
Sleep Quality Improvement Enhances Neuropsychological Recovery and Reduces Blood Aβ42/40 Ratio in Patients with Mild–Moderate Cognitive Impairment


Abstract
:1. Introduction
2. Materials and Methods
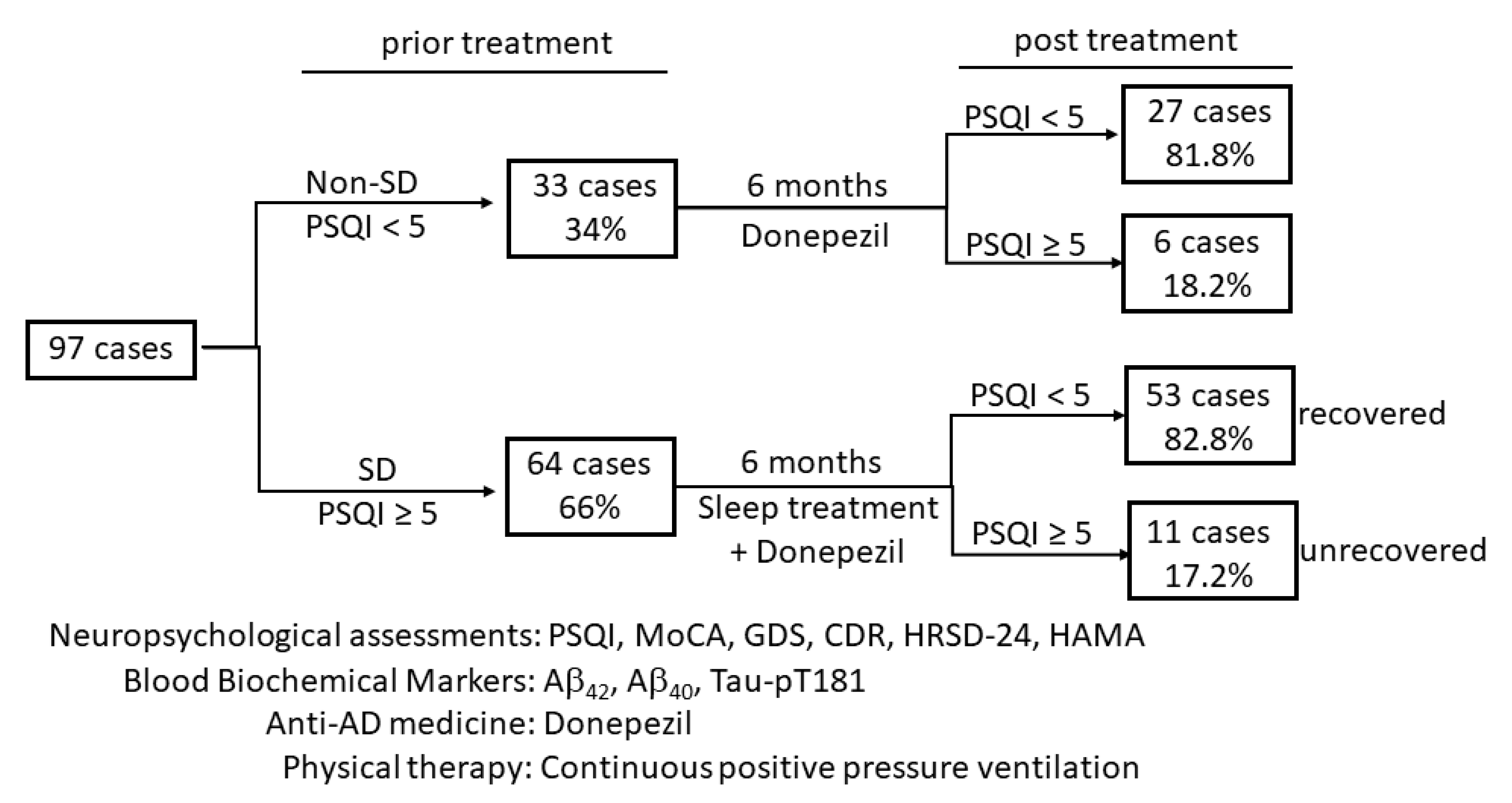
2.1. Study Design and Patients
2.1.1. General Procedures
2.1.2. Sleep Quality Evaluation
2.1.3. Assessment of Neuropsychological Status
2.2. Measurement of Blood Levels of Amyloid Peptides and Tau-pT181 Proteins
2.3. The Intervention of Sleep Disorders and Dementia
2.4. Data Collection and Statistical Analysis
3. Results
3.1. Patients Population and Clinical Parameters
3.2. Sleep Quality Was Associated with Neuropsychological Symptoms and Blood Biomarkers
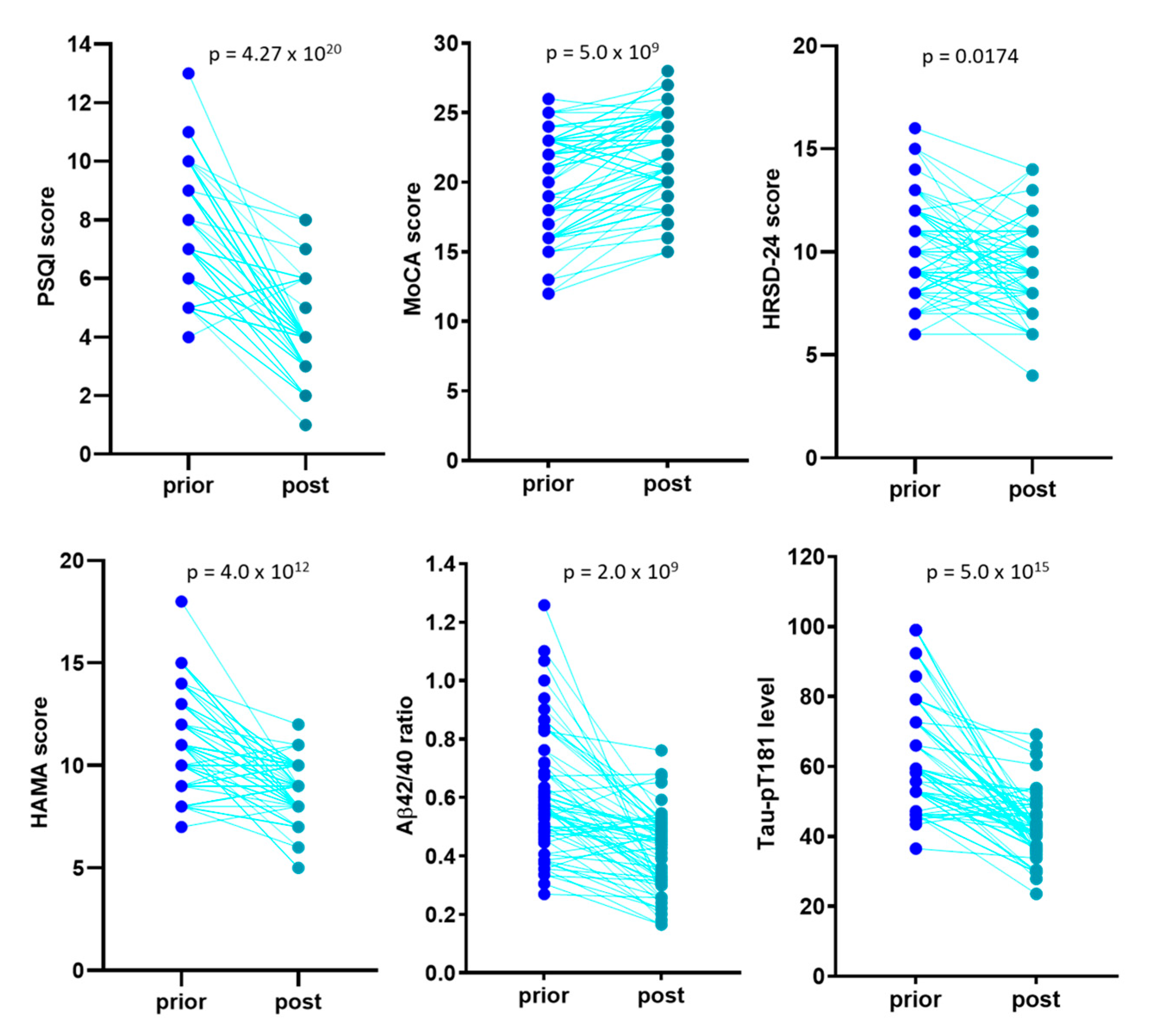
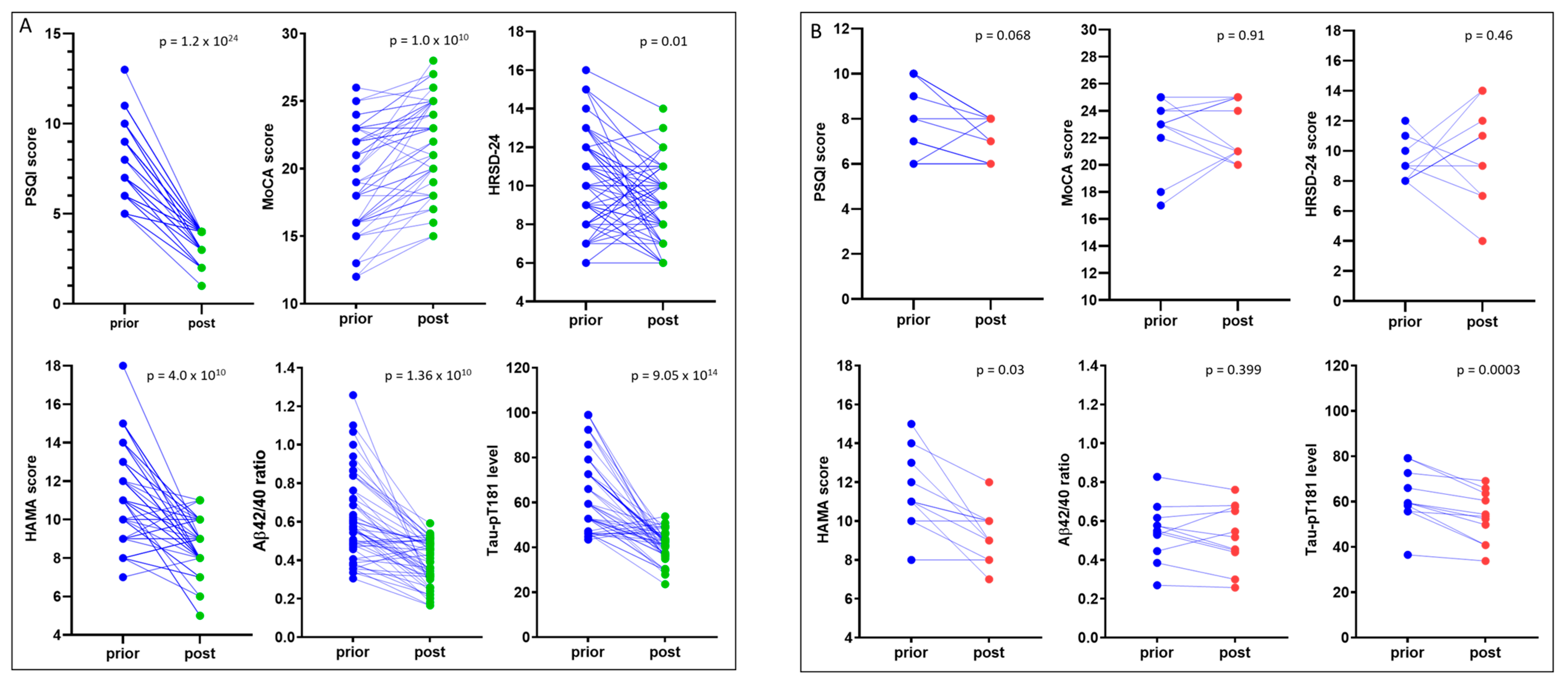
3.3. Sleep Treatment Improves COGNITION and Relieves Anxiety
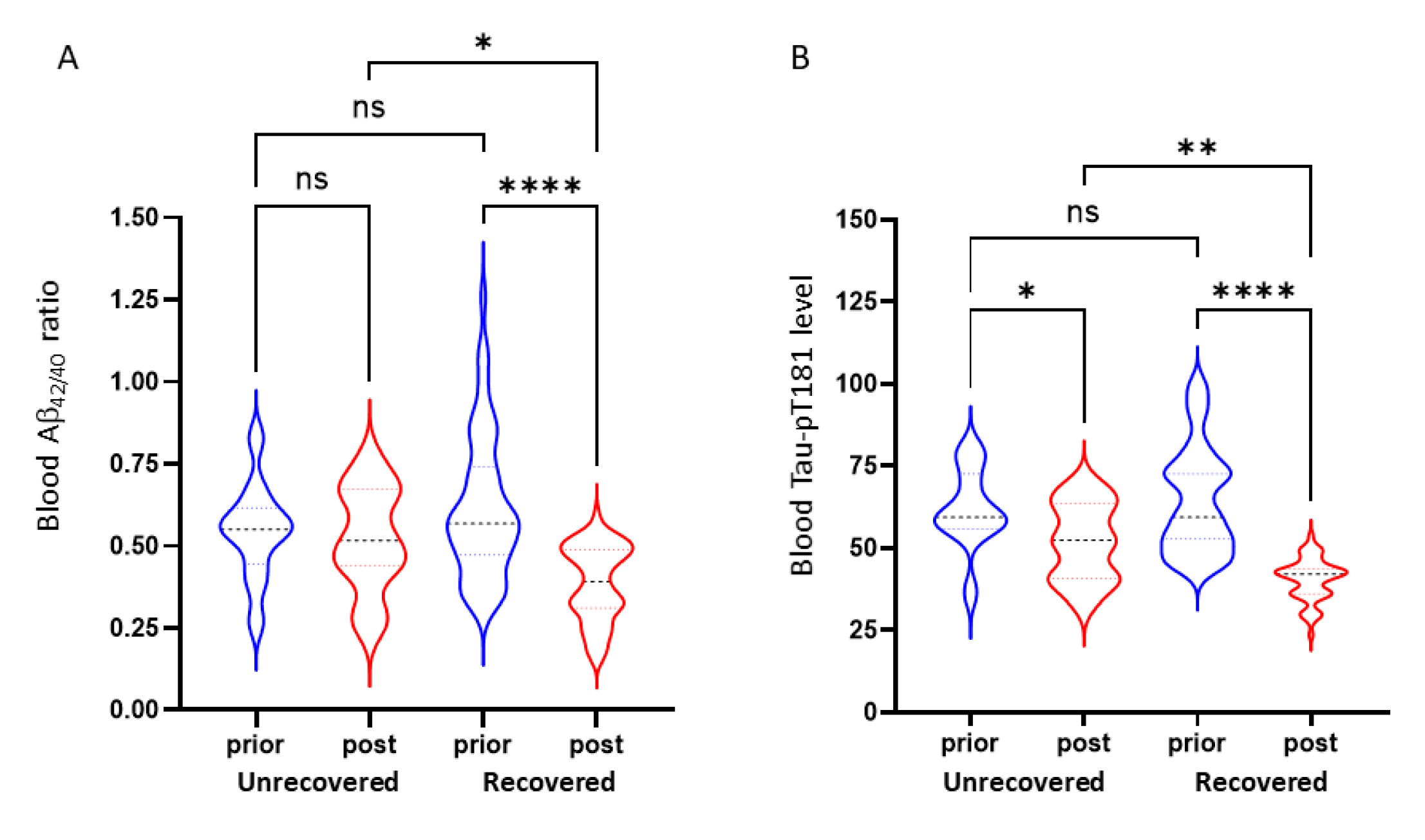
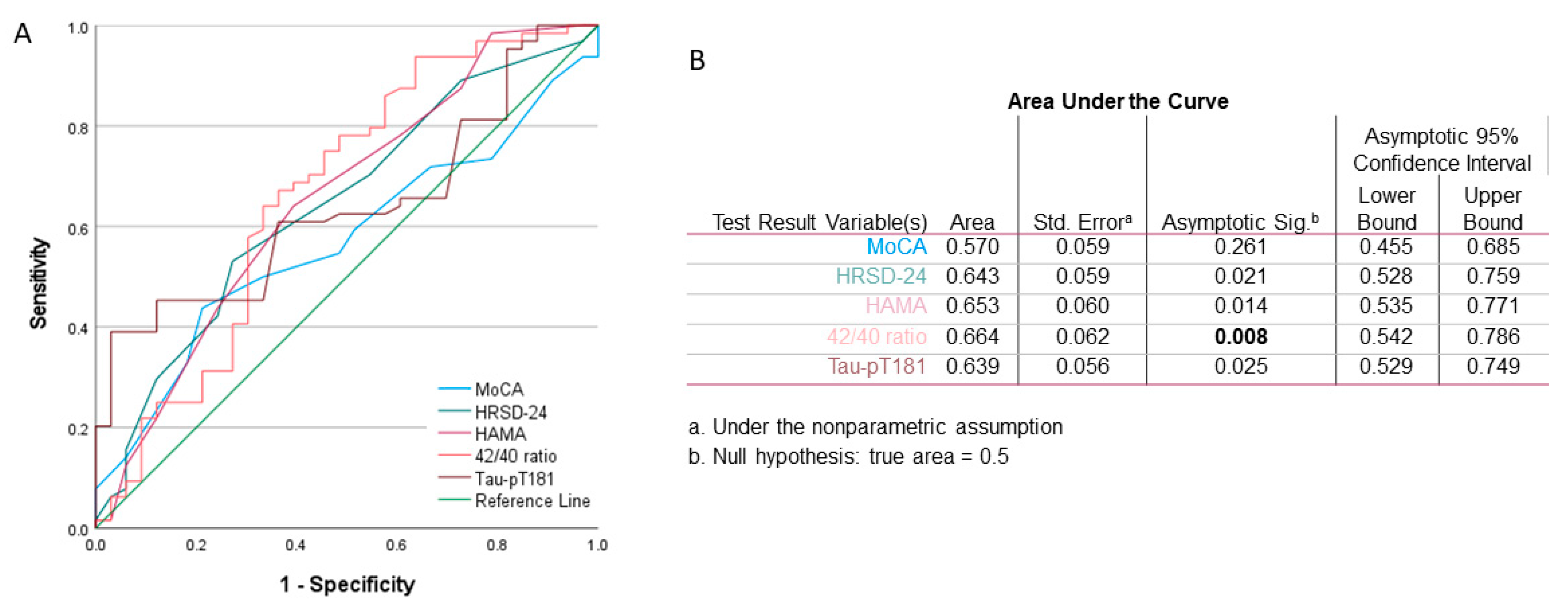
3.4. Blood Amyloid-β42/40 Ratio Is a Predictive Factor for Sleep Quality in MCI Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kivipelto, M.; Mangialasche, F.; Snyder, H.M.; Allegri, R.; Andriey, S.; Arai, H.; Baker, L.; Belleville, S.; Brodaty, H.; Brucki, S.M.; et al. World-Wide FINGERS Network: A global approach to risk reduction and prevention of dementia. Alzheimers Dement 2020, 16, 1078–1094. [Google Scholar] [CrossRef]
- Alzheimer’s Association Report. 2020 Alzheimer’s disease facts and figures. Alzheimers Dement 2020, 16, 391–460. [Google Scholar] [CrossRef]
- Polanco, J.C.; Li, C.; Bodea, L.G.; Martinez-Marmol, R.; Meunier, F.A.; Gotz, J. Amyloid-beta and tau complexity—Towards improved biomarkers and targeted therapies. Nat. Rev. Neurol. 2018, 14, 22–39. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.A.; Blazey, T.M.; Su, Y.; Hari-Raj, A.; Dincer, A.; Flores, S.; Christensen, J.; McDade, E.; Wang, G.; Xiong, C.; et al. Spatial patterns of neuroimaging biomarker change in individuals from families with autosomal dominant Alzheimer’s disease: A longitudinal study. Lancet Neurol. 2018, 17, 241–250. [Google Scholar] [CrossRef] [Green Version]
- De Strooper, B.; Karran, E. The Cellular Phase of Alzheimer’s Disease. Cell 2016, 164, 603–615. [Google Scholar] [CrossRef] [Green Version]
- Selkoe, D.J.; Hardy, J. The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO Mol. Med. 2016, 8, 595–608. [Google Scholar] [CrossRef]
- D’Abramo, C.; D’Adamio, L.; Giliberto, L. Significance of Blood and Cerebrospinal Fluid Biomarkers for Alzheimer’s Disease: Sensitivity, Specificity and Potential for Clinical Use. J. Pers. Med. 2020, 10, 116. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, G.; Holtzman, D.M. Amyloid-beta and Tau at the Crossroads of Alzheimer’s Disease. Adv. Exp. Med. Biol. 2019, 1184, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Roman, M.; Pulopulos, M.M.; Baquero, M.; Salvador, A.; Cuevas, A.; Ferrer, I.; Ciopat, O.; Gomez, E. Obstructive sleep apnea and Alzheimer’s disease-related cerebrospinal fluid biomarkers in mild cognitive impairment. Sleep 2020, 44, zsaa133. [Google Scholar] [CrossRef]
- Hefti, M.M.; Kim, S.; Bell, A.J.; Betters, R.K.; Fiock, K.L.; Iida, M.A.; Smalley, M.E.; Farrell, K.; Fowkes, M.E.; Crary, J.F. Tau Phosphorylation and Aggregation in the Developing Human Brain. J. Neuropathol. Exp. Neurol. 2019, 78, 930–938. [Google Scholar] [CrossRef]
- Olsson, B.; Lautner, R.; Andreasson, U.; Ohrfelt, A.; Portelius, E.; Bjerke, M.; Holtta, M.; Rosen, C.; Olsson, C.; Strobel, G.; et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: A systematic review and meta-analysis. Lancet Neurol. 2016, 15, 673–684. [Google Scholar] [CrossRef]
- Borges, C.R.; Poyares, D.; Piovezan, R.; Nitrini, R.; Brucki, S. Alzheimer’s disease and sleep disturbances: A review. Arq. Neuropsiquiatr. 2019, 77, 815–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bubu, O.M.; Brannick, M.; Mortimer, J.; Umasabor-Bubu, O.; Sebastiao, Y.V.; Wen, Y.; Schwartz, S.; Borenstein, A.R.; Wu, Y.; Morgan, D.; et al. Sleep, Cognitive impairment, and Alzheimer’s disease: A Systematic Review and Meta-Analysis. Sleep 2017, 40, piizsw032. [Google Scholar] [CrossRef]
- Wang, C.; Holtzman, D.M. Bidirectional relationship between sleep and Alzheimer’s disease: Role of amyloid, tau, and other factors. Neuropsychopharmacology 2020, 45, 104–120. [Google Scholar] [CrossRef]
- Ulland, T.K.; Ewald, A.C.; Knutson, A.O.; Marino, K.M.; Smith, S.M.C.; Watters, J.J. Alzheimer’s Disease, Sleep-disordered breathing, and Microglia: Puzzling out a Common Link. Cells 2021, 10, 2907. [Google Scholar] [CrossRef] [PubMed]
- Bliwise, D.L. Sleep disorders in Alzheimer’s disease and other dementias. Clin. Cornerstone 2004, 6, S16–S28. [Google Scholar] [CrossRef]
- Bubu, O.M.; Umasabor-Bubu, O.Q.; Turner, A.D.; Parekh, A.; Mullins, A.E.; Kam, K.; Birckbichler, M.K.; Mukhtar, F.; Mbah, A.K.; Williams, N.J.; et al. Self-reported obstructive sleep apnea, amyloid and tau burden, and Alzheimer’s disease time-dependent progression. Alzheimers Dement 2020, 17, 226–245. [Google Scholar] [CrossRef] [PubMed]
- Barthelemy, N.R.; Liu, H.; Lu, W.; Kotzbauer, P.T.; Bateman, R.J.; Lucey, B.P. Sleep Deprivation Affects Tau Phosphorylation in Human Cerebrospinal Fluid. Ann. Neurol. 2020, 87, 700–709. [Google Scholar] [CrossRef]
- Blattner, M.S.; Panigrahi, S.K.; Toedebusch, C.D.; Hicks, T.J.; McLeland, J.S.; Banks, I.R.; Schaibley, C.; Ovod, V.; Mawuenyega, K.G.; Bateman, R.J.; et al. Increased Cerebrospinal Fluid Amyloid-beta During Sleep Deprivation in Healthy Middle-Aged Adults Is Not Due to Stress or Circadian Disruption. J. Alzheimers Dis. 2020, 75, 471–482. [Google Scholar] [CrossRef]
- Lucey, B.P.; Hicks, T.J.; McLeland, J.S.; Toedebusch, C.D.; Boyd, J.; Elbert, D.L.; Patterson, B.W.; Baty, J.; Morris, J.C.; Ovod, V.; et al. Effect of sleep on overnight cerebrospinal fluid amyloid beta kinetics. Ann. Neurol. 2018, 83, 197–204. [Google Scholar] [CrossRef]
- Holth, J.K.; Fritschi, S.K.; Wang, C.; Pedersen, N.P.; Cirrito, J.R.; Mahan, T.E.; Finn, M.B.; Manis, M.; Geerling, J.C.; Fuller, P.M.; et al. The sleep-wake cycle regulates brain interstitial fluid tau in mice and CSF tau in humans. Science 2019, 363, 880–884. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Palmer, B.W.; Cooke, J.R.; Corey-Bloom, J.; Fiorentino, L.; Natarajan, L.; Liu, L.; Ayalon, L.; He, F.; Loredo, J.S. Cognitive effects of treating obstructive sleep apnea in Alzheimer’s disease: A randomized controlled study. J. Am. Geriatr. Soc. 2008, 56, 2076–2081. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep drives metabolite clearance from the adult brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Lucey, B.P. It’s complicated: The relationship between sleep and Alzheimer’s disease in humans. Neurobiol. Dis. 2020, 144, 105031. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Friedman, L.; Ancoli-Israel, S.; Bliwise, D.; Singer, C.; Vitiello, M.V.; Monjan, A.A.; Lebowitz, B. Development of diagnostic criteria for defining sleep disturbance in Alzheimer’s disease. J. Geriatr. Psychiatry Neurol. 2003, 16, 131–139. [Google Scholar] [CrossRef]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Tsai, P.S.; Wang, S.Y.; Wang, M.Y.; Su, C.T.; Yang, T.T.; Huang, C.J.; Fang, S.C. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, R.; Xiao, Y.; Dong, J.; Niu, X.; Kong, W. Reliability and Validity of the Beijing Version of the Montreal Cognitive Assessment in the Evaluation of Cognitive Function of Adult Patients with OSAHS. PLoS ONE 2015, 10, e0132361. [Google Scholar] [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M. Rating depressive patients. J. Clin. Psychiatry 1980, 41, 21–24. [Google Scholar]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Magierski, R.; Sobow, T.; Schwertner, E.; Religa, D. Pharmacotherapy of Behavioral and Psychological Symptoms of Dementia: State of the Art and Future Progress. Front. Pharmacol. 2020, 11, 1168. [Google Scholar] [CrossRef]
- De Oliveira, F.F.; Bertolucci, P.H.; Chen, E.S.; Smith Mde, A. Assessment of sleep satisfaction in patients with dementia due to Alzheimer’s disease. J. Clin. Neurosci. 2014, 21, 2112–2117. [Google Scholar] [CrossRef]
- Zhou, G.; Liu, S.; Yu, X.; Zhao, X.; Ma, L.; Shan, P. High prevalence of sleep disorders and behavioral and psychological symptoms of dementia in late-onset Alzheimer disease: A study in Eastern China. Medicine 2019, 98, e18405. [Google Scholar] [CrossRef] [PubMed]
- Stella, F.; Laks, J.; Govone, J.S.; de Medeiros, K.; Forlenza, O.V. Association of neuropsychiatric syndromes with global clinical deterioration in Alzheimer’s disease patients. Int. Psychogeriatr. 2016, 28, 779–786. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Wei, M.; Ding, W. Changes in Cognitive Function in Patients with Primary Insomnia. Shanghai Arch. Psychiatry 2017, 29, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Mullins, A.E.; Kam, K.; Parekh, A.; Bubu, O.M.; Osorio, R.S.; Varga, A.W. Obstructive Sleep Apnea and Its Treatment in Aging: Effects on Alzheimer’s disease Biomarkers, Cognition, Brain Structure and Neurophysiology. Neurobiol. Dis. 2020, 145, 105054. [Google Scholar] [CrossRef] [PubMed]
- Karikari, T.K.; Pascoal, T.A.; Ashton, N.J.; Janelidze, S.; Benedet, A.L.; Rodriguez, J.L.; Chamoun, M.; Savard, M.; Kang, M.S.; Therriault, J.; et al. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: A diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol. 2020, 19, 422–433. [Google Scholar] [CrossRef]
- Thijssen, E.H.; La Joie, R.; Wolf, A.; Strom, A.; Wang, P.; Iaccarino, L.; Bourakova, V.; Cobigo, Y.; Heuer, H.; Spina, S.; et al. Diagnostic value of plasma phosphorylated tau181 in Alzheimer’s disease and frontotemporal lobar degeneration. Nat. Med. 2020, 26, 387–397. [Google Scholar] [CrossRef]
- Ashton, N.J.; Leuzy, A.; Karikari, T.K.; Mattsson-Carlgren, N.; Dodich, A.; Boccardi, M.; Corre, J.; Drzezga, A.; Nordberg, A.; Ossenkoppele, R.; et al. The validation status of blood biomarkers of amyloid and phospho-tau assessed with the 5-phase development framework for AD biomarkers. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2140–2156. [Google Scholar] [CrossRef] [PubMed]
- Cianflone, A.; Coppola, L.; Mirabelli, P.; Salvatore, M. Predictive Accuracy of Blood-Derived Biomarkers for Amyloid-beta Brain Deposition Along with the Alzheimer’s Disease Continuum: A Systematic Review. J. Alzheimers Dis. 2021, 84, 393–407. [Google Scholar] [CrossRef]
- Stockmann, J.; Verberk, I.M.W.; Timmesfeld, N.; Denz, R.; Budde, B.; Lange-Leifhelm, J.; Scheltens, P.; van der Flier, W.M.; Nabers, A.; Teunissen, C.E.; et al. Amyloid-beta misfolding as a plasma biomarker indicates risk for future clinical Alzheimer’s disease in individuals with subjective cognitive decline. Alzheimers Res. Ther. 2020, 12, 169. [Google Scholar] [CrossRef]
- Lucey, B.P.; McCullough, A.; Landsness, E.C.; Toedebusch, C.D.; McLeland, J.S.; Zaza, A.M.; Fagan, A.M.; McCue, L.; Xiong, C.; Morris, J.C.; et al. Reduced non-rapid eye movement sleep is associated with tau pathology in early Alzheimer’s disease. Sci. Transl. Med. 2019, 11, eaau6550. [Google Scholar] [CrossRef]
- Ju, Y.E.; McLeland, J.S.; Toedebusch, C.D.; Xiong, C.; Fagan, A.M.; Duntley, S.P.; Morris, J.C.; Holtzman, D.M. Sleep quality and preclinical Alzheimer disease. JAMA Neurol. 2013, 70, 587–593. [Google Scholar] [CrossRef]
- Nakamura, A.; Kaneko, N.; Villemagne, V.L.; Kato, T.; Doecke, J.; Dore, V.; Fowler, C.; Li, Q.X.; Martins, R.; Rowe, C.; et al. High performance plasma amyloid-beta biomarkers for Alzheimer’s disease. Nature 2018, 554, 249–254. [Google Scholar] [CrossRef]
- Clark, C.M.; Schneider, J.A.; Bedell, B.J.; Beach, T.G.; Bilker, W.B.; Mintun, M.A.; Pontecorvo, M.J.; Hefti, F.; Carpenter, A.P.; Flitter, M.L.; et al. Use of florbetapir-PET for imaging beta-amyloid pathology. JAMA 2011, 305, 275–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, D.; Silva, E.J.; Munch, M.; Ronda, J.M.; Wang, W.; Duffy, J.F. Comparison of subjective and objective assessments of sleep in healthy older subjects without sleep complaints. J. Sleep Res. 2009, 18, 254–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Cases | SD Cases with Treatment | |||||
|---|---|---|---|---|---|---|
| Non-SD Cases | SD Cases | p-Value | Un-Recovered | Recovered | p-Value | |
| Case number (%) | 33 (34%) | 64 (66%) | 11 (17.2%) | 53 (82.8%) | ||
| Age (year) | 73 (66–81) | 73 (63–81) | n.s. | 73 (67–78) | 73 (63–81) | n.s. |
| Onset age (year) | 69 (63–79) | 71 (61–79) | n.s. | 69 (63–79) | 71 (61–79) | n.s. |
| Sex (Male/Female) | M18/F15 | M30/F34 | n.s. | M6/F5 | M24/F29 | n.s. |
| Disease length (month) | 32 (19–45) | 32 (16–59) | n.s. | 32 (19–45) | 32 (16–59) | n.s. |
| Secondary education | 4 (2–11) | 4 (0–11) | n.s. | 4 (2–11) | 4 (0–11) | n.s. |
| Body Mass Index | 23.7 (16.7–29.2) | 23.6 (15.48–33.02) | n.s. | 23.7 (16.7–29.2) | 24.5 (15.48–33.02) | n.s. |
| Correlation Pair | Pearson r | p-Value |
|---|---|---|
| Education vs. Onset age | −0.573 | 8.53 × 10−10 |
| PSQI vs. HAMA | 0.467 | 1.42 × 10−6 |
| PSQI vs. HRSD-24 | 0.353 | 0.0004 |
| PSQI vs. Aβ42/40 ratio | 0.348 | 0.0005 |
| PSQI vs. Tau-pT181 | 0.424 | 1.52 × 10−5 |
| HRSD-24 vs. HAMA | 0.419 | 1.93 × 10−5 |
| HRSD-24 vs. Aβ42/40 ratio | 0.506 | 1.24 × 10−7 |
| HRSD-24 vs. Tau-pT181 | 0.643 | 1.30 × 10−12 |
| HAMA vs. Aβ42/40 ratio | 0.506 | 1.28 × 10−7 |
| HAMA vs. Tau-pT181 | 0.555 | 3.61 × 10−9 |
| Aβ42/40 ratio vs. Tau-pT181 | 0.588 | 2.34 × 10−10 |
| Correlation Pair | Pearson r | p-Value |
|---|---|---|
| Education vs. Onset age | −0.709 | 5.53 × 10−11 |
| PSQI vs. HAMA | 0.488 | 4.22 × 10−4 |
| PSQI vs. HRSD-24 | 0.268 | 0.032 |
| PSQI vs. Aβ42/40 ratio | 0.311 | 0.012 |
| PSQI vs. Tau-pT181 | 0.328 | 0.008 |
| MoCa vs. GDS | −0.409 | 0.0008 |
| GDS vs. Aβ42/40 ratio | −0.316 | 0.011 |
| HRSD-24 vs. HAMA | 0.407 | 0.0008 |
| HRSD-24 vs. Aβ42/40 ratio | 0.580 | 4.96 × 10−7 |
| HRSD-24 vs. Tau-pT181 | 0.709 | 5.13 × 10−11 |
| HAMA vs. Aβ42/40 ratio | 0.526 | 7.98 × 10−6 |
| HAMA vs. Tau-pT181 | 0.663 | 2.43 × 10−9 |
| Aβ42/40 ratio vs. Tau-pT181 | 0.772 | 7.84 × 10−14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.; Li, M.; Zhang, M.; Qiu, J.; Cheng, H.; Mou, X.; Chen, Q.; Li, T.; Peng, J.; Li, B. Sleep Quality Improvement Enhances Neuropsychological Recovery and Reduces Blood Aβ42/40 Ratio in Patients with Mild–Moderate Cognitive Impairment. Medicina 2021, 57, 1366. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121366
Huang H, Li M, Zhang M, Qiu J, Cheng H, Mou X, Chen Q, Li T, Peng J, Li B. Sleep Quality Improvement Enhances Neuropsychological Recovery and Reduces Blood Aβ42/40 Ratio in Patients with Mild–Moderate Cognitive Impairment. Medicina. 2021; 57(12):1366. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121366
Chicago/Turabian StyleHuang, Haihua, Mingqiu Li, Menglin Zhang, Jiang Qiu, Haiyan Cheng, Xin Mou, Qinghong Chen, Tina Li, Jun Peng, and Benyi Li. 2021. "Sleep Quality Improvement Enhances Neuropsychological Recovery and Reduces Blood Aβ42/40 Ratio in Patients with Mild–Moderate Cognitive Impairment" Medicina 57, no. 12: 1366. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121366