Hip Fracture Prevention in Osteoporotic Elderly and Cancer Patients: An On-Line French Survey Evaluating Current Needs



Abstract
:1. Introduction
2. Materials and Methods
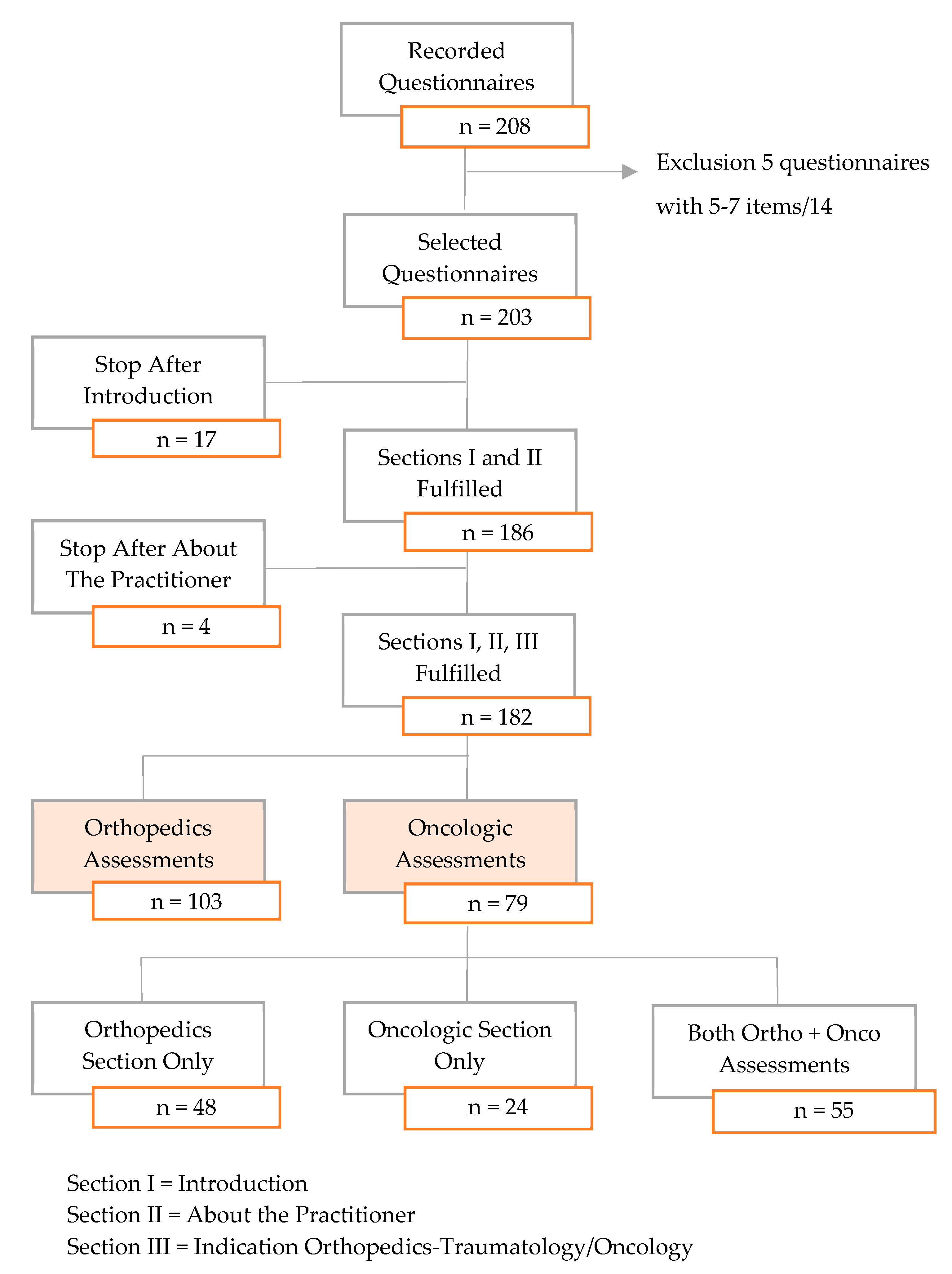
2.1. Study Design and Selection
2.2. Questionnaire
2.3. Data Collection
2.4. Statistical Analysis
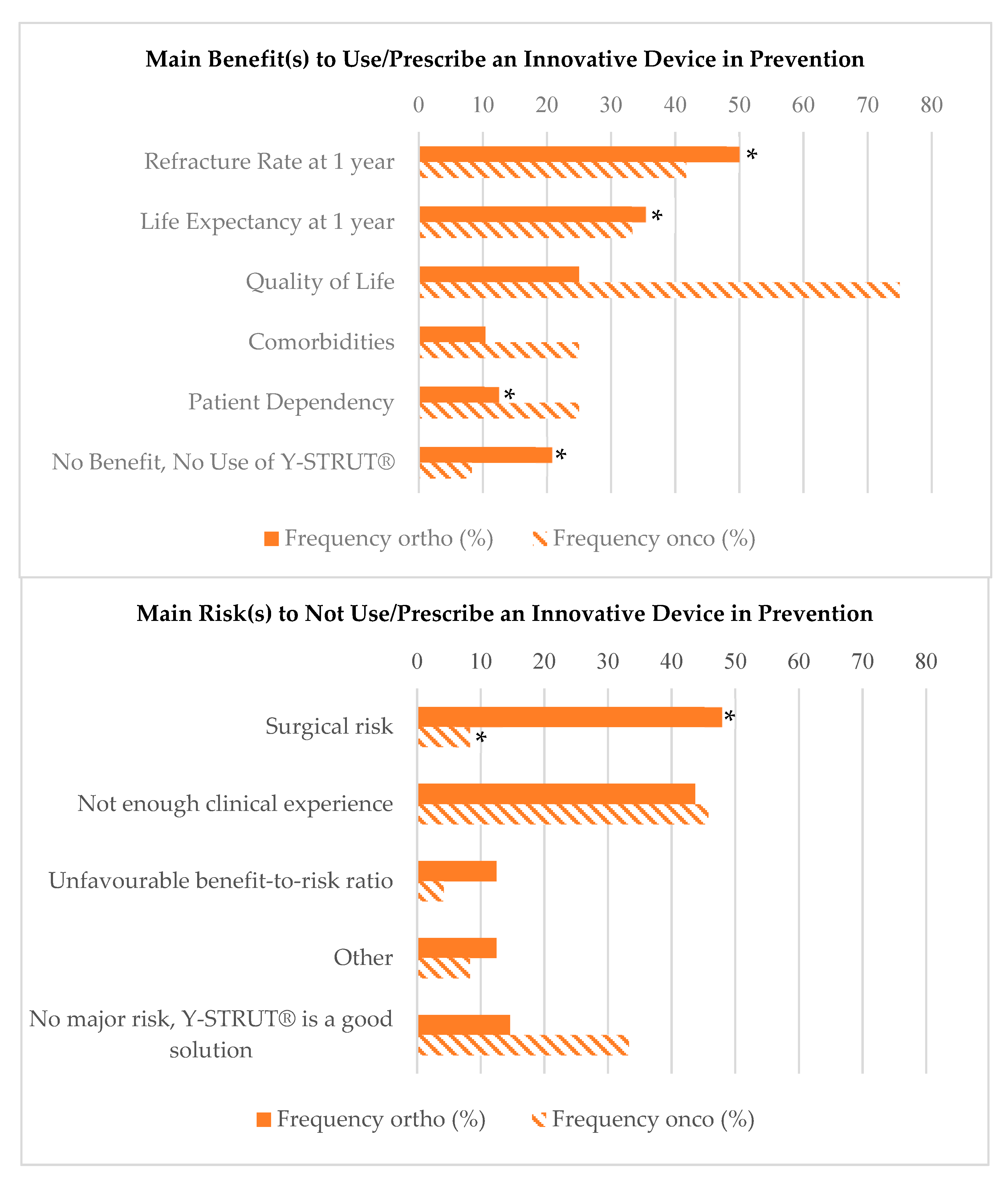
3. Results
3.1. Orthopedics Assessments
3.2. Oncology Assessments
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Interest for the Device | Orthopaedics Only (n = 48) | Oncology Only (n = 24) | Both (n = 55) | p-Value |
|---|---|---|---|---|
| Male | 47 (97.9%) | 21 (87.5%) | 53 (96.4%) | 0.16 |
| Age, Years | 0.22 | |||
| <35 | 1 (2.1%) | 3 (12.5%) | 3 (5.5%) | |
| 35–45 | 11 (22.9%) | 7 (29.2%) | 8 (23.6%) | |
| 45–55 | 13 (27.1%) | 7 (29.2%) | 31 (56.4%) | |
| >55 | 23 (47.9%) | 7 (29.2%) | 31 (56.4%) | |
| Professional Experience, Years | ||||
| <10 | 5 (10.4%) | 7 (29.2%) | 6 (10.9%) | 0.10 |
| 10–20 | 13 (27.1%) | 6 (25.0%) | 7 (12.7%) | |
| 20–30 | 20 (41.7%) | 6 (25.0%) | 23 (41.8%) | |
| >30 | 10 (20.8%) | 5 (20.8%) | 19 (34.5%) | |
| Workplace in Hospital (CHU, CHRU, CH) * | 15 (31.2%) | 12 (50.0%) | 27 (49.1%) | 0.14 |
| Orthopaedic Surgeon | 45 (93.8%) | 9 (37.5%) | 45 (81.8%) | <0.0001 |
| Previous Information on Y-STRUT® | 0.003 | |||
| Already Used or Prescribed | 0 | 5 (20.8%) | 1 (1.8%) | |
| Known, but Non-Used/Prescribed | 7 (14.6%) | 6 (25.0%) | 10 (18.2%) | |
| Never Heard About | 41 (85.4%) | 13 (54.2%) | 44 (80%) |
| Interest for the Device | Orthopaedics Only (n = 48) | Both (n = 55) | p-Value |
|---|---|---|---|
| Usage of the Device | 0.93 | ||
| User | 24 (50.0%) | 27 (49.1%) | |
| Prescriber | 5 (10.4%) | 7 (12.7%) | |
| Both | 19 (39.6%) | 21 (38.2%) | |
| Number of Patients with a Hip Fracture due to Osteoporosis, per Month | 0.05 | ||
| <5 | 24 (50.0%) | 18 (32.7%) | |
| 5–12 | 14 (29.2%) | 19 (34.55%) | |
| >12 | 10 (20.8%) | 18 (32.8%) | |
| Fracture Type | 0.66 | ||
| Mostly per Trochanteric Fractures | 12 (25.6%) | 11 (20.4) | |
| Mostly Femoral Neck Fractures | 6 (12.8%) | 10 (18.5%) | |
| Both Equally | 29 (61.7%) | 33 (61.1%) | |
| Fracture Cause | 0.66 | ||
| Mostly a Simple Fall from a Height | 32 (71.0%) | 38 (69.1%) | |
| Mostly a Fall from Bed | 0 (0%) | 1 (1.8%) | |
| A Little Bit of Everything | 13 (29.0%) | 16 (29.1%) | |
| Patients’ Sex | 0.85 | ||
| Mainly Women | 44 (91.7%) | 52 (94.5%) | |
| Patients’ Age, Years | 0.74 | ||
| 65–75 | 2 (4.2%) | 1 (1.8%) | |
| 75–85 | 31 (64.6%) | 38 (69.1%) | |
| >85 | 15 (31.2%) | 16 (29.1%) | |
| Osteoporosis Diagnosed Before Fracture | 0.27 | ||
| Mostly YES | 4 (10.8%) | 11 (22.9%) | |
| Mostly NO | 28 (75.7%) | 29 (60.4%) | |
| Both Similarly | 5 (13.5%) | 8 (16.7%) | |
| Fracture Fixation Material | 0.53 | ||
| Nail | 23 (48.9%) | 26 (47.3%) | |
| Screw and Plate | 9 (19.1%) | 9 (16.4%) | |
| Both | 6 (12.8%) | 10 (18.2%) | |
| Other | 5 (10.6%) | 2 (3.6%) | |
| No Surgery | 4 (8.5%) | 8 (14.5%) | |
| Main Criteria of Choice for Hip Fracture Treatment | |||
| Fracture Type | 38 (79.2%) | 43 (78.2%) | 1.00 |
| Pain | 1 (2.1%) | 0 (0%) | 0.95 |
| Stability, Rehabilitation | 19 (39.6%) | 25 (45.4%) | 0.69 |
| Easy-to-Use | 22 (45.8%) | 22 (40%) | 0.69 |
| Material Availability | 8 (16.7%) | 17 (30.9%) | 0.15 |
| Cost | 3 (6.25%) | 4 (7.3%) | 1.00 |
| Anaesthesia Choice for Hip Fracture Treatment | 0.17 | ||
| Mostly general | 16 (34.8%) | 26 (54.2%) | |
| Mostly spinal | 17 (37.0%) | 13 (27.1%) | |
| Both similarly | 13 (28.2%) | 9 (18.7%) | |
| Mean Surgical Time for Hip Fracture Treatment | 0.26 | ||
| <30 min | 18 (39.1%) | 23 (48.9%) | |
| 30–60+ min | 28 (60.9%) | 24 (51.1%) | |
| Strategy of Prevention | 0.08 | ||
| Simultaneously with First Fracture Treatment | 16 (42.1%) | 19 (51.4%) | |
| Postponed | 13 (34.2%) | 16 (43.2%) | |
| No Prevention | 9 (23.7%) | 2 (5.4%) | |
| Willing to Use/Prescribe Y-STRUT® in Prevention | 0.0008 | ||
| YES | 17 (63.0%) | 38 (97.4%) | |
| NO | 10 (37.0%) | 1 (2.6%) | |
| Questionnaire Satisfaction, median [Q1;Q3] | 75 [60; 80.5] | 76 [63.25; 89.75] | 0.18 |
| 100: very satisfied, 0: not satisfied at all | (n = 47) | (n = 54) | |
| Interest for the Device | Oncology Only (n = 24) | Both (n = 55) | p-Value |
|---|---|---|---|
| Usage of the Device | 0.24 | ||
| User | 10 (41.7%) | 29 (53.7%) | |
| Prescriber | 2 (8.3%) | 9 (16.7%) | |
| Both | 12 (50.0%) | 16 (29.6%) | |
| Number of Patients with Metastatic Pre-Fractural Lesions at the Proximal Hip, per Month | 1.00 | ||
| <5 | 23 (95.8%) | 50 (92.6%) | |
| 5–12 | 1 (4.2%) | 4 (7.4%) | |
| Medical Treatment for Osteolytic Metastasis at the Proximal Femur | 0.75 | ||
| YES | 15 (75.0%) | 26 (78.8%) | |
| NO | 5 (25.0%) | 7 (21.2%) | |
| Main Medical Treatment Prescribed | 0.17 | ||
| Chemotherapy | 1 (7.1%) | 4 (15.4%) | |
| Local Radiotherapy | 1 (7.1%) | 8 (30.8%) | |
| Chemotherapy + Local Radiotherapy | 12 (85.7%) | 13 (50.0%) | |
| Other | 0 (0%) | 1 (3.8%) | |
| Main type of Primary Cancer Associated to Osteolytic Metastasis at the Proximal Femur* | |||
| Lung | 18 (75.0%) | 28 (50.9%) | 0.052 |
| Breast | 17 (70.8%) | 42 (76.4%) | 0.59 |
| Prostate | 10 (41.7%) | 24 (43.6%) | 1.00 |
| Kidney | 11 (45.8%) | 18 (32.7%) | 0.31 |
| Melanoma | 3 (12.5%) | 1 (1.8%) | 0.081 |
| Other | 1 (4.2%) | 2 (3.6%) | 1.00 |
| Preventive Treatment for Proximal Femur Fracture Proposed to Patients | 0.74 | ||
| Mainly NO | 9 (39.1%) | 20 (37.0%) | |
| Mainly YES | 14 (60.9%) | 34 (63%) | |
| Main Preventive Treatment Proposed for Proximal Femur Fracture | 0.70 | ||
| Osteosynthesis in Orthopaedics Theatre | 11 (47.8%) | 35 (63.6%) | |
| Screwing + Cementoplasty | 4 (17.4%) | 7 (12.7%) | |
| Cementoplasty Alone | 1 (4.35%) | 2 (3.6%) | |
| No Prevention | 6 (26.1%) | 9 (16.4%) | |
| Other | 1 (4.35%) | 2 (3.6%) | |
| Main Criteria of Choice for Preventive Treatment* | |||
| Size of the Lesion | 17 (70.8%) | 41 (74.5%) | 0.78 |
| Pain | 11 (45.8%) | 26 (47.3%) | 1.00 |
| Easy-to-Use | 7 (29.2%) | 17 (30.9%) | 1.00 |
| Material Availability | 3 (12.5%) | 8 (14.5%) | 1.00 |
| Cost | 2 (8.3%) | 4 (7.3%) | 1.00 |
| Anaesthesia Choice for Preventive Treatment | 0.59 | ||
| Mostly General | 13 (72.2%) | 31 (64.6%) | |
| Mostly Spinal | 4 (22.2%) | 11 (22.9%) | |
| Both Similarly | 1 (5.6%) | 5 (10.4%) | |
| Other | 0 (0%) | 1 (2.0%) | |
| Mean Surgical Time for Hip Fracture Treatment, min | 0.66 | ||
| <30 | 5 (29.4%) | 10 (22.2%) | |
| 30–60 | 9 (52.9%) | 29 (64.4%) | |
| >60 | 3 (17.7%) | 6 (13.3%) | |
| Willing to Use/Prescribe Y-STRUT® in Prevention | 1.00 | ||
| YES | 15 (93.7%) | 40 (93.0%) | |
| NO | 1 (6.3%) | 3 (7.0%) | |
| Questionnaire Satisfaction, median [Q1;Q3] | 72.5 [66.25;88.5] | 72 [54.25;90] | 0.77 |
| 100: very satisfied, 0: not satisfied at all | (n = 24) | (n = 54) |
References
- Kaneko, T.S.; Skinner, H.B.; Keyak, J.H. Lytic lesions in the femoral neck: Importance of location and evaluation of a novel minimally invasive repair technique. J. Orthop. Res. 2008, 26, 1127–1132. [Google Scholar] [CrossRef]
- Ashford, R.U.; Hanna, S.A.; Park, D.H.; Pollock, R.C.; Skinner, J.A.; Briggs, T.W.R.; Cannon, S.R. Proximal femoral replacements for metastatic bone disease: Financial implications for sarcoma units. Int. Orthop. 2010, 34, 709–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundy, G.R. Metastasis to bone: Causes, consequences and therapeutic opportunities. Nat. Rev. Cancer 2002, 2, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Odén, A.; McCloskey, E.V.; Johansson, H.; Wahl, D.A.; Cooper, C. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos. Int. 2012, 23, 2239–2256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, W.W.; Egol, K.A.; Zuckerman, J.D.; Siu, A.L. Hip Fracture Management Tailoring Care for the Older Patient. JAMA 2012, 307, 2185–2194. [Google Scholar] [CrossRef]
- Veronese, N.; Maggi, S. Epidemiology and social costs of hip fracture. Injury 2018, 49, 1458–1460. [Google Scholar] [CrossRef]
- Ekman, E.F. The role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. J. Am. Acad. Orthop. Surg. 2010, 18, 278–285. [Google Scholar] [CrossRef]
- Mazzucchelli, R.; Pérez-Fernández, E.; Crespí, N.; García-Vadillo, A.; Rodriguez Caravaca, G.; Gil de Miguel, A.; Carmona, L. Second Hip Fracture: Incidence, Trends, and Predictors. Calcif. Tissue Int. 2018, 102, 619–626. [Google Scholar] [CrossRef]
- Dreinhöfer, K.E.; Mitchell, P.J.; Bégué, T.; Cooper, C.; Costa, M.L.; Falaschi, P.; Hertz, K.; Marsh, D.; Maggi, S.; Nana, A.; et al. A global call to action to improve the care of people with fragility fractures. Injury 2018, 49, 1393–1397. [Google Scholar] [CrossRef]
- González-Montalvo, J.I.; Mauleón, J.L.; Gil-Garay, E.; Gotor, P.; Martín-Vega, A. The orthogeriatric unit for acute patients: A new model of care that improves efficiency in the management of patients with hip fracture. HIP Int. 2010, 20, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Bawa, H.S.; Weick, J.; Dirschl, D.R. Anti-Osteoporotic Therapy After Fragility Fracture Lowers Rate of Subsequent Fracture: Analysis of a Large Population Sample. J. Bone Joint Surg. Am. 2015, 97, 1555–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liel, Y.; Castel, H.; Bonneh, D.Y. Impact of subsidizing effective anti-osteoporosis drugs on compliance with management guidelines in patients following low-impact fractures. Osteoporos. Int. 2003, 14, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Rabenda, V.; Mertens, R.; Fabri, V.; Vanoverloop, J.; Sumkay, F.; Vannecke, C.; Deswaef, A.; Verpooten, G.A.; Reginster, J.Y. Adherence to bisphosphonates therapy and hip fracture risk in osteoporotic women. Osteoporos. Int. 2008, 19, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Inderjeeth, C.A.; Chan, K.; Kwan, K.; Lai, M. Time to onset of efficacy in fracture reduction with current anti-osteoporosis treatments. J. Bone Miner. Metab. 2012, 30, 493–503. [Google Scholar] [CrossRef]
- Mugnier, B.; Daumas, A.; Couderc, A.; Mizzi, B.; González, T.; Amrani, A.; Lévêque, P.; Aymes, B.; Villani, P. Clinical effectiveness of osteoporosis treatment in older patients: A fracture liaison service-based prospective study. J. Women Aging 2018, 31, 553–565. [Google Scholar] [CrossRef]
- Schneiderbauer, M.M.; Von Knoch, M.; Schleck, C.D.; Harmsen, W.S.; Sim, F.H.; Scully, S.P. Patient Survival after Hip Arthroplasty for Metastatic Disease of the Hip. J. Bone Joint Surg Am 2004, 86, 1684–1689. [Google Scholar] [CrossRef]
- Parker, M.J.; Khan, A.Z.; Rowlands, T.K. Survival after pathological fractures of the proximal femur. HIP Int. 2011, 21, 526–530. [Google Scholar] [CrossRef]
- Hage, W.D.; Aboulafia, A.J.; Aboulafia, D.M. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop. Clin. N. Am. 2000, 31, 515–528. [Google Scholar] [CrossRef]
- Stresing, V.; Daubiné, F.; Benzaid, I.; Mönkkönen, H.; Clézardin, P. Bisphosphonates in cancer therapy. Cancer Lett. 2007, 257, 16–35. [Google Scholar] [CrossRef]
- Coleman, R.E.; McCloskey, E.V. Bisphosphonates in oncology. Bone 2011, 49, 71–76. [Google Scholar] [CrossRef]
- Ristevski, B.; Jenkinson, R.J.; Stephen, D.J.G.; Finkelstein, J.; Schemitsch, E.H.; McKee, M.D.; Kreder, H.J. Mortality and complications following stabilization of femoral metastatic lesions: A population-based study of regional variation and outcome. Can. J. Surg. 2008, 52, 302–308. [Google Scholar]
- Deschamps, F.; Farouil, G.; Hakime, A.; Barah, A.; Guiu, B.; Teriitehau, C.; Auperin, A.; deBaere, T. Cementoplasty of metastases of the proximal femur: Is it a safe palliative option? J. Vasc. Interv. Radiol. 2012, 23, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.-H.; He, C.-J.; Wu, C.-G.; Li, Y.-D.; Gu, Y.-F.; Wang, T.; Xiao, Q.-P.; Li, M.-H. Comparison of Percutaneous Cementoplasty with and Without Interventional Internal Fixation for Impending Malignant Pathological Fracture of the Proximal Femur. Cardiovasc. Interv. Radiol. 2015, 39, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Arvinius, C.; Parra, J.L.C.; Mateo, L.S.; Maroto, R.G.; Borrego, A.F.; Stern, L.L.-D. Benefits of early intramedullary nailing in femoral metastases. Int. Orthop. 2014, 38, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelekis, A.; Filippiadis, D.; Anselmetti, G.; Brountzos, E.; Mavrogenis, A.; Papagelopoulos, P.; Kelekis, N.; Martin, J.-B. Percutaneous Augmented Peripheral Osteoplasty in Long Bones of Oncologic Patients for Pain Reduction and Prevention of Impeding Pathologic Fracture: The Rebar Concept. Cardiovasc. Interv. Radiol. 2016, 39, 90–96. [Google Scholar] [CrossRef]
- Jawad, M.U.; Scully, S.P. In brief: Classifications in brief: Mirels’ classification: Metastatic disease in long bones and impending pathologic fracture. Clin. Orthop. Relat. Res. 2010, 468, 2825–2827. [Google Scholar] [CrossRef] [Green Version]
- Giannini, S.; Luciani, D.; Chiarello, E.; Cadossi, M.; Tedesco, G.; Hoque, M.; Gnudi, S. Osteosynthetic improvement of osteoporotic bone: Prevention surgery. Clin. Cases Miner. Bone Metab. 2011, 8, 51–54. [Google Scholar]
- Varga, P.; Hofmann-Fliri, L.; Blauth, M.; Windolf, M. Prophylactic augmentation of the osteoporotic proximal femur—Mission impossible? Bonekey Rep. 2016, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, S.; Reginster, J.-Y.; Brandi, M.L.; Kanis, J.A.; Devogelaer, J.-P.; Kaufman, J.-M.; Féron, J.-M.; Kurth, A.; Rizzoli, R. Unmet needs and current and future approaches for osteoporotic patients at high risk of hip fracture. Arch. Osteoporos. 2016, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, L.; Cornelis, F.H.; Reina, N.; Chevret, S. Prevention of Pathological Fracture of the Proximal Femur: A Systematic Review of Surgical and Percutaneous Image-Guided Techniques Used in Interventional Oncology. Medicina 2019, 55, 755. [Google Scholar] [CrossRef] [Green Version]
- Cornelis, F.H.; Tselikas, L.; Carteret, T.; Lapuyade, B.; De Baere, T.; Cabane, V.; Rodrigues, L.; Maas, C.; Deschamps, F. A Novel Implant for the Prophylactic Treatment of Impending Pathological Fractures of the Proximal Femur: Results from a Prospective, First-in-Man Study. Cardiovasc. Interv. Radiol. 2017, 40, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, F.H.; Tselikas, L.; Carteret, T.; Lapuyade, B.; De Baere, T.; Le Huec, J.C.; Deschamps, F. Percutaneous internal fixation with Y-STRUT® device to prevent both osteoporotic and pathological hip fractures: A prospective pilot study. J. Orthop. Surg. Res. 2017, 12, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szpalski, M.; Le Huec, J.C.; Jayankura, M.; Reynders, P.; Maas, C. Contralateral Prophylactic Reinforcement in Case of First Low-Energy Hip Fracture: First-in-Man Clinical Data of a New Percutaneous Internal Fixation Device. J. Osteoporos. Phys. Act. 2017, 5. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.C.S.; Conde, J.G. Research Electronic Data Capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Newcombe, R.G. Two-sided confidence intervals for the single proportion: Comparison of seven methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Grigoryan, K.V.; Javedan, H.; Rudolph, J.L. Orthogeriatric care models and outcomes in hip fracture patients: A systematic review and meta-analysis. J. Orthop. Trauma 2014, 28, e49–e55. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.; Åkesson, K.; Chandran, M.; Cooper, C.; Ganda, K.; Schneider, M. Best Practice & Research Clinical Rheumatology Implementation of Models of Care for secondary osteoporotic fracture prevention and orthogeriatric Models of Care for osteoporotic hip fracture. Best Pract. Res. Clin. Rheumatol. 2016, 30, 536–558. [Google Scholar]
- Ryg, J.; Rejnmark, L.; Overgaard, S.; Brixen, K.; Vestergaard, P. Hip fracture patients at risk of second hip fracture: A nationwide population-based cohort study of 169,145 cases during 1977–2001. J. Bone Miner. Res. 2009, 24, 1299–1307. [Google Scholar] [CrossRef]
- Mak, J.C.S.; Cameron, I.D.; March, L.M. Evidence-based guidelines for the management of hip fractures in older persons: An update. MJA 2010, 192, 37–41. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, L.; Cornelis, F.H.; Chevret, S. Hip Fracture Prevention in Osteoporotic Elderly and Cancer Patients: An On-Line French Survey Evaluating Current Needs. Medicina 2020, 56, 397. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56080397
Rodrigues L, Cornelis FH, Chevret S. Hip Fracture Prevention in Osteoporotic Elderly and Cancer Patients: An On-Line French Survey Evaluating Current Needs. Medicina. 2020; 56(8):397. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56080397
Chicago/Turabian StyleRodrigues, Laëtitia, François H. Cornelis, and Sylvie Chevret. 2020. "Hip Fracture Prevention in Osteoporotic Elderly and Cancer Patients: An On-Line French Survey Evaluating Current Needs" Medicina 56, no. 8: 397. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56080397