Health-Related Quality of Life and Related Factors in Persons with Preserved Ratio Impaired Spirometry: Data from the Korea National Health and Nutrition Examination Surve


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Participants
2.2. Variables
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
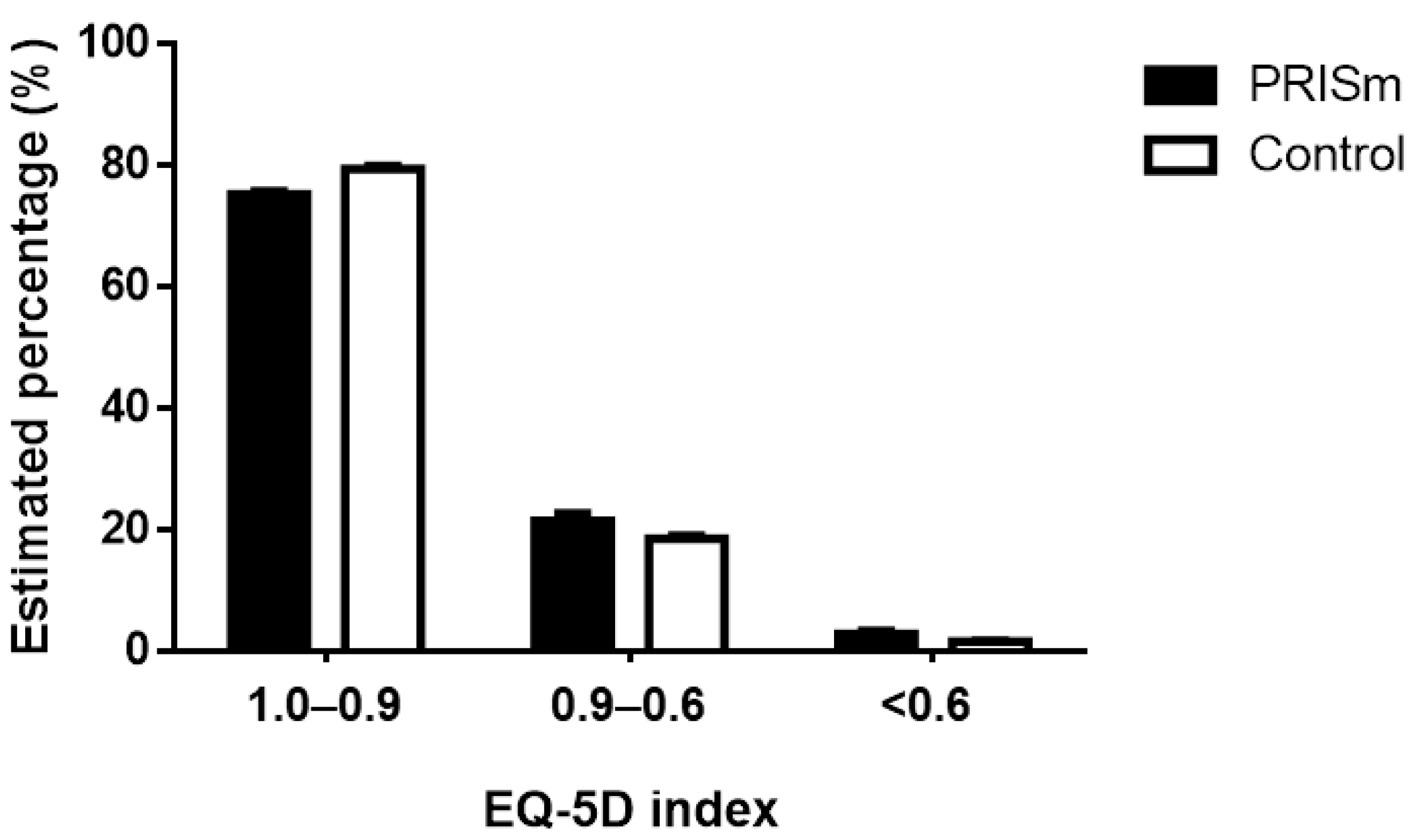
3.2. Comparing HRQOL between the PRISm and Normal Lung Function Groups
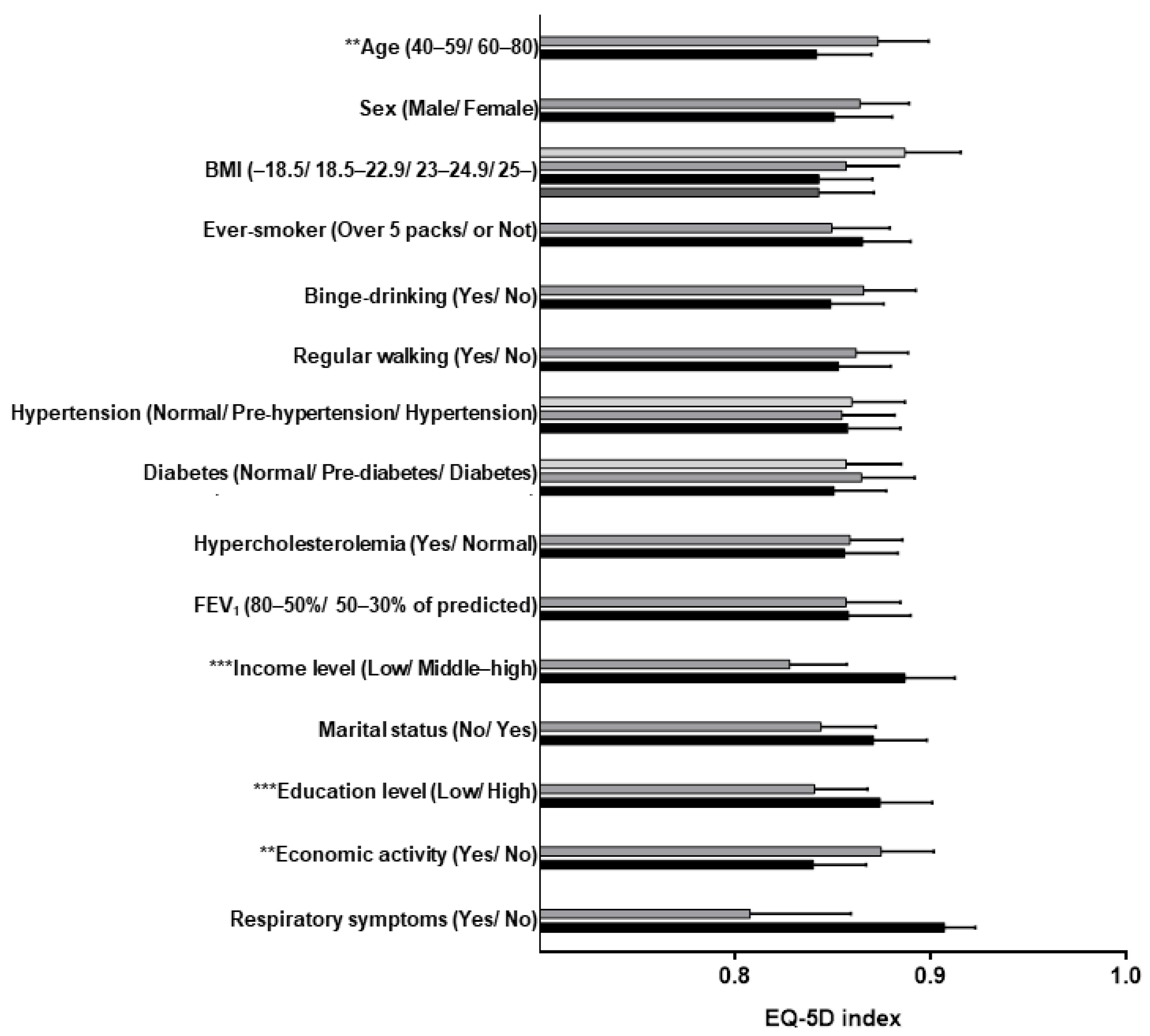
3.3. Factors Associated with HRQOL in PRISm
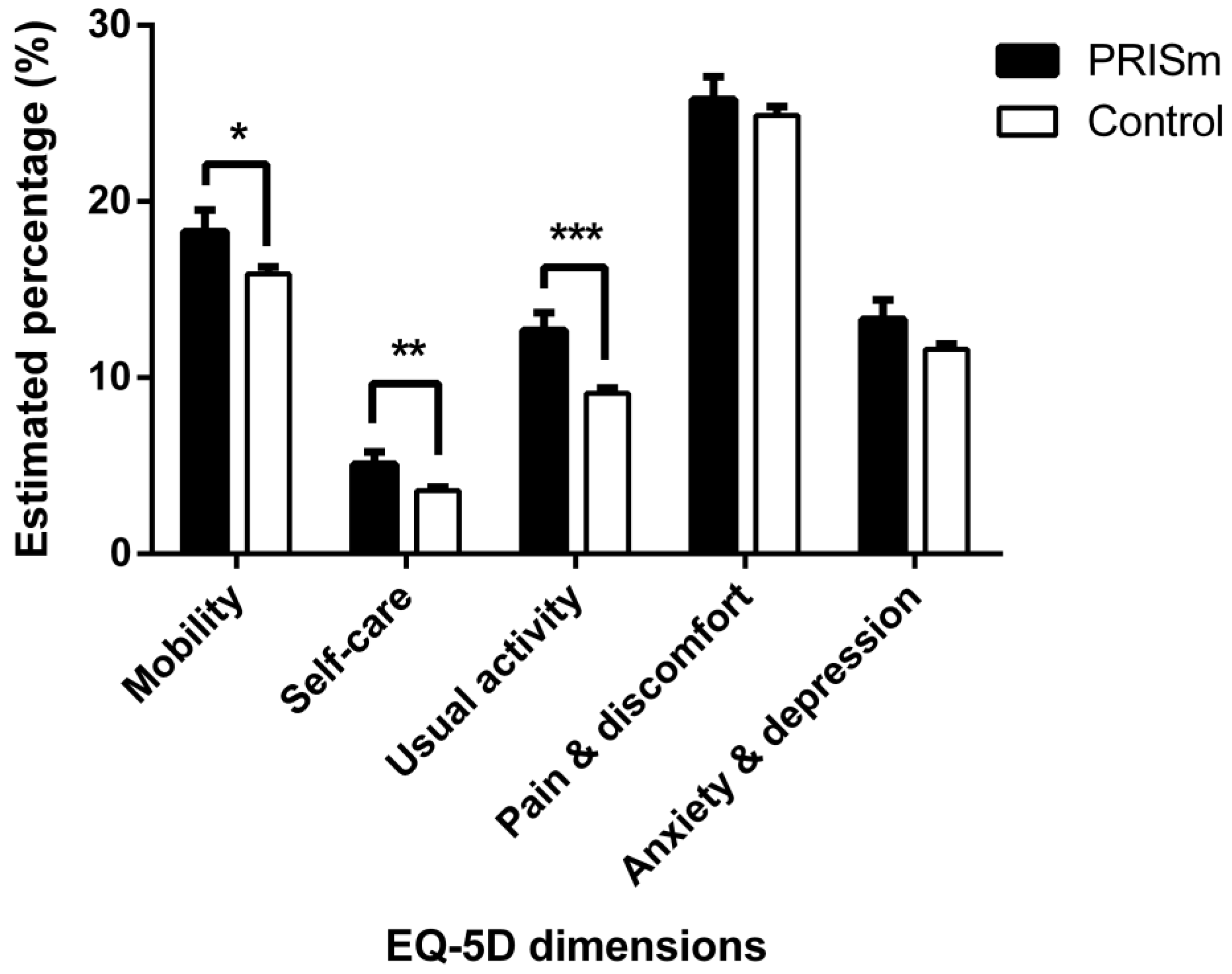
3.4. HRQOL According to Each Dimension of EQ-5D
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed]
- Iyer, V.N.; Schroeder, D.R.; Parker, K.O.; Hyatt, R.E.; Scanlon, P.D. The nonspecific pulmonary function test: Longitudinal follow-up and outcomes. Chest 2011, 139, 878–886. [Google Scholar] [CrossRef] [PubMed]
- Make, B.J. COPD: A New Diagnostic Paradigm. Chronic Obstr. Pulm. Dis. 2019, 6, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Adibi, A.; Sadatsafavi, M. Looking at the COPD spectrum through “PRISm”. Eur. Respir. J. 2020, 55, 1902217. [Google Scholar] [CrossRef] [PubMed]
- Wan, E.S.; Castaldi, P.J.; Cho, M.H.; Hokanson, J.E.; Regan, E.A.; Make, B.J.; Beaty, T.H.; Han, M.K.; Curtis, J.L.; Curran-Everett, D.; et al. Epidemiology, genetics, and subtyping of preserved ratio impaired spirometry (PRISm) in COPDGene. Respir. Res. 2014, 15, 89. [Google Scholar] [CrossRef] [Green Version]
- Wijnant, S.R.A.; De Roos, E.; Kavousi, M.; Stricker, B.H.; Terzikhan, N.; Lahousse, L.; Brusselle, G.G. Trajectory and mortality of preserved ratio impaired spirometry: The Rotterdam Study. Eur. Respir. J. 2020, 55, 1901217. [Google Scholar] [CrossRef]
- Nishimura, K.; Izumi, T.; Tsukino, M.; Oga, T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest 2002, 121, 1434–1440. [Google Scholar] [CrossRef] [Green Version]
- Medinas Amorós, M.; Mas-Tous, C.; Renom-Sotorra, F.; Rubí-Ponseti, M.; Centeno-Flores, M.J.; Gorriz-Dolz, M.T. Health-related quality of life is associated with COPD severity: A comparison between the GOLD staging and the BODE index. Chron. Respir. Dis. 2009, 6, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef]
- Meguro, M.; Barley, E.A.; Spencer, S.; Jones, P.W. Development and Validation of an Improved, COPD-Specific Version of the St. George Respiratory Questionnaire. Chest 2007, 132, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celli, B.R.; MacNee, W. Standards for the diagnosis and treatment of patients with COPD: A summary of the ATS/ERS position paper. Eur. Respir. J. 2004, 23, 932–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.K.; Nam, H.S.; Chuang, L.H.; Kim, K.Y.; Yang, H.K.; Kwon, I.S.; Kind, P.; Kweon, S.S.; Kim, Y.T. South Korean time trade-off values for EQ-5D health states: Modeling with observed values for 101 health states. Value Health 2009, 12, 1187–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.U.; Lee, J.H.; Kim, J.S.; Hwang, Y.I.; Kim, T.H.; Lim, S.Y.; Yoo, K.H.; Jung, K.S.; Kim, Y.K.; Rhee, C.K. Comparison of World Health Organization and Asia-Pacific body mass index classifications in COPD patients. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 2465–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannino, D.M.; McBurnie, M.A.; Tan, W.; Kocabas, A.; Anto, J.; Vollmer, W.M.; Buist, A.S. Restricted spirometry in the Burden of Lung Disease Study. Int. J. Tuberc. Lung Dis. 2012, 16, 1405–1411. [Google Scholar] [CrossRef]
- Backman, H.; Eriksson, B.; Hedman, L.; Stridsman, C.; Jansson, S.A.; Sovijärvi, A.; Lindberg, A.; Rönmark, E.; Lundbäck, B. Restrictive spirometric pattern in the general adult population: Methods of defining the condition and consequences on prevalence. Respir. Med. 2016, 120, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Jankowich, M.; Elston, B.; Liu, Q.; Abbasi, S.; Wu, W.C.; Blackshear, C.; Godfrey, M.; Choudhary, G. Restrictive Spirometry Pattern, Cardiac Structure and Function, and Incident Heart Failure in African Americans. TheJackson Heart Study. Ann. Am. Thorac. Soc. 2018, 15, 1186–1196. [Google Scholar] [CrossRef]
- Wan, E.S.; Hokanson, J.E.; Murphy, J.R.; Regan, E.A.; Make, B.J.; Lynch, D.A.; Crapo, J.D.; Silverman, E.K. Clinical and radiographic predictors of GOLD-unclassified smokers in the COPDGene study. Am. J. Respir. Crit. Care Med. 2011, 184, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Guerra, S.; Carsin, A.E.; Keidel, D.; Sunyer, J.; Leynaert, B.; Janson, C.; Jarvis, D.; Stolz, D.; Rothe, T.; Pons, M.; et al. Health-related quality of life and risk factors associated with spirometric restriction. Eur. Respir. J. 2017, 49, 1602096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, S.; Sherrill, D.L.; Venker, C.; Ceccato, C.M.; Halonen, M.; Martinez, F.D. Morbidity and mortality associated with the restrictive spirometric pattern: A longitudinal study. Thorax 2010, 65, 499–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, E.S.; Fortis, S.; Regan, E.A.; Hokanson, J.; Han, M.K.; Casaburi, R.; Make, B.J.; Crapo, J.D.; DeMeo, D.L.; Silverman, E.K. Longitudinal Phenotypes and Mortality in Preserved Ratio Impaired Spirometry in the COPDGene Study. Am. J. Respir. Crit. Care Med. 2018, 198, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.Y.; Kim, E. Factors contributing to quality of life in COPD patients in South Korea. Int. J. Chron. Obs. Pulmon. Dis. 2016, 11, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Won, H.K.; Lee, J.H.; An, J.; Sohn, K.H.; Kang, M.G.; Kang, S.Y.; Morice, A.H.; Cho, S.H.; Song, W.J. Impact of Chronic Cough on Health-Related Quality of Life in the Korean Adult General Population: The Korean National Health and Nutrition Examination Survey 2010. Allergy Asthma Immunol. Res. 2020, 12, 964–979. [Google Scholar] [CrossRef] [PubMed]
- Kil, S.R.; Lee, S.I.; Yun, S.C.; An, H.M.; Jo, M.W. The decline of health-related quality of life associated with some diseases in Korean adults. J. Prev. Med. Public Health 2008, 41, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Han, C.H. Health related quality of life in relation to asthma-Data from a cross sectional study. J. Asthma 2018, 55, 1011–1017. [Google Scholar] [CrossRef]
- Vatrella, A.; Calabrese, C.; Mattiello, A.; Panico, C.; Costigliola, A.; Chiodini, P.; Panico, S. Abdominal adiposity is an early marker of pulmonary function impairment: Findings from a Mediterranean Italian female cohort. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 643–648. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G.; Rumley, A.; Sattar, N.; Whincup, P.H.; Thomas, M.C.; Lowe, G.D. Lung function and risk of type 2 diabetes and fatal and nonfatal major coronary heart disease events: Possible associations with inflammation. Diabetes Care 2010, 33, 1990–1996. [Google Scholar] [CrossRef] [Green Version]
- Kalhan, R.; Tran, B.T.; Colangelo, L.A.; Rosenberg, S.R.; Liu, K.; Thyagarajan, B.; Jacobs Jr, D.R.; Smith, L.J. Systemic inflammation in young adults is associated with abnormal lung function in middle age. PLoS ONE 2010, 5, e11431. [Google Scholar] [CrossRef]
- Thyagarajan, B.; Jacobs, D.R.; Apostol, G.G.; Smith, L.J.; Lewis, C.E.; Williams, O.D. Plasma fibrinogen and lung function: The CARDIA Study. Int. J. Epidemiol. 2006, 35, 1001–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortis, S.; Comellas, A.; Kim, V.; Casaburi, R.; Hokanson, J.E.; Crapo, J.D.; Silverman, E.K.; Wan, E.S. Low FVC/TLC in Preserved Ratio Impaired Spirometry (PRISm) is associated with features of and progression to obstructive lung disease. Sci. Rep. 2020, 10, 5169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maleki-Yazdi, M.R.; Lewczuk, C.K.; Haddon, J.M.; Choudry, N.; Ryan, N. Early detection and impaire quality of life in COPD GOLD stage 0: A pilot study. COPD 2007, 4, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Bridevaux, P.O.; Gerbase, M.W.; Probst-Hensch, N.M.; Schindler, C.; Gaspoz, J.M.; Rochat, T. Long-term decline in lung function, utilisation of care and quality of life in modified GOLD stage 1 COPD. Thorax 2008, 63, 768–774. [Google Scholar] [CrossRef] [Green Version]
- Leone, N.; Courbon, D.; Thomas, F.; Bean, K.; Jégo, B.; Leynaert, B.; Guize, L.; Zureik, M. Lung function impairment and metabolic syndrome: The critical role of abdominal obesity. Am. J. Respir. Crit. Care Med. 2009, 179, 509–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, E.; Choi, S.E.; Lee, H.; Shin, G.; Kang, D. Validity of EQ-5D utility index and minimal clinically important difference estimation among patients with chronic obstructive pulmonary disease. BMC Pulm. Med. 2020, 20, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngo, C.Q.; Phan, P.T.; Vu, G.V.; Pham, Q.L.T.; Nguyen, L.H.; Vu, G.T.; Tran, T.T.; Nguyen, H.L.T.; Tran, B.X.; Latkin, C.A.; et al. Effects of Different Comorbidities on Health-Related Quality of Life among Respiratory Patients in Vietnam. J. Clin. Med. 2019, 8, 214. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| PRISm (n = 1875) | Control (n = 14,467) | p-Value | |
|---|---|---|---|
| Age (years) | 0.025 * | ||
| 40–59 | 70.3 (1.4) | 73.4 (0.6) | |
| 60 and above | 29.7 (1.4) | 26.6 (0.6) | |
| Sex | <0.001 *** | ||
| Male | 49.4 (1.6) | 43.0 (0.5) | |
| Female | 50.6 (1.6) | 57.0 (0.5) | |
| BMI | <0.001 *** | ||
| <18.5 | 2.5 (0.5) | 1.1 (0.1) | |
| 18.5–22.9 | 27.6 (1.3) | 33.8 (0.5) | |
| 23–24.9 | 27.2 (1.4) | 27.3 (0.5) | |
| >25.0 | 42.8 (1.5) | 37.8 (0.6) | |
| Smoking habit | |||
| Ever-smoker (>5 packs) | 44.8 (1.6) | 38.2 (0.5) | <0.001 *** |
| Current smoker | 34.2 (1.5) | 26.3 (0.5) | <0.001 *** |
| Binge-drinking | 18.0 (1.3) | 16.9 (0.4) | 0.429 |
| Regular walking exercise | 35.0 (1.5) | 39.1 (0.6) | 0.001 ** |
| Hypertension | <0.001 *** | ||
| Normal | 30.3 (1.4) | 36.9 (0.6) | |
| Pre-hypertension | 25.6 (1.5) | 27.5 (0.5) | |
| Hypertension | 44.1 (1.6) | 35.6 (0.6) | |
| Diabetes mellitus | <0.001 *** | ||
| Normal | 55.9 (1.6) | 65.0 (0.5) | |
| Pre-diabetes | 27.7 (1.5) | 24.4 (0.5) | |
| Diabetes mellitus | 16.3 (1.1) | 10.6 (0.3) | |
| Hypercholesterolemia | 18.2 (1.2) | 16.7 (0.4) | 0.217 |
| Lung function tests | |||
| FVC (L) | 2.92 (0.02) | 3.63 (0.01) | <0.001 *** |
| FVC (% of predicted) | 75.5 (0.3) | 96.1 (0.1) | <0.001 *** |
| FEV1 (L) | 2.25 (0.02) | 2.89 (0.01) | <0.001 *** |
| FEV1 (% of predicted) | 74.2 (0.2) | 97.1 (0.1) | <0.001 *** |
| FEV1/FVC | 0.77 (0.0) | 0.80 (0.0) | <0.001 *** |
| Socioeconomic factors | |||
| Low income | 20.3 (1.3) | 17.6 (0.5) | 0.034 * |
| No marital status | 15.3 (1.1) | 16.0 (0.4) | 0.521 |
| Low educational level | 34.6 (1.5) | 35.7 (0.7) | 0.479 |
| No economic activity | 35.6 (1.5) | 33.9 (0.6) | 0.306 |
| Univariate Analysis | Risk-Adjusted Analysis | |||
|---|---|---|---|---|
| Contrast Estimate (SE) | p Value | Contrast Estimate (SE) | p Value | |
| Age (years) | ||||
| 40–59 | - | - | - | - |
| 60 and above | −0.089 (0.010) | <0.001 *** | −0.031 (0.011) | 0.004 ** |
| Sex | ||||
| Male | - | - | - | - |
| Female | −0.039 (0.008) | <0.001 *** | −0.013 (0.014) | 0.349 |
| BMI | ||||
| <18.5 | 0.013 (0.015) | 0.378 | 0.030 (0.016) | 0.067 |
| 18.5–22.9 | - | - | - | - |
| 23–24.9 | −0.017 (0.010) | 0.095 | −0.014 (0.009) | 0.123 |
| >25.0 | −0.013 (0.009) | 0.142 | −0.014 (0.009) | 0.124 |
| Ever-smoker (>5 packs) | 0.009 (0.004) | 0.025 * | −0.016 (0.013) | 0.222 |
| Binge-drinking | 0.041 (0.008) | <0.001 *** | 0.017 (0.010) | 0.091 |
| Regular walking exercise | 0.011 (0.008) | 0.129 | 0.009 (0.006) | 0.154 |
| Hypertension | ||||
| Normal | - | - | - | - |
| Pre-hypertension | −0.016 (0.009) | 0.083 | −0.005 (0.009) | 0.571 |
| Hypertension | −0.013 (0.009) | <0.001 *** | −0.002 (0.009) | 0.821 |
| Diabetes mellitus | ||||
| Normal | - | - | - | - |
| Pre-diabetes | −0.010 (0.010) | 0.32 | 0.008 (0.009) | 0.376 |
| Diabetes mellitus | −0.030 (0.011) | 0.006 ** | −0.006 (0.013) | 0.635 |
| Hypercholesterolemia | −0.024 (0.011) | 0.031 * | 0.003 (0.012) | 0.806 |
| Lung function tests | ||||
| FEV1 50–80% of predicted | - | - | - | - |
| FEV1 30–50% of predicted | 0.004 (0.026) | 0.864 | - | - |
| Respiratory symptoms | −0.109 (0.065) | 0.096 | −0.099 (0.055) | 0.072 |
| Socioeconomic factors | ||||
| Low income | −0.102 (0.014) | <0.001 *** | −0.059 (0.015) | <0.001 *** |
| No marital status | −0.073 (0.014) | <0.001 *** | −0.027 (0.016) | 0.093 |
| Low educational level | −0.087 (0.009) | <0.001 *** | −0.034 (0.010) | <0.001 *** |
| No economic activity | −0.067 (0.009) | <0.001 *** | −0.035 (0.010) | <0.001 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, I.R.; Kim, H.C.; Kim, T.H. Health-Related Quality of Life and Related Factors in Persons with Preserved Ratio Impaired Spirometry: Data from the Korea National Health and Nutrition Examination Surve. Medicina 2021, 57, 4. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010004
Heo IR, Kim HC, Kim TH. Health-Related Quality of Life and Related Factors in Persons with Preserved Ratio Impaired Spirometry: Data from the Korea National Health and Nutrition Examination Surve. Medicina. 2021; 57(1):4. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010004
Chicago/Turabian StyleHeo, I Re, Ho Cheol Kim, and Tae Hoon Kim. 2021. "Health-Related Quality of Life and Related Factors in Persons with Preserved Ratio Impaired Spirometry: Data from the Korea National Health and Nutrition Examination Surve" Medicina 57, no. 1: 4. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010004