 4.6, 5.0 (3.5–6.0) | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 362, 392 (115–696) | THC: 0.33 | |||||||
| 11-OH-THC: 0.4, 0.4 (0.3–0.6) | 11-OH-THC: 0.60, 0.33 (0.33–1.5) | |||||||
| THC-COOH: 315, 191 (27.9–1263) | THC-COOH: 10, 10 (0.33–20) | |||||||
| THCV-COOH: 5.4, 4.7 (1.6–10.6) | THCV-COOH: 0.33 | |||||||
| Vandrey et al., 2017 [62] | R, DB, NP | 9 M, 9 F Previous experience of cannabis use but not exposed within the previous 3 months | Oral | Brownie | 10 mg THC | Blood | Blood | Subjective effects Significant subjective and cognitive drug effects at the 25 and 50 mg doses. Vital effects Significant PD effects. Psychomotor performance Significant effects on psychomotor performance at the 25 and 50 mg doses. |
| THC: 1.0 (0–3) | THC: 0.9 (0–2) | |||||||
| 11-OH-THC: 1.0 (0–2) | 11-OH-THC: 1.3 (0–3) | |||||||
| THC-COOH: 7.2 (5–14) | THC-COOH: 3.2 (2–4) | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 191.5 (47–412) | THC: 0.2 (0.2–0.5) | |||||||
| THC-COOH: 0.051 (0–0.231) | THC-COOH: 1.0 (0–3) | |||||||
| Oral | Brownie | 25 mg THC | Blood | Blood | ||||
| THC: 3.5 (3.0–4) | THC: 2.6 (1.0–4) | |||||||
| 11-OH-THC: 3.3 (2–5) | 11-OH-THC: 3.0 (1.5–4) | |||||||
| THC-COOH: 21.3 (12–39) | THC-COOH: 3.3 (1.5–6) | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 477.5 (70–1128) | THC: 0.2 (0.2–0.5) | |||||||
| THC-COOH: 0.140 (0.023–0.251) | THC-COOH: 9.8 (3–30) | |||||||
| Oral | Brownie | 50 mg THC | Blood | Blood | ||||
| THC: 3.3 (1.0–5) | THC: 2.3 (1.0–6) | |||||||
| 11-OH-THC: 3.2 (2–4) | 11-OH-THC: 1.8 (1–3) | |||||||
| THC-COOH: 29.3 (16–44) | THC-COOH: 3.3 (1.5–6) | |||||||
| Oral fluid | Oral fluid | |||||||
| THC: 597.5 (350–1010) | THC: 0.2 (0.2–0.5) | |||||||
| THC-COOH: 0.314 (0–0.822) | THC-COOH: 17.4 (0–54) |
| Capsules | Decoction | Oil | Tablets | Baked Goods | |
|---|---|---|---|---|---|
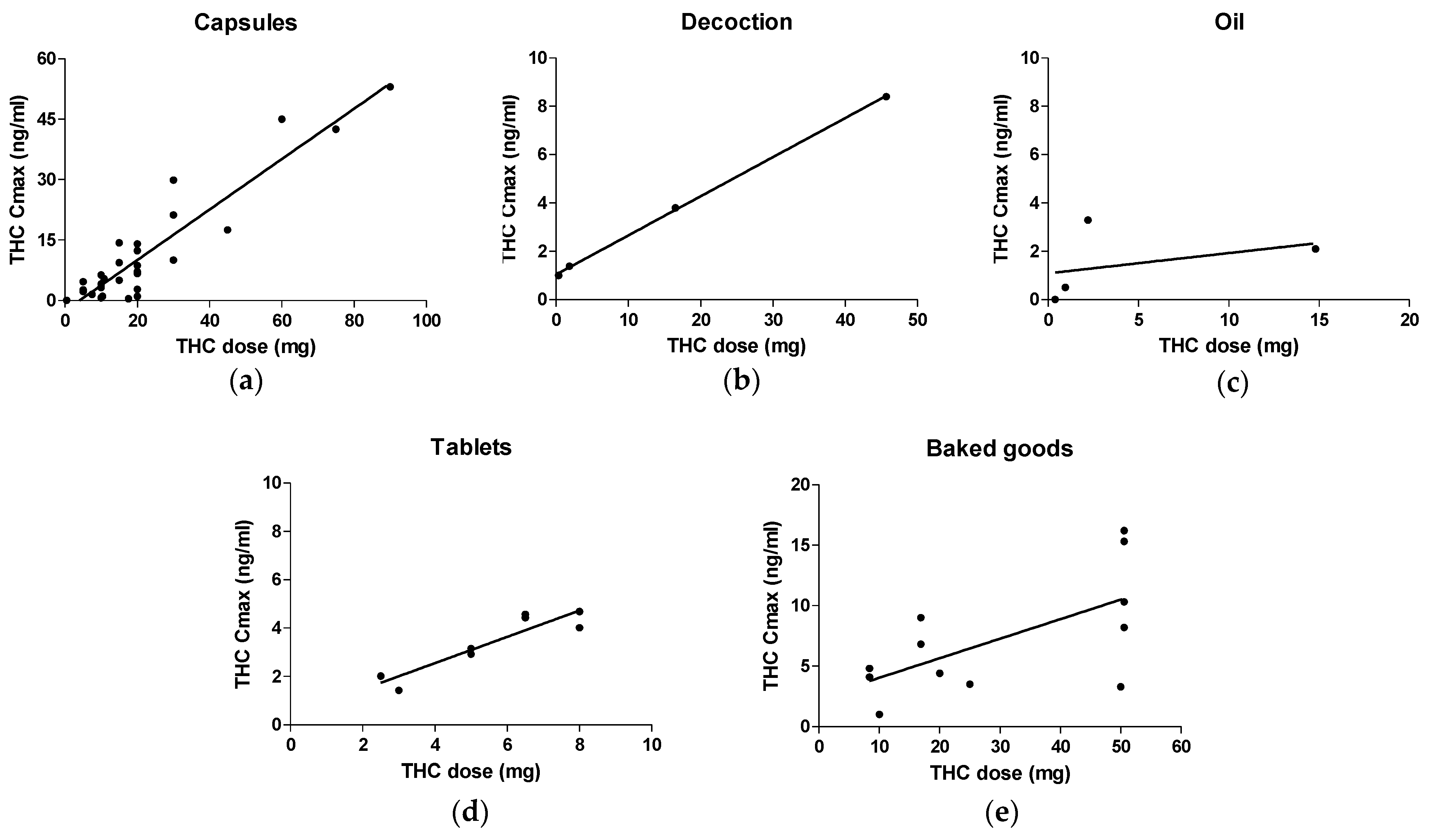
| Pearson’s r | 0.9271 | 0.9997 | 0.3806 | 0.9178 | 0.6365 |
| 95% confidence interval | 0.8492 to 0.9656 | 0.9851 to 1.000 | −0.9154 to 0.9824 | 0.6032 to 0.9853 | 0.09838 to 0.8866 |
| p value (two-tailed) | <0.0001 | 0,0003 | 0.6194 | 0.0013 | 0.0261 |
| R2 | 0.8596 | 0.9994 | 0.1448 | 0.8423 | 0.4051 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poyatos, L.; Pérez-Acevedo, A.P.; Papaseit, E.; Pérez-Mañá, C.; Martin, S.; Hladun, O.; Siles, A.; Torrens, M.; Busardo, F.P.; Farré, M. Oral Administration of Cannabis and Δ-9-tetrahydrocannabinol (THC) Preparations: A Systematic Review. Medicina 2020, 56, 309. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060309
Poyatos L, Pérez-Acevedo AP, Papaseit E, Pérez-Mañá C, Martin S, Hladun O, Siles A, Torrens M, Busardo FP, Farré M. Oral Administration of Cannabis and Δ-9-tetrahydrocannabinol (THC) Preparations: A Systematic Review. Medicina. 2020; 56(6):309. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060309
Chicago/Turabian StylePoyatos, Lourdes, Ana Pilar Pérez-Acevedo, Esther Papaseit, Clara Pérez-Mañá, Soraya Martin, Olga Hladun, Adrià Siles, Marta Torrens, Francesco Paolo Busardo, and Magí Farré. 2020. "Oral Administration of Cannabis and Δ-9-tetrahydrocannabinol (THC) Preparations: A Systematic Review" Medicina 56, no. 6: 309. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56060309