
Clinicopathological Characteristics and Survival Outcomes of Patients with Buccal Squamous Cell Carcinoma: Results of a Multi-Institutional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
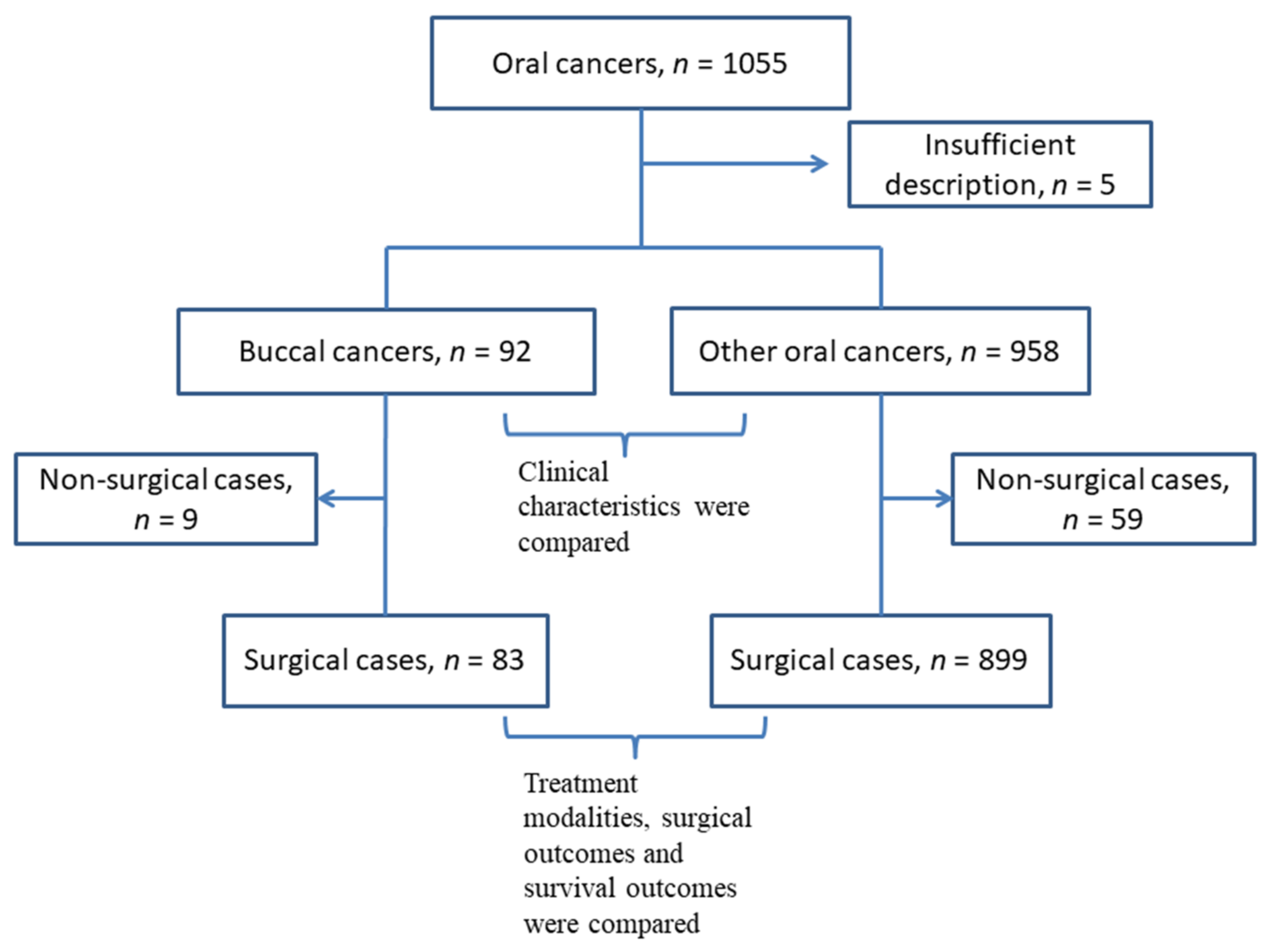
2.1. Patient’s Data Source
2.2. Patient’s Demographics and Clinical Characteristics
2.3. Survival Analysis
2.4. Statistics Analysis
3. Results
3.1. The Difference in Patient Characteristics between Buccal Cancer Patients and Other Oral Cancer Patients
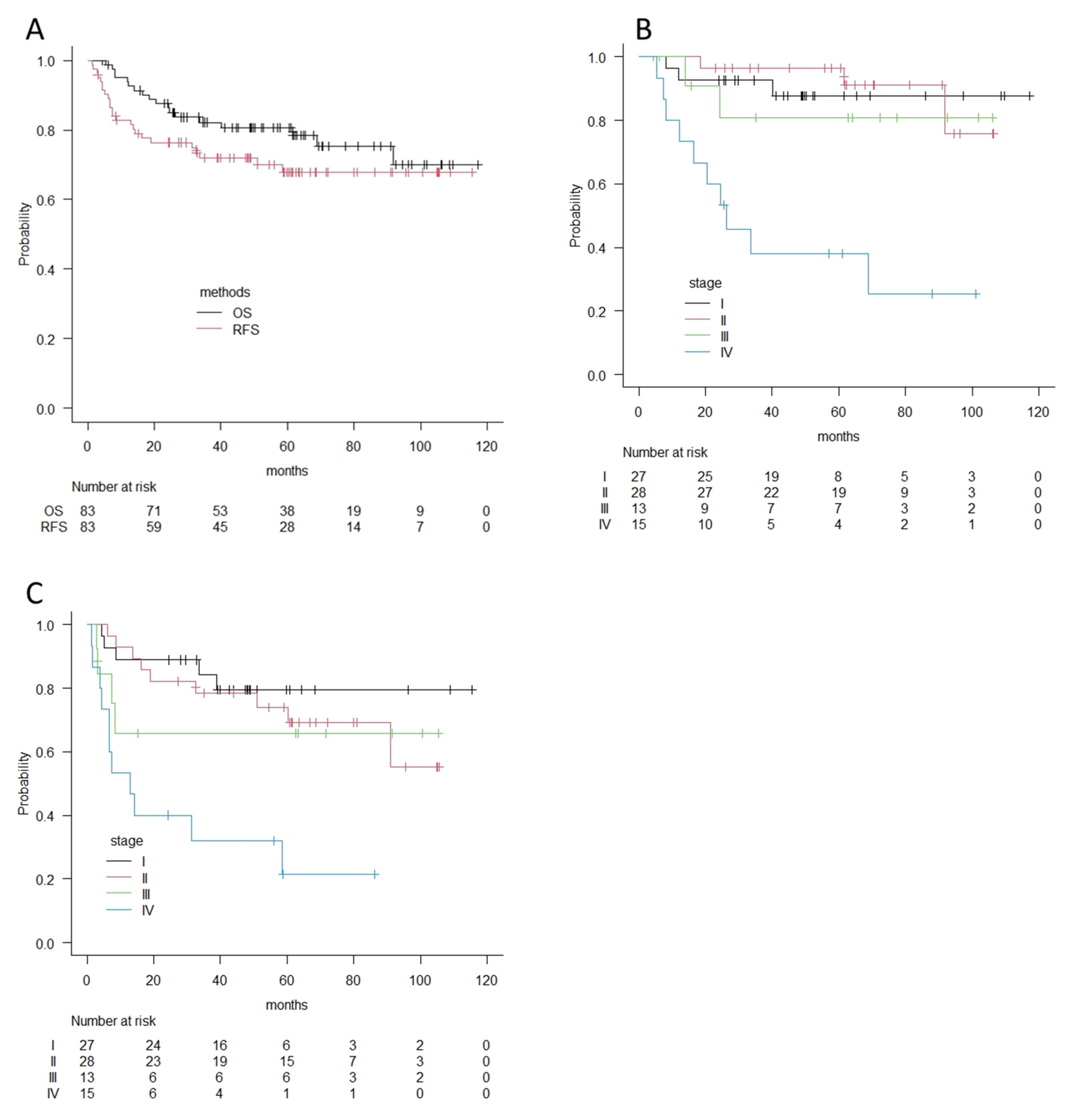
3.2. Survival Outcomes of Buccal Cancer Patients
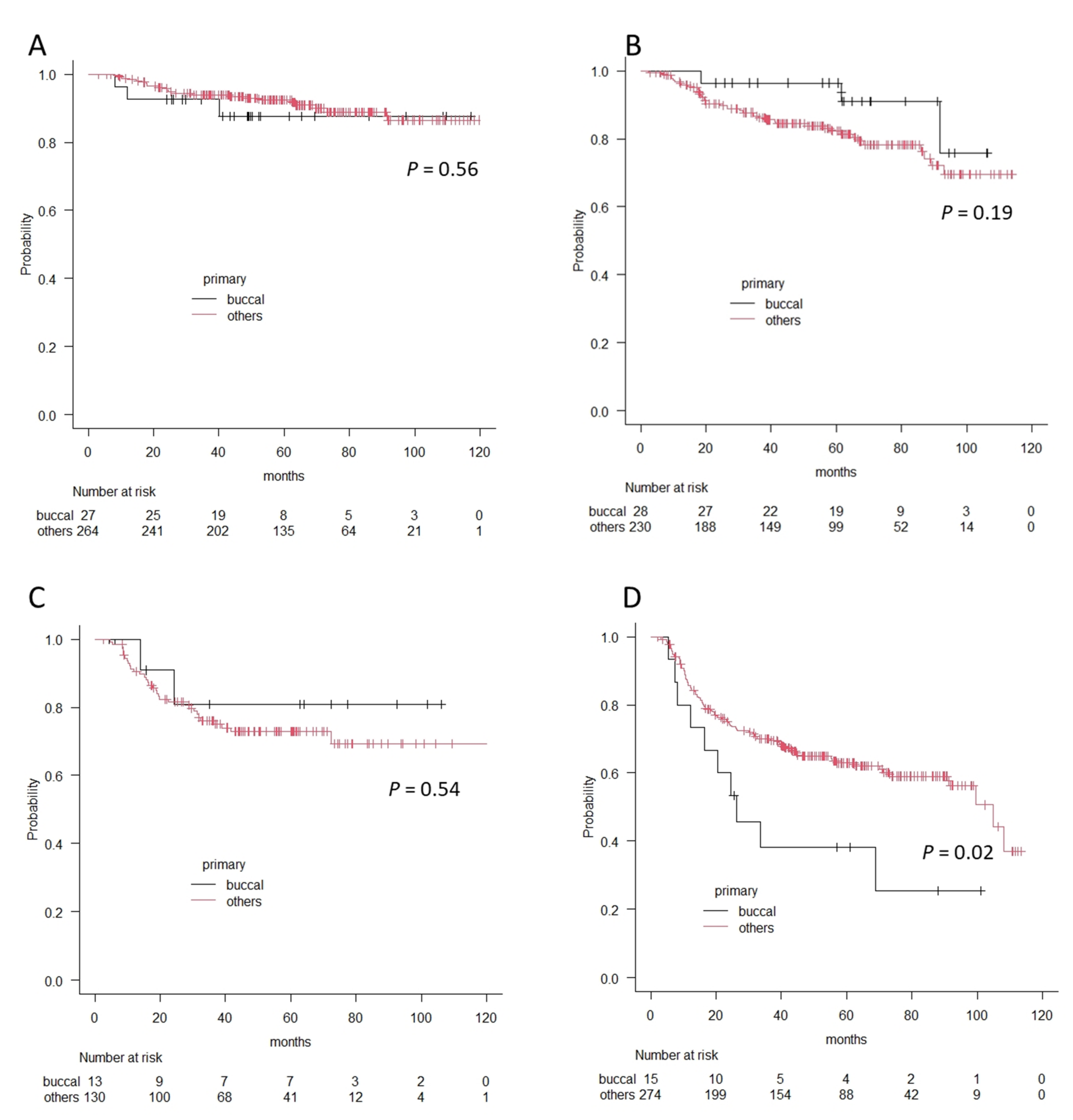
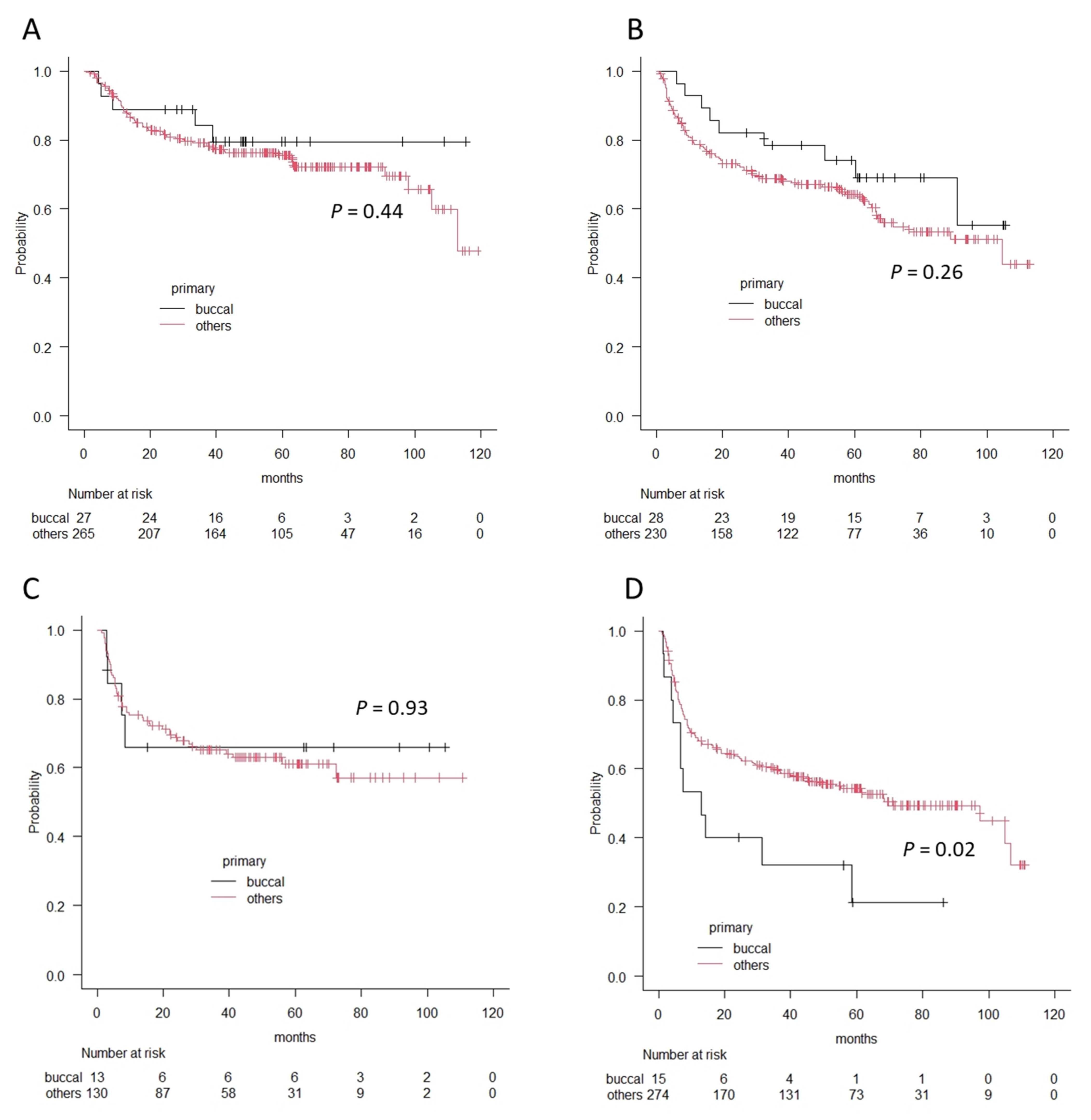
3.3. The Comparison of Survival Outcomes between Buccal Cancer Patients and Other Oral Cancer Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camilon, P.R.; Stokes, W.A.; Fuller, C.W.; Nguyen, S.A.; Lentsch, E.J. Does buccal cancer have worse prognosis than other oral cavity cancers? Laryngoscope 2014, 124, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- Lubek, J.E.; Dyalram, D.; Perera, E.H.; Liu, X.; Ord, R.A. A Retrospective Analysis of Squamous Carcinoma of the Buccal Mucosa: An Aggressive Subsite within the Oral Cavity. J. Oral Maxillofac. Surg. 2013, 71, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, M.; Harada, H.; Asato, R.; Hamaguchi, K.; Tamaki, H.; Mizuta, M.; Hori, R.; Kojima, T.; Honda, K.; Tsujimura, T.; et al. Lingual Lymph Node Metastases as a Prognostic Factor in Oral Squamous Cell Carcinoma-A Retrospective Multicenter Study. Medicina 2021, 57, 374. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, S.A. Surgery for cancer of the buccal mucosa. Semin. Surg. Oncol. 1989, 5, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.T.; Wang, H.M.; Ng, S.H.; Yen, T.C.; Lee, L.Y.; Hsueh, C.; Wei, F.; Chen, I.; Kang, C.; Huang, S.; et al. Good tumor control and survivals of squamous cell carcinoma of buccal mucosa treated with radical surgery with or without neck dissection in Taiwan. Oral Oncol. 2006, 42, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Sieczka, E.; Datta, R.; Singh, A.; Loree, T.; Rigual, N.; Orner, J.; Hicks, W., Jr. Cancer of the buccal mucosa: Are margins and T-stage accurate predictors of local control? Am. J. Otolaryngol. 2001, 22, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.T.; Huang, S.F.; Chen, I.H.; Kang, C.J.; Lin, C.Y.; Fan, K.H.; Wang, H.; Ng, S.; Hsueh, C.; Lee, L.; et al. Tongue and buccal mucosa carcinoma: Is there a difference in outcome? Ann. Surg. Oncol. 2010, 17, 2984–2991. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-F.; Chang, J.T.-C.; Liao, C.-T.; Kang, C.-J.; Lin, C.-Y.; Fan, K.-H.; Wang, H.-M.; Chen, I.-H. The role of elective neck dissection in early stage buccal cancer. Laryngoscope 2014, 125, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Sagheb, K.; Blatt, S.; Kraft, I.S.; Zimmer, S.; Rahimi-Nedjat, R.-K.; Al-Nawas, B.; Walter, C. Outcome and cervical metastatic spread of squamous cell cancer of the buccal mucosa, a retrospective analysis of the past 25 years. J. Oral Pathol. Med. 2016, 46, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Diaz, E.M., Jr.; Holsinger, F.C.; Zuniga, E.R.; Roberts, D.B.; Sorensen, D.M. Squamous cell carcinoma of the buccal mucosa: One institution’s experience with 119 previously untreated patients. Head Neck 2003, 25, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; McGlashan, G.; Woolgar, J.A.; Lowe, D.; Brown, J.S.; Vaughan, E.D.; Rogers, S.N. Prognostic importance of site in squamous cell carcinoma of the buccal mucosa. Br. J. Oral Maxillofac. Surg. 2009, 47, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.S.; Jen, Y.M.; Cheng, M.F.; Lin, Y.S.; Su, W.F.; Hwang, J.M.; Chang, L.; Chao, H.; Liu, D.; Lin, H.; et al. Squamous cell carcinoma of the buccal mucosa: An aggressive cancer requiring multimodality treatment. Head Neck 2006, 28, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Hoda, N.; Bc, R.; Ghosh, S.; Ks, S.; Nathani, J. Cervical lymph node metastasis in squamous cell carcinoma of the buccal mucosa: A retrospective study on pattern of involvement and clinical analysis. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e84–e89. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C.; Tsou, Y.A.; Lin, M.H.; Hua, C.H.; Tseng, H.C.; Bau, D.T.; Tsai, M.H. Impact of neck dissection in early tongue and buccal cancer without neck extension. B-ENT 2011, 7, 97–102. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Buccal | Others | p Value | |
| n = 92 | n = 958 | |||
| Clinical characterstics | ||||
| Age | Range (Median) | 47–94 (73) | 21–98 (69) | <0.01 |
| Gender | Male (%) | 59 (64%) | 591 (61%) | 0.63 |
| Female (%) | 33 (36%) | 368(39%) | ||
| Alcohol | None/Sometimes (%) | 56 (61%) | 510 (53%) | 0.26 |
| Habitual (%) | 36 (39%) | 430 (45%) | ||
| Unknown (%) | 0 (0%) | 18 (2%) | ||
| Smoking | Never/Former (%) | 58 (63%) | 581 (61%) | 0.7 |
| Current (%) | 33 (36%) | 364 (38%) | ||
| Unknown (%) | 1 (1%) | 13(1%) | ||
| UICC TNM classification | ||||
| cT classification | Tis/T1 (%) | 28 (30%) | 283 (30%) | 0.01 * |
| T2 (%) | 42 (46%) | 316 (33%) | ||
| T3 (%) | 9 (10%) | 138 (14%) | ||
| T4a (%) | 7 (8%) | 209 (22%) | ||
| T4b (%) | 6 (7%) | 12 (1%) | ||
| cN classification | N0 (%) | 66 (72%) | 638 (67%) | <0.01 ** |
| N1 (%) | 13 (14%) | 113 (12%) | ||
| N2 (%) | 11 (12%) | 188 (20%) | ||
| N3 (%) | 2 (2%) | 19 (2%) | ||
| M classification | M0 (%) | 91 (99%) | 953 (99%) | 0.49 |
| M1 (%) | 1 (1%) | 5 (1%) | ||
| c Stage | I (%) | 27 (29%) | 267 (28%) | 0.20 *** |
| II (%) | 29 (32%) | 236 (25%) | ||
| III (%) | 14 (15%) | 135 (14%) | ||
| IV (%) | 22 (24%) | 320 (33%) | ||
| Treatment | Surgery (%) | 83 (90%) | 899(94%) | 0.22 |
| Others (%) | 9 (10%) | 59 (6%) | ||
| Variables | Buccal | Others | p Value | |
| n = 83 | n = 899 | |||
| Primary Resection | ||||
| Per oral | 77 (93%) | 739 (82%) | 0.01 | |
| External | 6 (7%) | 160 (18%) | ||
| Neck dissection | ||||
| Yes | 30 (36%) | 479 (53%) | <0.01 | |
| No | 53 (64%) | 420 (47%) | ||
| Reconstruction | ||||
| None | 19 (23%) | 236 (26%) | ||
| Artifiial material | 54 (65%) | 478 (53%) | ||
| Local/pedicled flap | 0 (0%) | 53 (6%) | ||
| Free flap | 10 (12%) | 132 (15%) | ||
| Postoperative treatment | ||||
| Yes | 15 (18%) | 219 (24%) | 0.20 | |
| No | 68 (82%) | 680 (76%) | ||
| Surgical margin | ||||
| Positive | 4 (5%) | 71(8%) | 0.31 | |
| Negative | 79 (95%) | 828 (92%) | ||
| Positive nodes | ||||
| pN positive | 19 (23%) | 214 (24%) | 0.85 * | |
| pN negative | 11 (13%) | 265 (29%) | ||
| not dissected | 53 (64%) | 420 (47%) | ||
| Extracapsular extension | ||||
| Yes | 4 (5%) | 58 (6%) | 0.56 ** | |
| No | 15 (18%) | 156 (17%) | ||
| no positive nodes | 64(77%) | 685(77%) | ||
| Variables | Overall Survival | p Value | Recurrence-Free Survival | p Value | |||
| 2 Years | 5 Years | 2 Years | 5 Years | ||||
| Age | |||||||
| >73 | 82.8% | 77.5% | 0.24 | 70.7% | 63.4% | 0.65 | |
| 73≦ | 87.1% | 84.2% | 77.6% | 65.9% | |||
| Gender | |||||||
| Male | 88.6% | 82.3% | 0.70 | 73.6% | 71.4% | 0.98 | |
| Female | 85.7% | 77.4% | 75.2% | 51.0% | |||
| cT classification | |||||||
| Tis/T1/T2 | 91.0% | 87.5% | <0.01 | 80.4% | 72.7% | 0.04 | |
| T3/T4 | 71.4% | 48.2% | 57.4% | 45.9% | |||
| cN classification | |||||||
| N0 | 91.8% | 87.9% | 0.02 | 85.0% | 75.0% | 0.01 | |
| N1/N2/N3 | 75.0% | 59.2% | 50.0% | 44.4% | |||
| c Stage | |||||||
| I/II | 94.5% | 92.2% | <0.01 | 85.5% | 76.0% | <0.01 | |
| III/IV | 76.8% | 56.1% | 50.6% | 40.9% | |||
| Neck dissection | |||||||
| Yes | 79.7% | 72.5% | 0.22 | 66.7% | 58.3% | 0.50 | |
| No | 92.2% | 85.5% | 82.2% | 73.8% | |||
| Postoperative treatment | |||||||
| Yes | 73.3% | 66.7% | 0.07 | 60.0% | 32.8% | 0.02 | |
| No | 90.9% | 83.9% | 80.2% | 75.9% | |||
| pN classification | |||||||
| N0 | 90.3% | 86.6% | 0.10 | 83.6% | 74.0% | 0.03 | |
| N1/N2/N3 | 78.9% | 61.8% | 52.6% | 46.1% | |||
| Surgical margin | |||||||
| Positive | 66.6% | 66.6% | 0.77 | 66.7% | 66.7% | 0.98 | |
| Negative | 87.1% | 81.2% | 76.7% | 67.7% | |||
| Extracapsular extension | |||||||
| Positive | 50.0% | 50.0% | 0.08 | 50.0% | 50.0% | 0.22 | |
| Negative/no positive nodes | 89.6% | 82.2% | 77.7% | 68.6% | |||
| Variables | Overall Survival | Recurrence-Free Survival | |||||||
| HR | 95%CI | p Value | HR | 95%CI | p Value | ||||
| Age | >73 vs. 73≦ | 0.644 | 0.207 | 2.00 | 0.45 | 0.804 | 0.344 | 1.880 | 0.61 |
| Gender | Male vs. Female | 1.904 | 0.627 | 5.77 | 0.26 | 1.624 | 0.708 | 3.724 | 0.25 |
| cT classification | T3/T4 vs. Tis/T1/T2 | 4.921 | 1.519 | 15.94 | <0.01 | 3.084 | 1.001 | 9.500 | 0.04 |
| cN classification | N1/N2/N3 vs. N0 | 2.376 | 0.359 | 15.72 | 0.37 | 3.474 | 0.344 | 22.700 | 0.19 |
| Neck dissection | Yes vs. No | 0.473 | 0.114 | 1.95 | 0.30 | 0.123 | 0.021 | 0.724 | 0.02 |
| Postoperative treatment | Yes vs. No | 1.188 | 0.284 | 4.95 | 0.81 | 2.121 | 5.985 | 5.985 | 0.15 |
| pN classification | N1/N2/N3 vs. N0 | 0.944 | 0.172 | 5.17 | 0.95 | 2.804 | 0.541 | 14.520 | 0.21 |
| Surgical margin | Positive vs. Negative | 2.046 | 0.231 | 18.07 | 0.52 | 0.719 | 0.093 | 5.571 | 0.75 |
| Extracapsular extension | Positive vs. Negative/no positive nodes | 1.027 | 0.151 | 6.96 | 0.98 | 0.344 | 0.054 | 2.180 | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shinohara, S.; Kikuchi, M.; Harada, H.; Hamaguchi, K.; Asato, R.; Tamaki, H.; Mizuta, M.; Hori, R.; Kojima, T.; Honda, K.; et al. Clinicopathological Characteristics and Survival Outcomes of Patients with Buccal Squamous Cell Carcinoma: Results of a Multi-Institutional Study. Medicina 2021, 57, 1361. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121361
Shinohara S, Kikuchi M, Harada H, Hamaguchi K, Asato R, Tamaki H, Mizuta M, Hori R, Kojima T, Honda K, et al. Clinicopathological Characteristics and Survival Outcomes of Patients with Buccal Squamous Cell Carcinoma: Results of a Multi-Institutional Study. Medicina. 2021; 57(12):1361. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121361
Chicago/Turabian StyleShinohara, Shogo, Masahiro Kikuchi, Hiroyuki Harada, Kiyomi Hamaguchi, Ryo Asato, Hisanobu Tamaki, Masanobu Mizuta, Ryusuke Hori, Tsuyoshi Kojima, Keigo Honda, and et al. 2021. "Clinicopathological Characteristics and Survival Outcomes of Patients with Buccal Squamous Cell Carcinoma: Results of a Multi-Institutional Study" Medicina 57, no. 12: 1361. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121361