
Minimally Invasive Approaching in Hip Surgery—An Anatomical Investigation of 20 Specimens

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alecci, V.; Valente, M.; Crucil, M.; Minerva, M.; Pellegrino, C.-M.; Sabbadini, D.D. Comparison of primary total hip replacements performed with a direct anterior approach versus the standard lateral approach: Perioperative findings. J. Orthop. Traumatol. 2011, 12, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Bal, B.S.; Vallurupalli, S. Minimally invasive total hip arthroplasty with the anterior approach. Indian J. Orthop. 2008, 42, 301–308. [Google Scholar] [CrossRef]
- Bergin, P.F.; Doppelt, J.D.; Kephart, C.J.; Benke, M.T.; Graeter, J.H.; Holmes, A.S.; Haleem-Smith, H.; Tuan, R.S.; Unger, A.S. Comparison of Minimally Invasive Direct Anterior Versus Posterior Total Hip Arthroplasty Based on Inflammation and Muscle Damage Markers. J. Bone Jt. Surg.-Am. Vol. 2011, 93, 1392–1398. [Google Scholar] [CrossRef] [Green Version]
- Bergin, P.F.; Unger, A.S. Direct Anterior Total Hip Arthroplasty. JBJS Essent Surg. Tech. 2011, 1, e15. [Google Scholar] [CrossRef]
- Bernasek, T.L.; Lee, W.S.; Lee, H.J.; Lee, J.S.; Kim, K.H.; Yang, J.J. Minimally invasive primary THA: Anterolateral intermuscular approach versus lateral trans-muscular approach. Arch. Orthop. Trauma Surg. 2010, 130, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Bertin, K.C.; Röttinger, H. Anterolateral mini-incision hip replacement surgery: A modified Watson-Jones approach. Clin. Orthop. Relat. Res. 2004, 429, 248–255. [Google Scholar] [CrossRef]
- Laffosse, J.M.; Chiron, P.; Molinier, F.; Bensafi, H.; Puget, J. Prospective and comparative study of the anterolateral mini-invasive approach versus minimally invasive posterior approach for primary total hip replacement. Early results. Int. Orthop. 2006, 31, 597–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, B.; Mittelstaedt, A.; Schulz, M.S.; Sebena, P.; Singer, J. Comparison of a minimally invasive posterior approach and the standard posterior approach for total hip arthroplasty A prospective and comparative study. J. Orthop. Surg. Res. 2010, 5, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhargava, T.; Goytia, R.N.; Jones, L.C.; Hungerford, M.W. Lateral femoral cutaneous nerve impairment after direct anterior approach for total hip arthroplasty. Orthopedics 2010, 33, 472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldman, B.J. Advancements in Minimally Invasive Total Hip Arthroplasty. Orthopedics 2003, 26, S833–S836. [Google Scholar] [CrossRef]
- Nakamura, S.; Matsuda, K.; Arai, N.; Wakimoto, N.; Matsushita, T. Mini-incision posterior approach for total hip arthroplasty. Int. Orthop. 2004, 28, 214–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadossi, M.; Sambri, A.; Tedesco, G.; Mazzotti, A.; Terrando, S.; Faldini, C. Anterior Approach in Total Hip Replacement. Orthopedics 2017, 40, e553–e556. [Google Scholar] [CrossRef] [Green Version]
- Light, T.R.; Keggi, K.J. Anterior approach to hip arthroplasty. Clin. Orthop. Relat. Res. 1980, 152, 255. [Google Scholar] [CrossRef]
- Sutherland, R.; Rowe, M.J., Jr. Simplified Surgical Approach to the Hip. Arch. Surg. 1944, 48, 144–145. [Google Scholar] [CrossRef]
- D’Arrigo, C.; Speranza, A.; Monaco, E.; Carcangiu, A.; Ferretti, A. Learning curve in tissue sparing total hip replacement: Comparison between different approaches. J. Orthop. Traumatol. 2009, 10, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Matta, J.M.; A Ferguson, T. The anterior approach for hip replacement. Orthopedics 2005, 28, 927–928. [Google Scholar] [CrossRef]
- Rachbauer, F. Minimal-invasive Hüftendoprothetik über einen direkten vorderen Zugang. Der Orthopäde 2005, 34, 1103–1111. [Google Scholar] [CrossRef]
- Christensen, C.P.; Karthikeyan, T.; Jacobs, C.A. Greater Prevalence of Wound Complications Requiring Reoperation with Direct Anterior Approach Total Hip Arthroplasty. J. Arthroplast. 2014, 29, 1839–1841. [Google Scholar] [CrossRef] [PubMed]
- Müller, D.A.; Zingg, P.O.; Dora, C. Anterior Minimally Invasive Approach for Total Hip Replacement: Five-Year Survivorship and Learning Curve. HIP Int. 2014, 24, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Spaans, A.J.; Hout, J.A.A.M.V.; Bolder, S.B.T. High complication rate in the early experience of minimally invasive total hip arthroplasty by the direct anterior approach. Acta Orthop. 2012, 83, 342–346. [Google Scholar] [CrossRef] [Green Version]
- Zeiler, K.; Auff, E.; Deecke, L. Klinische Neurologie I: Grundlagen für Human-und Zahnmediziner; Facultas Verlags-und Buchhandels AG: Vienna, Austria, 2006. [Google Scholar]
- Ropars, M.; Morandi, X.; Huten, D.; Thomazeau, H.; Berton, E.; Darnault, P. Anatomical study of the lateral femoral cutaneous nerve with special reference to minimally invasive anterior approach for total hip replacement. Surg. Radiol. Anat. 2009, 31, 199–204. [Google Scholar] [CrossRef]
- Paillard, P. Hip replacement by a minimal anterior approach. Int. Orthop. 2007, 31, 13–15. [Google Scholar] [CrossRef] [Green Version]
- Carai, A.; Fenu, G.; Sechi, E.; Crotti, F.M.; Montella, A. Anatomical variability of the lateral femoral cutaneous nerve: Findings from a surgical series. Clin. Anat. 2009, 22, 365–370. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
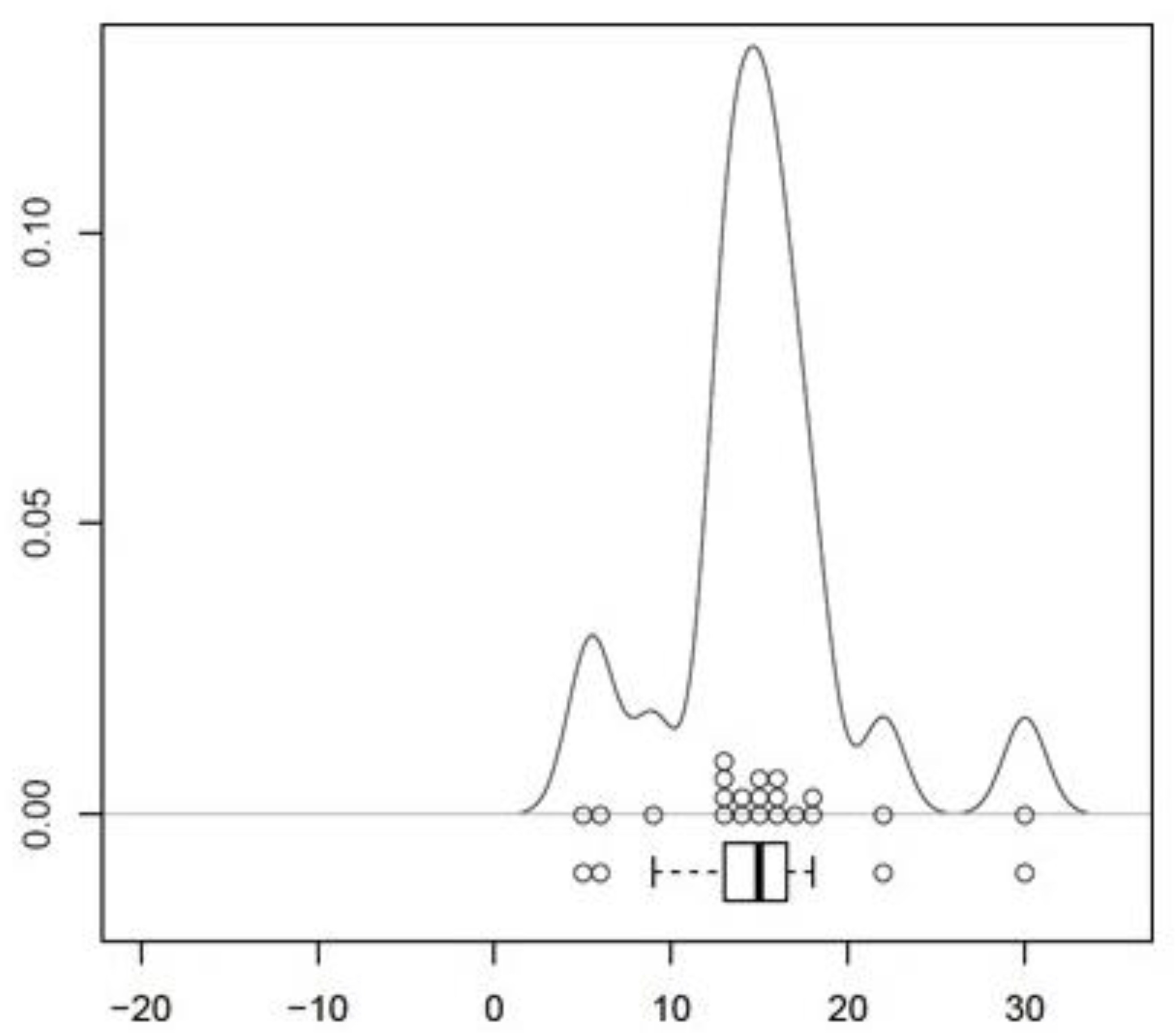
| Mean value | 14.90 mm |
| Standard error | 1.19 mm |
| Confidence interval (CI) | 95%, 12.42–17.38 mm |
| p | <0.001 |
| Direction to the skin incision | 100% medial (n = 20) |
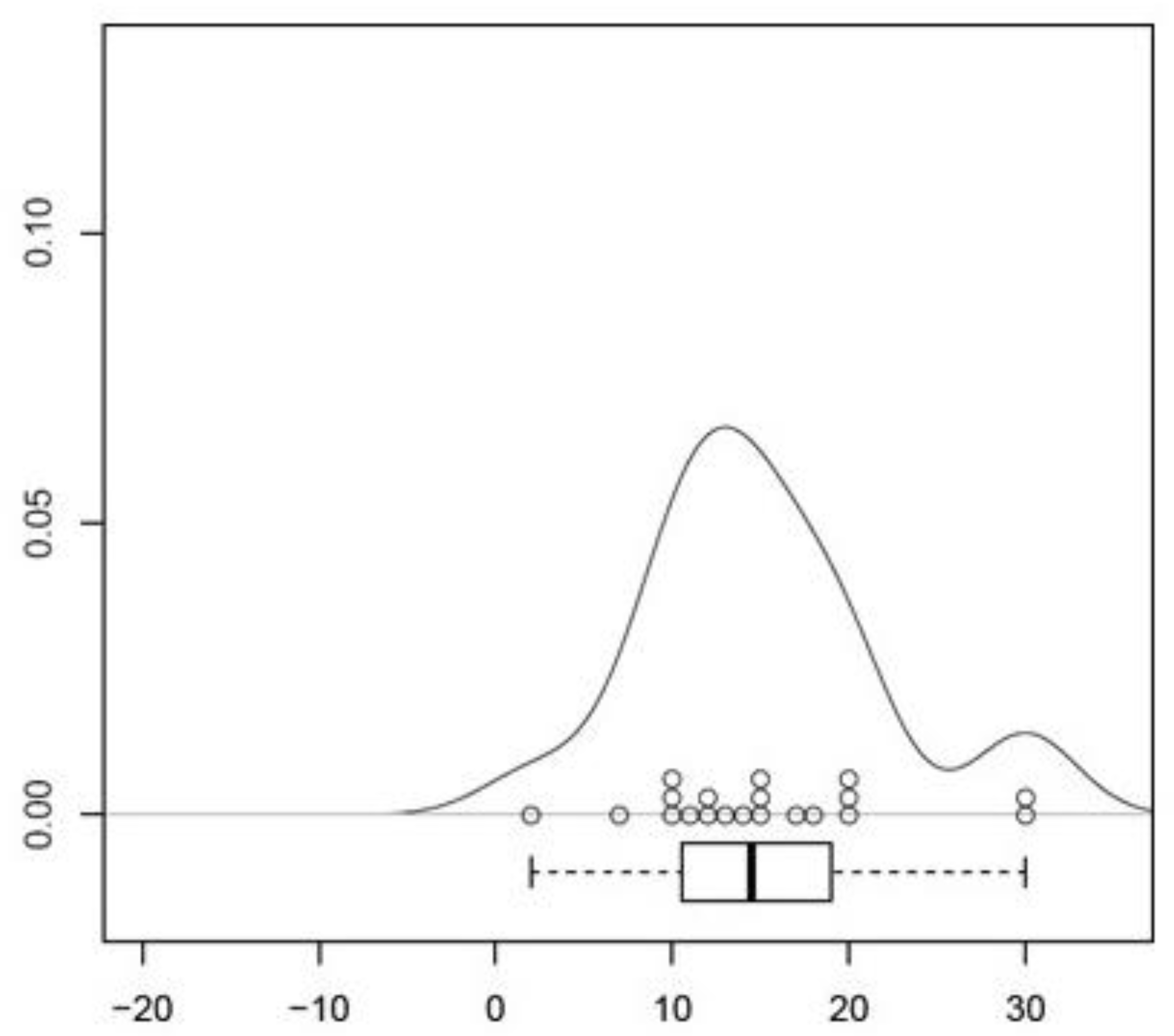
| Mean value | 15.05 mm |
| Standard error | 1.53 mm |
| Confidence interval (CI) | 95%, 11.86–8.24 mm |
| p | <0.001 |
| Direction to the skin incision | 100% medial (n = 20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schopper, C.; Traxler, H.; Schauer, B.; Hipmair, G.; Gotterbarm, T.; Luger, M. Minimally Invasive Approaching in Hip Surgery—An Anatomical Investigation of 20 Specimens. Medicina 2021, 57, 1283. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111283
Schopper C, Traxler H, Schauer B, Hipmair G, Gotterbarm T, Luger M. Minimally Invasive Approaching in Hip Surgery—An Anatomical Investigation of 20 Specimens. Medicina. 2021; 57(11):1283. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111283
Chicago/Turabian StyleSchopper, Clemens, Hannes Traxler, Bernhard Schauer, Günter Hipmair, Tobias Gotterbarm, and Matthias Luger. 2021. "Minimally Invasive Approaching in Hip Surgery—An Anatomical Investigation of 20 Specimens" Medicina 57, no. 11: 1283. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111283