1. Introduction
Systemic arterial hypertension is considered a public health problem because it is associated with a high risk of mortality [
1]. Factors such as self-medication [
2], self-measurement and BP control influence non-adherence to treatment due to a lack of knowledge and guidance [
3,
4]. There are several pharmacological and non-pharmacological therapeutic measures that can be applied to control hypertension. However, the general population’s knowledge of hypertension and BP control is still not ideal and, therefore, effective strategies must be developed to improve BP control and treatment adherence [
4].
One of the strategies used by hypertensive patients to achieve these goals is self-measurement of BP at home with the aid of digital devices. Some studies have shown that BP self-measurement allows for a better and/or similar BP prognosis and control than measurements performed in a health care setting [
5,
6,
7,
8]. In addition, BP self-measurement is more attractive to the patients than the usual procedure of making medical appointments [
4]. However, despite the patient’s preference for using the digital device to measure systemic blood pressure, whether for the convenience of carrying out a greater number of measurements during the day, the reliability of BP measurements, that is, the measurement performed by the patient himself, is not unanimously accepted [
4,
9]. This is due to the great variation that occurs in BP due to the lack of posture during the measurement, interferences of the situations experienced by the patient, exposure to stressful events, such as anxiety, throughout the day [
10].
Studies indicate that this self-measurement procedure, when controlled and instructed by the clinician, has positive effects on the diagnosis and adherence to the patient’s treatment [
11,
12,
13], other studies [
4,
9] indicate that it interferes with the control of BP. Such researches aimed to evaluate self-measurement of blood pressure in a controlled and instructed way, regarding the position and indication of correct measurements, by health professionals. However, these investigations were not conducted with the aim of evaluating the association of BP self-measurement in patients with anxiety disorder, for example. It is known that anxiety is one of the factors that influence the increase in blood pressure. Thus, it is suggested that hypertensive patients with anxiety disorder and who perform self-measurement may result in higher occurrences of unscheduled visits to the emergency room and self-medication.
Therefore, the present study aimed to evaluate in hypertensive patients the association of BP self-measurement with its control, as well as the presence of anxiety disorders, the occurrence of unscheduled visits to the emergency room, and self-medication.
2. Methods
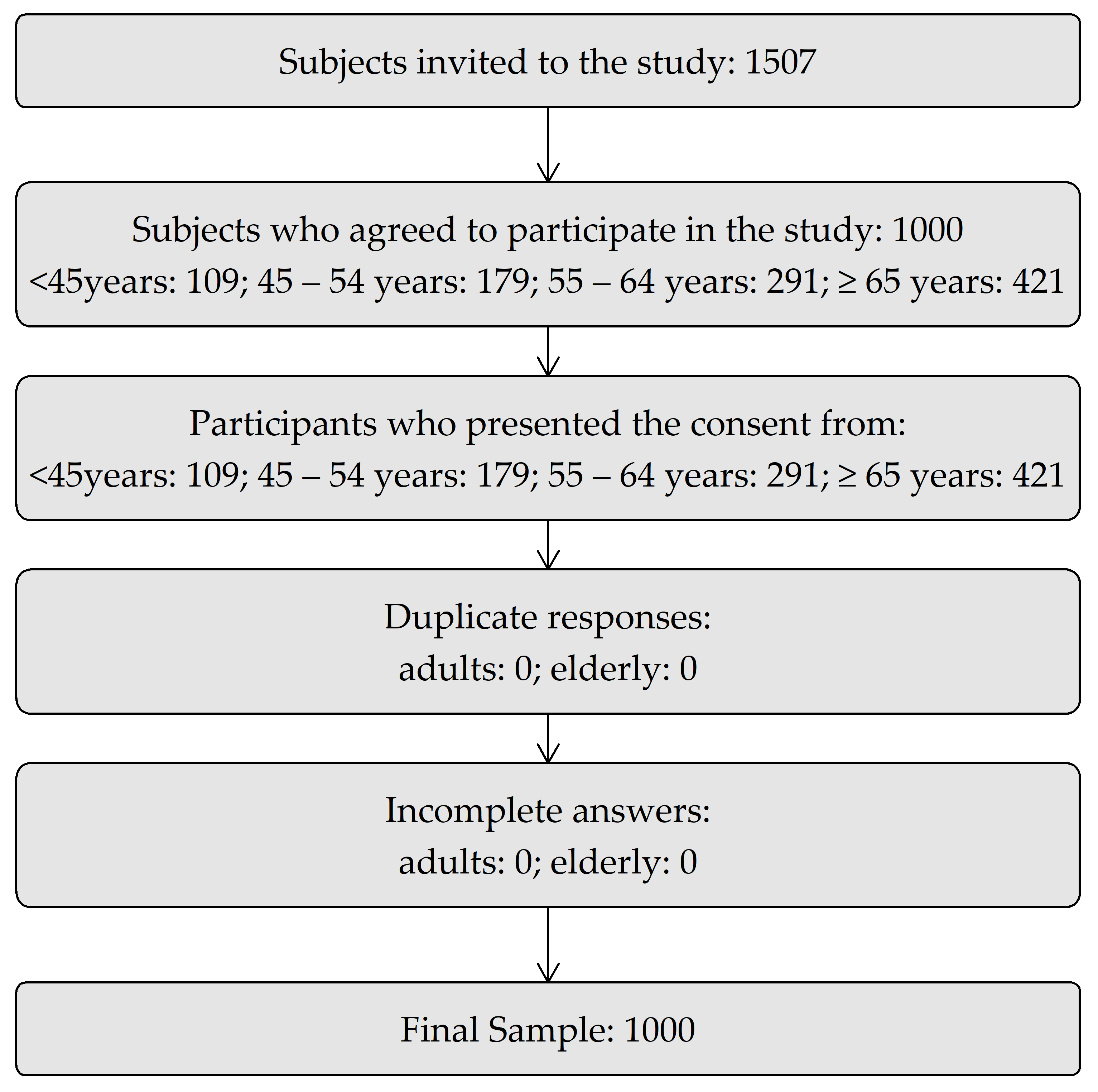
The present study was characterized as cross-sectional and observational with an analytical character, carried out between June 2017 and October 2019 in the city of Aracaju-Sergipe, Brazil. The sample was carried out in a non-random manner with the evaluation of 1000 consecutively selected patients to minimize sampling bias. As an inclusion criterion, patients from 18 years of age, both sexes and diagnosed with systemic arterial hypertension were defined. Those with mental disorders that could compromise the answers to the questionnaires were excluded. Initially, 1507 subjects were invited to participate in the research and 1000 responded that they would accept it. It was found that there were no duplicate or incomplete responses, and 1000 responses were readable for the final analysis (
Figure 1). The classification of age groups was defined based on intervals used by Wang et al. [
14]. The sample was divided into the following groups: <45 years, (39.57 ± 4.28; 57% female and 43% male), 45–54 years (49.71 ± 2.89; 55% female and 45% male), 55–64 years (59.80 ± 2.98; 56% female and 44% male) and ≥65 years (72.49 ± 6.06; 59% female and 41% male).
Data collection was performed through the application of a specific questionnaire for research, which included data related to the patient’s sociodemographic and clinical aspects, quantification of unscheduled visits to the emergency services, self-medication and BP self-assessment. Self-medication related to antihypertensive treatment was considered as the use by the patient of an extra dose of an antihypertensive without a recommendation by a health care professional, the use of another non-prescribed antihypertensive, the non-use of an antihypertensive or not following the prescribed dose. The criterion for a self-measurement was the patient’s report of their frequency of use of the blood pressure (BP) measuring device per day and/or week. An unscheduled visit to the emergency room was based on the patient’s report of visits to the emergency room because of high BP in the last 12 months, as confirmed by their medical records. The control of BP was defined by means of ambulatory blood pressure monitoring (ABPM) or the average of the measurements in the last three consultations that were taken by three assistant physicians according to the College of Cardiology and the cardiology guidelines.
The State-Trait Anxiety Inventory (STAI) was applied by a trained psychologist and information on clinical data and patient identification was collected by a nurse at the Federal University of Sergipe.
The sample consisted of hypertensive patients aged 18 or over, of both sexes, followed up on an outpatient basis at three hospital institutions in the city of Aracaju-Sergipe, Brazil. One of these institutions exclusively serves users of the public health service and two serve the private sector. Those diagnosed with a mental disorder based on the answers to the questionnaires were excluded from the research. Patients who consented to participate in the present study signed an Informed Consent Form. This study was approved by the Research Ethics Committee involving human beings under the number CAAE: 60473316.9.0000.5546.
2.1. Procedures
Data collection was performed through the application of a specific questionnaire covering the following topics: (1) Patient identification and sociodemographic elements (gender, age, income, education, marital status, self-medication, unscheduled visits to the emergency room, information on BP self-checking). The social class and education were inserted in the questionnaire according to the classification used by the Brazilian Institute of Geography and Statistics (IBGE). IBGE is a public institute of the Brazilian federal administration, which provides the geographic and statistical information of Brazil and classifies the social class by family income group, in which class A corresponds to above 20 minimum wages; B: 10 to 20 minimum wages; C: 4 to 10 minimum wages; D: 2 to 4 minimum wages; E: Up to 2 minimum wages. Education is classified as: elementary, high school, university, graduation program and never studied. (2) Clinical data: a cardiologist evaluation based on the average of the last three measurements performed in the last three consultations according to the College of Cardiology and the cardiology and/or ABPM guidelines for the classification of controlled and uncontrolled BP, in addition to the identification of the comorbidities of such patients. BP values were considered for the diagnosis of systemic arterial hypertension (SAH) according to the recommendations of the 2017 guideline, in which the American Society of Cardiology [
15] classifies blood pressure levels differently and suggests a definition for stage 1 blood pressure values. Systolic blood pressure (SBP) between 130–139 mmHg or diastolic blood pressure (DBP) between 80–89 mmHg; Stage 2 hypertension includes subjects with SBP values greater than 140 mmHg or DBP equal to or greater than 90 mmHg. The category of normal blood pressure was defined as SBP less than 120 mmHg and DBP less than 80 mmHg, and elevated BP was classified as SBP between 130–139 mmHg and DBP higher than 90 mmHg. This categorization is justified based on observational data related to the association between diastolic and systolic blood pressure and risk of cardiovascular diseases. To dichotomize the variable in controlled and uncontrolled hypertension, the procedure was carried out through ABPM or by the average of the measurements from the last three consultations performed by three medical assistants according to the College of Cardiology and the guidelines of Brazilian cardiology [
16]. The cutoff point for uncontrolled hypertension was between SBP: 130–139 mmHg or DBP between 80–89 mmHg. Anxiety: the STAI was applied by a trained psychologist to all research volunteers. STAI aims to assess anxiety as a characteristic of the state (E) and personality (T). It is a self-assessment instrument, comprising two parallel scales, each with 20 items [
17]. On STAI, on the T scale according to the sieve, the stipulated average is 45.34 to 55.22 and on the E scale the expected average is 43.64. The internal consistency of both scales was determined based on Cronbach’s alpha. The E scale showed a Cronbach’s alpha of 0.91, while the T scale was 0.894. Therefore, the instruments showed high internal validity when compared to the general population, with an index between 5.6% and 1.8%. Values above 0.8 indicate a high consistency, although coefficients above 0.60 have demonstrated adequate consistency [
18].
2.2. Statistics
The continuous variables were described as mean and standard deviation. As for the categorical variables, absolute frequencies and percentages, and 95% confidence intervals were used to summarize them when relevant. The Shapiro–Wilk test was used to assess the assumption of normality. To test hypotheses related to categorical variables, Pearson’s chi-square test or Fisher’s exact test were used when most appropriate. The comparison between groups (with self-assessment versus without self-assessment; controlled vs. uncontrolled hypertension) was performed using Student’s
t test for independent data in the case of quantitative variables. The Breslow–Day test was applied to assess whether the intensity of the relationship between anxiety (trait and state) and gender is dependent on the age groups. To analyze the factors associated with the outcome variables (self-measurement of systemic BP, uncontrolled hypertension, self-medication, unscheduled visits and trait anxiety), the logistic regression technique was used using the “forward stepwise” and “backward stepwise” method, considering entry in the model
p = 0.25 and remaining in the model
p = 0.05. Then, simple and adjusted odds ratios were calculated. The Statistical Package for Social Sciences version 24.0 was used to perform the statistical calculations for testing. The estimates were made with the following parameters: power = 80%. The effect size (Cohen’s D for continuous variables and Cohen’s h for categorical variables) was defined as small (<0.20), medium (between 0.20 and 0.50), large (between 0.50 and 0.80) and very large (>1, 20) [
19]. The two-tailed p value less than 0.05 was taken as the criterion of statistical significance.
4. Discussion
BP measurement is an important procedure that must be performed for any medical evaluation, regardless of specialty [
20], and in view of the previous information, the main findings of this study were that patients who performed self-measurements had less control over their BP, self-medicated more frequently, had a greater presence of state anxiety and attended the emergency room more frequently because of their BP. These findings seem to point out that there is a lack of knowledge on the part of patients, regarding the self-measurement of blood pressure, and its implications when performing this procedure. Thus, a more effective explanation of how to use the pressure device would minimize the worsening of existing diseases.
The result of this research differs from some studies [
4,
21,
22,
23] on self-measurement and BP control. In the aforementioned studies, patients were instructed on the use, calibration and validation of the blood pressure device before use, in addition to the correct position and BP values for control. However, in the present study, the sample was observed in real-life circumstances, with no guidance on how to use the device. In this case, the objective was to observe how the population has been using the blood pressure device without guidance. Another important point is that factors such as association with anxiety, self-medication and visits to the emergency room were not investigated in the studies cited.
Research has shown that women constitute the majority of the hypertensive population followed in primary health care [
9,
24]. Thus, we found that women have higher frequencies of BP self-measurement (60.2%), that is, they seek greater health care. On the other hand, they presented worse BP control (65.2%). Data from the National Survey on Access, Use and Promotion of Rational Use of Medicines in Brazil (PNAUM) point out that females have a greater influence on the practice of self-medication [
25], a predictive factor for non-adherence to medication [
2] and, consequently, a factor that implies the lack of BP control. In addition, the appearance of physical and psychological disorders such as anxiety, insomnia, tiredness, and irritability are more common in women than in men, in addition to the decrease in the production of estrogens, changes in the lipid profile, weight gain and sedentary lifestyle [
9].
One of the main causes of self-medication is the need to relieve symptoms [
26] and psychosocial factors [
27]. Among the most described symptoms are headache, atypical chest pain, dyspnea, acute psychological stress, anxiety and panic syndrome. When patients associate these symptoms with high BP, this condition is characterized as a false hypertensive crisis [
1]. Among psychiatric disorders, anxiety is the most prevalent in the general population, with prevalence rates between 5.6% and 18.1% [
28]. In women, this prevalence is higher than in men, being a risk factor for elevated BP [
9,
29,
30,
31], which can constitute a barrier to non-BP control [
9,
32]. According to a study by the Global Burden of Disease [
33], the sixth leading cause of disability in the world is related to mental disorders, and individuals affected with anxiety symptoms have lower quality of life and worse psychosocial factor. Individuals with such symptoms tend to present a pattern of recurrence to the disorder and an increasing urgency leading to a chronic course and worsening of other illnesses.
In some studies that analyzed the profile of individuals who seek health services in this country, it was observed that there is a predominance of users who seek urgent care with chronic diseases, such as arterial hypertension, with greater severity due to their lack of control of the condition [
34,
35].
It needs to be taken into account that hypertension is the main treatable cardiovascular risk factor [
36,
37,
38]. Hypertension tends to significantly increase the risk of myocardial infarct, stroke, kidney damage, and other pathologies [
39]. In this sense, ineffective control, especially of hypertension, and cardiovascular problems, would be linked to therapeutic inertia, the use of incorrect dosages and/or inappropriate combinations of medication, low adherence to treatment [
3], an unhealthy lifestyle (smoking, alcohol abuse, excess of fat and salt in the diet, sedentary habits, and being overweight), use of self-assessments in medical guidance and indication, and the prescription of other drugs that can induce hypertension, even when self-administered.
5. Study Limitation
Regarding the limitations of this study, it should be noted that there was no randomization for the use or non-use of the blood pressure device because the devices used were obtained by the patients, which can lead to errors resulting from the use of the device, mistakes regarding knowledge about the device and other distortions.
Another limitation of the study is that there was no standardization regarding the performance of ABPM, since not all patients underwent the exam which can interfere with some results. It is suggested for future work, randomized studies to assess the influence of self-measurement with self-medication, unscheduled visits to the hospital and anxiety disorders.
6. Conclusions
Patients who self-assessed BP had the lowest blood pressure control, self-medicated more frequently, had a greater presence of state anxiety and had more emergency room visits because of their blood pressure. The factors associated with non-BP control were: self-medication, unscheduled visits to the hospital, state of anxiety, prevalence of females, the presence of comorbidities, especially diabetes mellitus and dyslipidemia, and the use of medications for comorbidities.
Thus, the lack of knowledge about the disease and its implications, as well as the wrong guidance on the use of the pressure device are key factors in this chain of events and not BP control. Therefore, it is wise to discourage the use of digital pressure devices in patients to whom adequate guidance has not been given and the clinical picture has been observed, especially if such a patient suffers from an anxiety disorder. In addition, it is wise to invest in public policies aimed at capacitors, informing the population about the proper use of the blood pressure device and pointing out the importance of a multidisciplinary approach in the management of hypertensive patients with anxiety disorder.

 ,
, 

{kind=link}
