Increased Psychological Distress, Loneliness, and Unemployment in the Spread of COVID-19 over 6 Months in Germany


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Self-Reported Psychological Distress
2.3. Measures of Loneliness
2.4. Data Analysis
3. Results
3.1. Group Description
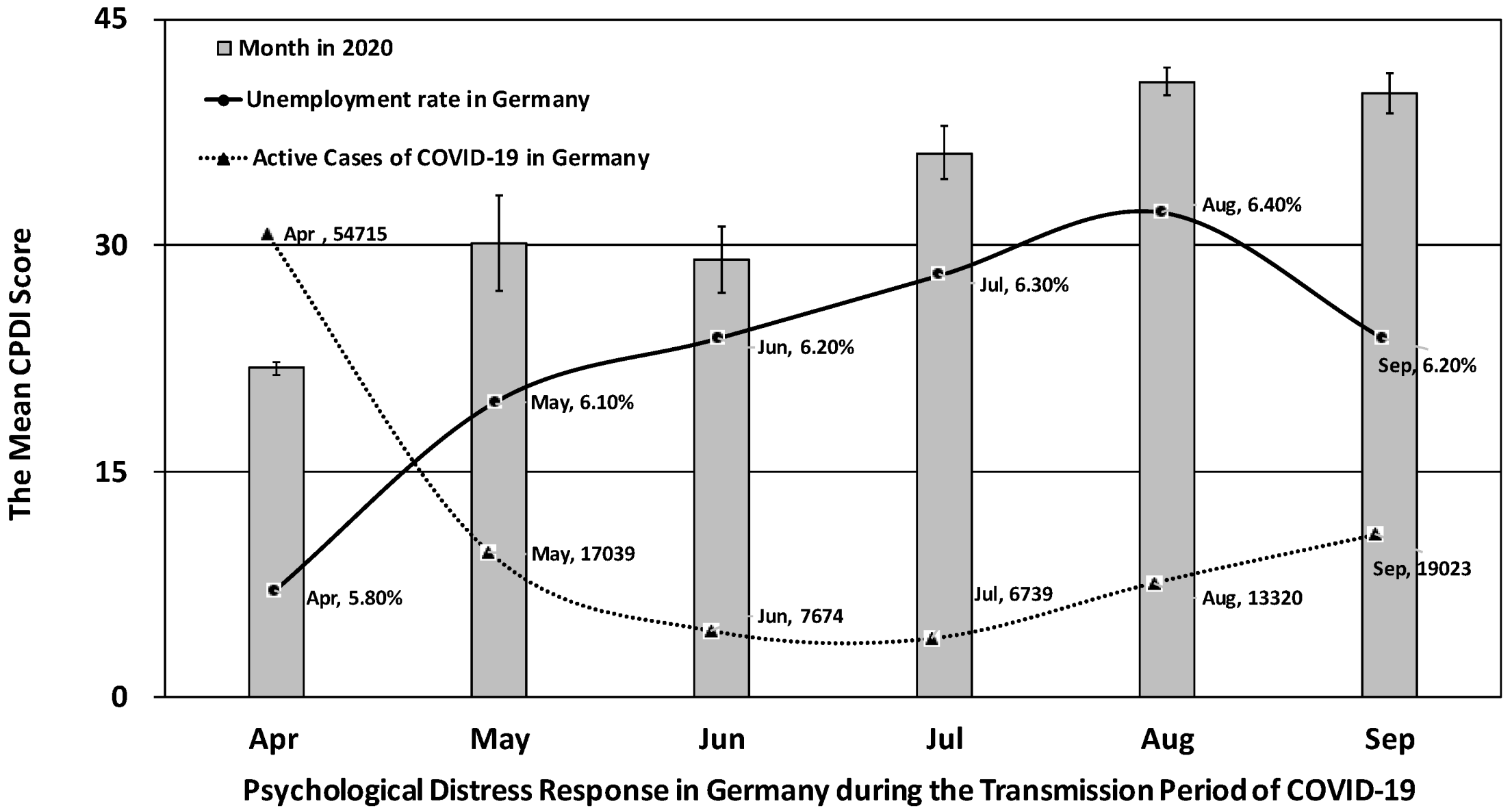
3.2. Increased Psychological Distress over the Course of the Pandemic in Germany
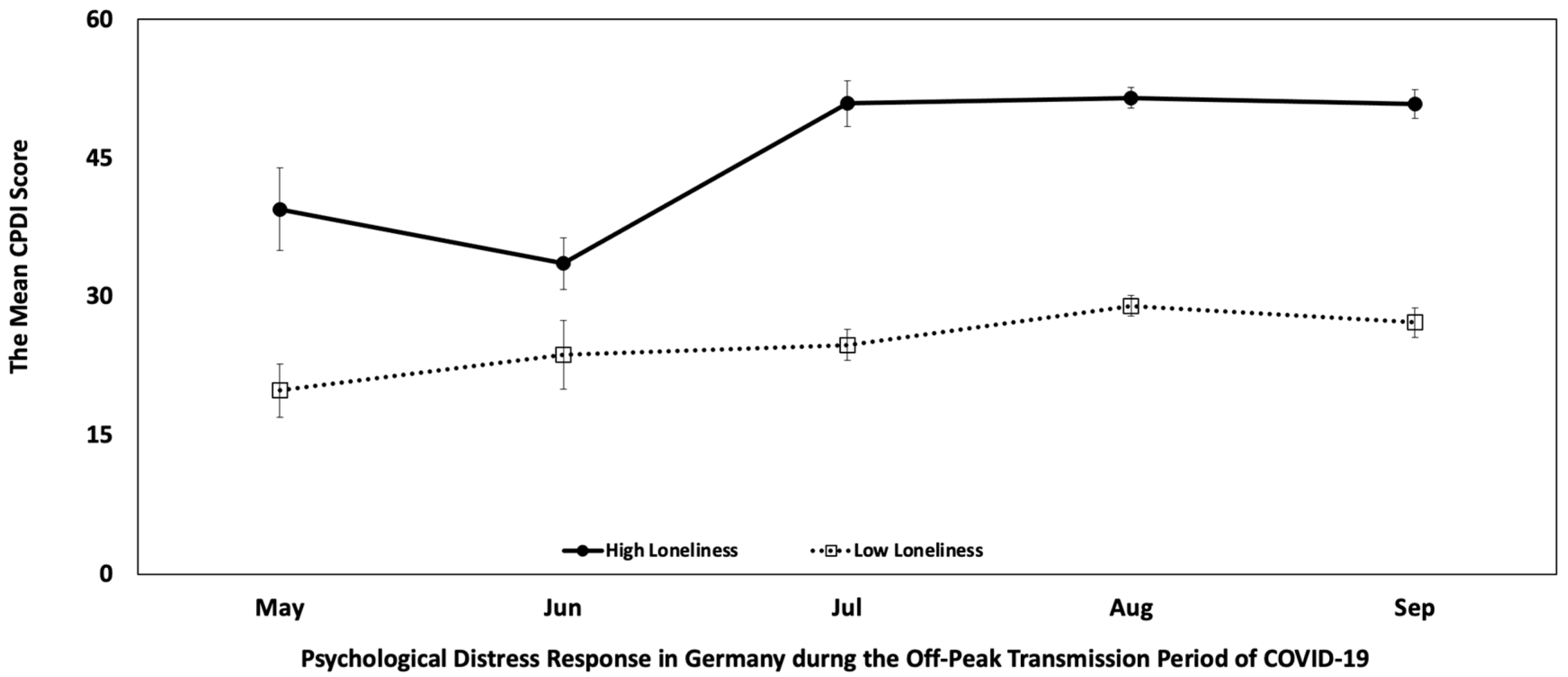
3.3. Loneliness Predicts Psychological Distress
4. Discussion
4.1. General Discussion
4.2. Limitations
4.3. Outlook and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kola, L. Global mental health and COVID-19. Lancet Psychiatry 2020, 7, 655–657. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020. [Google Scholar] [CrossRef] [Green Version]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. The enemy which sealed the world: Effects of COVID-19 diffusion on the psychological state of the Italian population. J. Clin. Med. 2020, 9, 1802. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Henssler, J.; Stock, F.; van Bohemen, J.; Walter, H.; Heinz, A.; Brandt, L. Mental health effects of infection containment strategies: Quarantine and isolation—A systematic review and meta-analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, K.R.; Petkova, E.; Bhui, K.S.; Schulze, T.G. A global needs assessment in times of a global crisis: World psychiatry response to the COVID-19 pandemic. BJPsych Open 2020, 6, e48. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, D.B.; Thapa, B.B.; Katuwal, N.; Shrestha, B.; Pant, C.; Basnet, B.; Mandal, P.; Gurung, A.; Agrawal, A.; Rouniyar, R. Psychological distress in Nepalese residents during COVID-19 pandemic: A community level survey. BMC Psychiatry 2020, 20, 491. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Heinz, A. Cross-cultural validity of psychological distress measurement during the coronavirus pandemic. Pharmacopsychiatry 2020, 53, 237–238. [Google Scholar] [PubMed]
- Pakenham, K.I.; Landi, G.; Boccolini, G.; Furlani, A.; Grandi, S.; Tossani, E. The moderating roles of psychological flexibility and inflexibility on the mental health impacts of COVID-19 pandemic and lockdown in Italy. J. Contextual Behav. Sci. 2020, 17, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Jahanshahi, A.A.; Dinani, M.M.; Madavani, A.N.; Li, J.; Zhang, S.X. The distress of Iranian adults during the Covid-19 pandemic—More distressed than the Chinese and with different predictors. Brain Behav. Immun. 2020, 87, 124–125. [Google Scholar] [CrossRef]
- Zhang, S.X.; Wang, Y.; Jahanshahi, A.A.; Schmitt, V.G.H. Mental distress of adults in Brazil during the COVID-19 crisis. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Costantini, A.; Mazzotti, E. Italian validation of CoViD-19 Peritraumatic Distress Index and preliminary data in a sample of general population. Riv. Psichiatr. 2020, 55, 145–151. [Google Scholar]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Bartelink, V.H.; Zay Ya, K.; Guldbrandsson, K.; Bremberg, S. Unemployment among young people and mental health: A systematic review. Scand. J. Public Health 2020, 48, 544–558. [Google Scholar] [CrossRef]
- Wanberg, C.R.; van Hooft, E.A.; Dossinger, K.; van Vianen, A.E.; Klehe, U.-C. How strong is my safety net? Perceived unemployment insurance generosity and implications for job search, mental health, and reemployment. J. Appl. Psychol. 2020, 105, 209. [Google Scholar] [CrossRef]
- Achdut, N.; Refaeli, T. Unemployment and psychological distress among young people during the COVID-19 pandemic: Psychological resources and risk factors. Int. J. Environ. Res. Public Health 2020, 17, 7163. [Google Scholar] [CrossRef]
- Reichert, A.R.; Tauchmann, H. The causal impact of fear of unemployment on psychological health. Ruhr Econ. Pap. 2011. [Google Scholar] [CrossRef] [Green Version]
- Heinz, A.; Zhao, X.; Liu, S. Implications of the association of social exclusion with mental health. JAMA Psychiatry 2020, 2, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N. Suicides in Greece before and during the period of austerity by sex and age group: Relationship to unemployment and economic variables. J. Affect. Disord. 2020, 260, 174–182. [Google Scholar] [CrossRef]
- Blustein, D.L.; Duffy, R.; Ferreira, J.A.; Cohen-Scali, V.; Cinamon, R.G.; Allan, B.A. Unemployment in the time of COVID-19: A research agenda. J. Vocat. Behav. 2020, 119, 103436. [Google Scholar] [CrossRef] [PubMed]
- Hwang, T.-J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and Social Isolation during the COVID-19 Pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, 1–4. [Google Scholar] [CrossRef]
- Singer, C. Health effects of social isolation and loneliness. J. Aging Life Care 2018, 28, 4–8. [Google Scholar]
- Jeste, D.V.; Lee, E.E.; Cacioppo, S. Battling the modern behavioral epidemic of loneliness: Suggestions for research and interventions. JAMA Psychiatry 2020, 77, 553–554. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [Green Version]
- Xia, N.; Li, H. Loneliness, social isolation, and cardiovascular health. Antioxid. Redox Signal. 2018, 28, 837–851. [Google Scholar] [CrossRef] [Green Version]
- Beutel, M.E.; Klein, E.M.; Brähler, E.; Reiner, I.; Jünger, C.; Michal, M.; Wiltink, J.; Wild, P.S.; Münzel, T.; Lackner, K.J. Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry 2017, 17, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buecker, S.; Horstmann, K.T.; Krasko, J.; Kritzler, S.; Terwiel, S.; Kaiser, T.; Luhmann, M. Changes in daily loneliness during the first four weeks of the Covid-19 lockdown in Germany. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Rauschenberg, C.; Schick, A.; Goetzl, C.; Roehr, S.; Riedel-Heller, S.G.; Koppe, G.; Durstewitz, D.; Krumm, S.; Reininghaus, U. Social isolation, mental health and use of digital interventions in youth during the COVID-19 pandemic: A nationally representative survey. PsyArXiv 2020. [Google Scholar] [CrossRef]
- McGinty, E.E.; Presskreischer, R.; Han, H.; Barry, C.L. Psychological Distress and Loneliness Reported by US Adults in 2018 and April 2020. JAMA 2020, 327, 93–94. [Google Scholar] [CrossRef]
- Luchetti, M.; Lee, J.H.; Aschwanden, D.; Sesker, A.; Strickhouser, J.E.; Terracciano, A.; Sutin, A.R. The trajectory of loneliness in response to COVID-19. Am. Psychol. 2020, 75, 897–908. [Google Scholar] [CrossRef]
- Kissler, S.M.; Tedijanto, C.; Goldstein, E.; Grad, Y.H.; Lipsitch, M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 2020, 368, 860–868. [Google Scholar] [CrossRef]
- Cortez, P.A.; Joseph, S.J.; Das, N.; Bhandari, S.S.; Shoib, S. Tools to measure psychological impact of COVID-19 pandemic: What do we have in the platter? Asian J. Psychiatry 2020, 53, 102371. [Google Scholar] [CrossRef]
- Döring, N.; Bortz, J. Psychometrische Einsamkeitsforschung: Deutsche Neukonstruktion der UCLA Loneliness Scale. Diagnostica 1993, 39, 224–239. [Google Scholar]
- Hays, R.D.; DiMatteo, M.R. A short-form measure of loneliness. J. Personal. Assess. 1987, 51, 69–81. [Google Scholar] [CrossRef]
- Clark, K.A. Unemployed at midlife: Coping strategies that safeguard well-being. Appl. Res. Qual. Life 2020, 1–19. [Google Scholar] [CrossRef]
- Armbruster, S.; Klotzbücher, V. Lost in Lockdown? COVID-19, Social Distancing, and Mental Health in Germany; Diskussionsbeiträge: Freiburg, Germany, 2020. [Google Scholar]
- Shanahan, L.; Steinhoff, A.; Bechtiger, L.; Murray, A.L.; Nivette, A.; Hepp, U.; Ribeaud, D.; Eisner, M. Emotional distress in young adults during the COVID-19 pandemic: Evidence of risk and resilience from a longitudinal cohort study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E. Mental health and wellbeing during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 mental health & wellbeing study. Br. J. Psychiatry 2020, 1–17. [Google Scholar] [CrossRef]
- Qi, M.; Zhou, S.-J.; Guo, Z.-C.; Zhang, L.-G.; Min, H.-J.; Li, X.-M.; Chen, J.-X. The effect of social support on mental health in Chinese adolescents during the outbreak of COVID-19. J. Adolesc. Health 2020, 67, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Marston, C.; Renedo, A.; Miles, S. Community participation is crucial in a pandemic. Lancet 2020, 395, 1676–1678. [Google Scholar] [CrossRef]
- van Agteren, J.; Bartholomaeus, J.; Fassnacht, D.B.; Iasiello, M.; Ali, K.; Lo, L.; Kyrios, M. Using internet-based psychological measurement to capture the deteriorating community mental health profile during COVID-19: Observational Study. JMIR Ment. Health 2020, 7, e20696. [Google Scholar] [CrossRef]
- Ebert, D.D.; Van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.L. Internet-and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Gao, Z.; Lee, J.E.; McDonough, D.J.; Albers, C. Virtual reality exercise as a coping strategy for health and wellness promotion in older adults during the COVID-19 pandemic. J. Clin. Med. 2020, 9, 1986. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Boda, Z.; Elmer, T.; Vörös, A.; Stadtfeld, C. Short-term and long-term effects of a social network intervention on friendships among university students. Sci. Rep. 2020, 10, 2889. [Google Scholar] [CrossRef] [Green Version]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. Evaluation of mental health factors among people with systemic lupus erythematosus during the SARS-CoV-2 pandemic. J. Clin. Med. 2020, 9, 2872. [Google Scholar] [CrossRef] [PubMed]
- Maciaszek, J.; Ciulkowicz, M.; Misiak, B.; Szczesniak, D.; Luc, D.; Wieczorek, T.; Fila-Witecka, K.; Gawlowski, P.; Rymaszewska, J. Mental health of medical and non-medical professionals during the peak of the COVID-19 pandemic: A cross-sectional nationwide study. J. Clin. Med. 2020, 9, 2527. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | N | Mean Age (SEM) | p | Mean Education (SEM) | p | Mean CPDI (SEM) | p | |
|---|---|---|---|---|---|---|---|---|
| Gender | Male | 466 | 39.20 (0.65) | 0.103 | 16.80 (0.20) | 0.760 | 27.66 (0.86) | 0.003 |
| Female | 1437 | 38.03 (0.35) | 16.87 (0.11) | 30.63 (0.49) | ||||
| Age, years | Elder 1 | 927 | 49.82 (0.30) | <0.001 | 17.29 (0.15) | <0.001 | 26.38 (0.57) | <0.001 |
| Younger 1 | 925 | 26.90 (0.15) | 16.35 (0.12) | 33.65 (0.63) | ||||
| Education, years | Higher 2 | 801 | 40.15 (0.41) | <0.001 | 20.61 (0.10) | <0.001 | 25.35 (0.64) | <0.001 |
| Lower 2 | 903 | 37.03 (0.49) | 13.49 (0.06) | 33.64 (0.69) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Heinzel, S.; Haucke, M.N.; Heinz, A. Increased Psychological Distress, Loneliness, and Unemployment in the Spread of COVID-19 over 6 Months in Germany. Medicina 2021, 57, 53. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010053
Liu S, Heinzel S, Haucke MN, Heinz A. Increased Psychological Distress, Loneliness, and Unemployment in the Spread of COVID-19 over 6 Months in Germany. Medicina. 2021; 57(1):53. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010053
Chicago/Turabian StyleLiu, Shuyan, Stephan Heinzel, Matthias N. Haucke, and Andreas Heinz. 2021. "Increased Psychological Distress, Loneliness, and Unemployment in the Spread of COVID-19 over 6 Months in Germany" Medicina 57, no. 1: 53. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010053