
A New Criterion for Fluoroquinolone-Associated Disability Diagnosis: Functional Gastrointestinal Disorders


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. FDA Adverse Event Reporting System Data Collection
2.2. Study Participants
2.3. The Bowel Disease Questionnaire
2.4. Data Analysis
3. Results
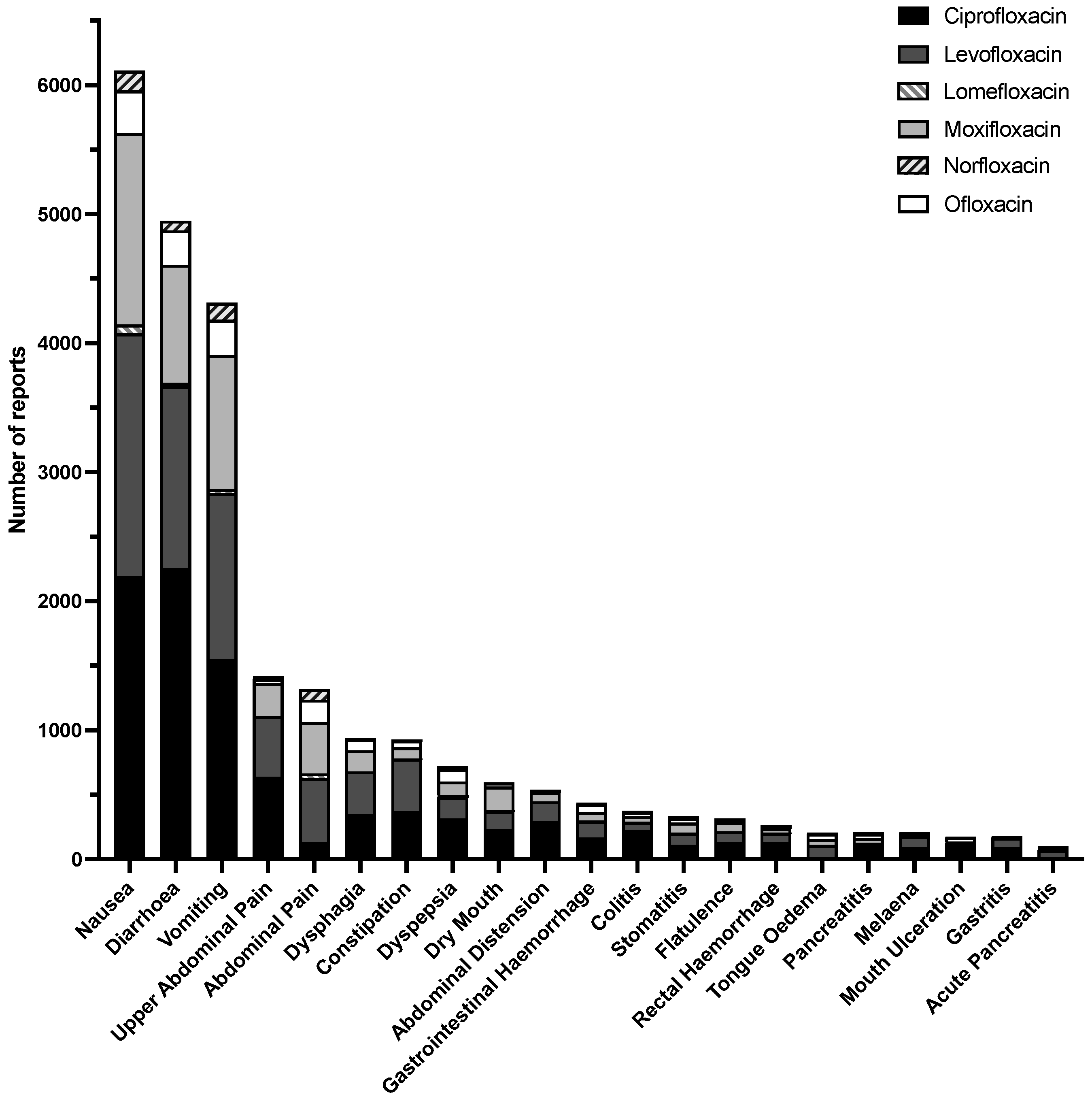
3.1. FAERS Reports on Gastrointestinal Disorders
3.2. Survey Responses
3.2.1. Upper and Lower Abdominal Issues
3.2.2. Bowel Habits
3.2.3. Nausea, Appetite, and Heartburn
3.2.4. Patient Scoring
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fluoroquinolones|A.R. & Patient Safety Portal. Available online: https://arpsp.cdc.gov/profile/antibiotic-use/fluoroquinolones (accessed on 25 August 2021).
- Aldred, K.J.; Kerns, R.J.; Osheroff, N. Mechanism of Quinolone Action and Resistance. Biochemistry 2014, 53, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Stahlmann, R.; Riecke, K. Well tolerated or risky? Adverse effect of quinolones. Pharm. Unserer Zeit 2001, 30, 412–417. [Google Scholar] [CrossRef]
- Chui, C.S.; Chan, E.W.Y.; Wong, A.Y.; Root, A.; Douglas, I.J.; Wong, I.C. Association between oral fluoroquinolones and seizures. Neurology 2016, 86, 1708–1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etminan, M.; Brophy, J.M.; Samii, A. Oral fluoroquinolone use and risk of peripheral neuropathy: A pharmacoepidemiologic study. Neurology 2014, 83, 1261–1263. [Google Scholar] [CrossRef]
- Lewis, T.; Cook, J. Fluoroquinolones and Tendinopathy: A Guide for Athletes and Sports Clinicians and a Systematic Review of the Literature. J. Athl. Train. 2014, 49, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, A.L.; Wu, W.; Cortes, D.; Rochon, P. Tendon Injury and Fluoroquinolone Use: A Systematic Review. Drug Saf. 2013, 36, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Yarrington, M.E.; Anderson, D.J.; Ashley, E.D.; Jones, T.; Davis, A.; Johnson, M.; Lokhnygina, Y.; Sexton, D.J.; Moehring, R.W. Impact of FDA black box warning on fluoroquinolone and alternative antibiotic use in southeastern US hospitals. Infect. Control. Hosp. Epidemiol. 2019, 40, 1297–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fluoroquinolone Safety Labeling Changes—FDA/CDER Drug Information Webinar. Available online: https://www.fda.gov/media/104060/download (accessed on 25 August 2021).
- Levaquin Citizen Petition. Available online: https://ewscripps.brightspotcdn.com/e7/36/d5778eb841b882edc9277eafd700/levaquin-citizens-petition.pdf (accessed on 25 August 2021).
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [Green Version]
- Kabbani, S.; Hersh, A.L.; Shapiro, D.J.; Fleming-Dutra, K.E.; Pavia, A.T.; Hicks, L.A. Opportunities to Improve Fluoroquinolone Prescribing in the United States for Adult Ambulatory Care Visits. Clin. Infect. Dis. 2018, 67, 134–136. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV. Gastroenterology 2016, 150, 1262–1279.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasricha, P.J. Neurogastroenterology: A Great Career Choice for Aspiring Gastroenterologists Thinking About the Future. Gastroenterology 2011, 140, 1126–1128.e1. [Google Scholar] [CrossRef]
- Clyburn, C.; Browning, K.N. Glutamatergic plasticity within neurocircuits of the dorsal vagal complex and the regulation of gastric functions. Am. J. Physiol. Liver Physiol. 2021, 320, G880–G887. [Google Scholar] [CrossRef]
- Stakenborg, N.; Giovangiulio, M.D.; Boeckxstaens, G.E.; Matteoli, G. The Versatile Role of The Vagus Nerve in The Gastrointestinal Tract. EMJ Gastroenterol. 2013, 9, 106–114. [Google Scholar]
- Altschuler, S.M.; Escardo, J.; Lynn, R.B.; Miselis, R.R. The central organization of the vagus nerve innervating the colon of the rat. Gastroenterology 1993, 104, 502–509. [Google Scholar] [CrossRef]
- Browning, K.N.; Travagli, R.A. Central Nervous System Control of Gastrointestinal Motility and Secretion and Modulation of Gastrointestinal Functions. Compr. Physiol. 2014, 4, 1339–1368. [Google Scholar] [CrossRef] [Green Version]
- Travagli, R.A.; Anselmi, L. Vagal neurocircuitry and its influence on gastric motility. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 389–401. [Google Scholar] [CrossRef] [Green Version]
- Fornai, M.; Antonioli, L.; Colucci, R.; Tuccori, M.; Blandizzi, C. Pathophysiology of gastric ulcer development and healing: Molecular mechanisms and novel therapeutic options. In Peptic Ulcer Disease; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2011. [Google Scholar] [CrossRef] [Green Version]
- Travagli, R.A.; Gillis, R.A.; Rossiter, C.D.; Vicini, S. Glutamate and GABA-mediated synaptic currents in neurons of the rat dorsal motor nucleus of the vagus. Am. J. Physiol. Liver Physiol. 1991, 260, G531–G536. [Google Scholar] [CrossRef]
- Gillis, R.A.; Dezfuli, G.; Bellusci, L.; Vicini, S.; Sahibzada, N. Brainstem Neuronal Circuitries Controlling Gastric Tonic and Phasic Contractions: A Review. Cell. Mol. Neurobiol. 2021, 1–28. [Google Scholar] [CrossRef]
- Herman, M.A.; Cruz, M.T.; Sahibzada, N.; Verbalis, J.; Gillis, R.A. GABA signaling in the nucleus tractus solitarius sets the level of activity in dorsal motor nucleus of the vagus cholinergic neurons in the vagovagal circuit. Am. J. Physiol. Liver Physiol. 2009, 296, G101–G111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, L.A.; Taylor, T.H.; Hunkler, R.J. U.S. Outpatient Antibiotic Prescribing. N. Engl. J. Med. 2013, 368, 1461–1462. [Google Scholar] [CrossRef]
- Domagala, J.M. Structure-activity and structure-side-effect relationships for the quinolone antibacterials. J. Antimicrob. Chemother. 1994, 33, 685–706. [Google Scholar] [CrossRef]
- Green, M.A.; Halliwell, R.F. Selective antagonism of the GABAA receptor by ciprofloxacin and biphenylacetic acid. Br. J. Pharmacol. 1997, 122, 584–590. [Google Scholar] [CrossRef] [Green Version]
- Ilgin, S.; Can, O.D.; Atli, O.; Üçel, U.I.; Şener, E.; Guven, I. Ciprofloxacin-induced neurotoxicity: Evaluation of possible underlying mechanisms. Toxicol. Mech. Methods 2015, 25, 374–381. [Google Scholar] [CrossRef]
- Davey, P.G.; Charter, M.; Kelly, S.; Varma, T.R.; Jacobson, I.; Freeman, A.; Precious, E.; Lambert, J. Ciprofloxacin and sparfloxacin penetration into human brain tissue and their activity as antagonists of GABAA receptor of rat vagus nerve. Antimicrob. Agents Chemother. 1994, 38, 1356–1362. [Google Scholar] [CrossRef] [Green Version]
- Kawai, Y.; Matsubayashi, K.; Hakusui, H. Interaction of Quinolones with Metal Cations in Aqueous Solution. Chem. Pharm. Bull. 1996, 44, 1425–1430. [Google Scholar] [CrossRef] [Green Version]
- Michalak, K.; Sobolewska-Włodarczyk, A.; Włodarczyk, M.; Sobolewska, J.; Wozniak, P.; Sobolewski, B. Treatment of the Fluoroquinolone-Associated Disability: The Pathobiochemical Implications. Oxidative Med. Cell. Longev. 2017, 2017, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Seedher, N.; Agarwal, P. Effect of metal ions on some pharmacologically relevant interactions involving fluoroquinolone antibiotics. Drug Metab. Drug Interact. 2010, 25, 17–24. [Google Scholar] [CrossRef]
- Ma, H.H.M.; Chiu, F.C.K.; Li, R.C. Mechanistic Investigation of the Reduction in Antimicrobial Activity of Ciprofloxacin by Metal Cations. Pharm. Res. 1997, 14, 366–370. [Google Scholar] [CrossRef]
- Koga, H. High-Performance Liquid Chromatography Measurement of Antimicrobial Concentrations in Polymor-phonuclear Leukocytes. Antimicrob. Agents Chemother. 1987, 31, 1904–1908. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.; García, I.; Ballesta, S.; Perea, E.J. Uptake and intracellular activity of trovafloxacin in human phagocytes and tissue-cultured epithelial cells. Antimicrob. Agents Chemother. 1997, 41, 274–277. [Google Scholar] [CrossRef] [Green Version]
- Andriole, V.T. The Quinolones, 3rd ed.; Academic Press: San Diego, CA, USA, 2000. [Google Scholar]
- De Sarro, G.; Nava, F.; Calapai, G.; De Sarro, A. Effects of Some Excitatory Amino Acid Antagonists and Drugs En-hancing Gamma-Aminobutyric Acid Neurotransmission on Pefloxacin-Induced Seizures in DBA/2 Mice. Antimicrob. Agents Chemother. 1997, 41, 427–434. [Google Scholar] [CrossRef] [Green Version]
- Moghimi, A.; Mollazadeh, S.; Rassouli, F.B.; Shiee, R.; Khalilzade, M.A. The Effect of Ciprofloxacin Injection on Ge-netically Absence Prone (Wag/Rij) Rat’s Electroencephalogram Characteristics. Basic Clin. Neurosci. 2013, 4, 31–35. [Google Scholar] [PubMed]
- CIPRO (Ciprofloxacin Hydrochloride)–FDA Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/019537s086lbl.pdf (accessed on 25 August 2021).
- LEVAQUIN© (Levofloxacin)—Label. Available online: https://www.fda.gov/files/drugs/published/Levaquin-Label.pdf (accessed on 25 August 2021).
- Talley, N.J.; Phillips, S.F.; Wiltgen, C.M.; Zinsmeister, A.R.; Melton, L.J. Assessment of Functional Gastrointestinal Disease: The Bowel Disease Questionnaire. Mayo Clin. Proc. 1990, 65, 1456–1479. [Google Scholar] [CrossRef] [Green Version]
- Keeney, K.M.; Yurist-Doutsch, S.; Arrieta, M.-C.; Finlay, B.B. Effects of Antibiotics on Human Microbiota and Subsequent Disease. Annu. Rev. Microbiol. 2014, 68, 217–235. [Google Scholar] [CrossRef]
- AVELOX (Moxifloxacin Hydrochloride). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/021085s063lbl.pdf (accessed on 1 October 2021).
- FLOXIN© (Ofloxacin Tablets)—Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/019735s059lbl.pdf (accessed on 25 August 2021).
- MAXAQUIN© (Lomefloxacin Hydrochloride Tablets)—Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/20013s015lbl.pdf (accessed on 25 August 2021).
- NOROXIN© (Norfloxacin)—Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/019384s066lbl.pdf (accessed on 25 August 2021).
- Alajbegovic, S.; Sanders, J.W.; Atherly, D.E.; Riddle, M.S. Effectiveness of rifaximin and fluoroquinolones in preventing travelers’ diarrhea (TD): A systematic review and meta-analysis. Syst. Rev. 2012, 1, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, W.; Heaton, K.W. Functional bowel disorders in apparently healthy people. Gastroenterology 1980, 79, 283–288. [Google Scholar] [CrossRef]
- Manning, A.P.; Thompson, W.G.; Heaton, K.W.; Morris, A.F. Towards positive diagnosis of the irritable bowel. BMJ 1978, 2, 653–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, W.G. Gastrointestinal symptoms in the irritable bowel compared with peptic ulcer and inflammatory bowel disease. Gut 1984, 25, 1089–1092. [Google Scholar] [CrossRef] [Green Version]
- Kruis, W.; Thieme, C.; Weinzierl, M.; Schüssler, P.; Holl, J.; Paulus, W. A diagnostic score for the irritable bowel syndrome. Gastroenterology 1984, 87, 1–7. [Google Scholar] [CrossRef]
- Muris, J.; Starmans, R.; Pop, P.; Crebolder, H.F.; Knottnerus, J.A. Discriminant value of symptoms in patients with dyspepsia. J. Fam. Pract. 1994, 38. [Google Scholar]
- Horrocks, J.C.; De Dombal, F.T. Clinical presentation of patients with "dyspepsia". Detailed symptomatic study of 360 patients. Gut 1978, 19, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drossman, D.A.; Sandler, R.S.; McKee, D.C.; Lovitz, A.J. Bowel patterns among subjects not seeking health care. Use of a questionnaire to identify a population with bowel dysfunction. Gastroenterology 1982, 83, 529–534. [Google Scholar] [CrossRef]
- Sandler, R.S.; Drossman, D.A.; Nathan, H.P.; McKee, D.C. Symptom complaints and health care seeking behavior in subjects with bowel dysfunction. Gastroenterology 1984, 87, 314–318. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional GI Disorders: What’s in a Name? Gastroenterology 2005, 128, 1771–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drossman, D.A. The Functional Gastrointestinal Disorders and the Rome III Process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Kommalapati, A.; Wallam, S.; Tella, S.H.; Qureshi, Z.P.; Bennett, C.L. Fluoroquinolone-associated suicide. Eur. J. Intern. Med. 2018, 55, e21–e22. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.C.; Bennett, C.L.; Witherspoon, B.; Knopf, K.B. An evaluation of reports of ciprofloxacin, levofloxacin, and moxifloxacin-association neuropsychiatric toxicities, long-term disability, and aortic aneurysms/dissections disseminated by the Food and Drug Administration and the European Medicines Agency. Expert Opin. Drug Saf. 2019, 18, 1055–1063. [Google Scholar] [CrossRef]
- Kandasamy, A.; Srinath, D. Levofloxacin-induced acute anxiety and insomnia. J. Neurosci. Rural. Pract. 2012, 3, 212–214. [Google Scholar] [CrossRef]
- Feinberg, S.S. Fluoroquinolone-induced depression. Am. J. Psychiatry 1995, 152, 954–955. [Google Scholar] [CrossRef] [PubMed]
- Egerbacher, M.; Seiberl, G.; Wolfesberger, B.; Walter, I. Ciprofloxacin causes cytoskeletal changes and detachment of human and rat chondrocytes in vitro. Arch. Toxicol. 2000, 73, 557–563. [Google Scholar] [CrossRef]
- Shakibaei, M.; Kociok, K.; Förster, C.; Vormann, J.; Günther, T.; Stahlmann, R.; Merker, H.-J. Comparative Evaluation of Ultrastructural Changes in Articular Cartilage of Ofioxacin-Treated and Magnesium-Deficient Immature Rats. Toxicol. Pathol. 1996, 24, 580–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egerbacher, M.; Wolfesberger, B.; Walter, I.; Seiberl, G. Integrins mediate the effects of quinolones and magnesium deficiency on cultured rat chondrocytes. Eur. J. Cell Biol. 1999, 78, 391–397. [Google Scholar] [CrossRef]
- Hsiao, C.-J.J.; Younis, H.; Boelsterli, U.A. Trovafloxacin, a fluoroquinolone antibiotic with hepatotoxic potential, causes mitochondrial peroxynitrite stress in a mouse model of underlying mitochondrial dysfunction. Chem. Interact. 2010, 188, 204–213. [Google Scholar] [CrossRef]
- Pouzaud, F.; Bernard-Beaubois, K.; Thevenin, M.; Warnet, J.-M.; Hayem, G.; Rat, P. In Vitro Discrimination of Fluoroquinolones Toxicity on Tendon Cells: Involvement of Oxidative Stress. J. Pharmacol. Exp. Ther. 2003, 308, 394–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, P.; Liu, R. Oxidative stress response of two fluoroquinolones with catalase and erythrocytes: A combined molecular and cellular study. J. Hazard. Mater. 2013, 252–253, 321–329. [Google Scholar] [CrossRef]
- Talla, V.; Veerareddy, P. Oxidative Stress Induced by Fluoroquinolones on Treatment for Complicated Urinary Tract Infections in Indian Patients. J. Young-Pharm. 2011, 3, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Kumbhar, G.B.; Khan, A.M.; Rampal, S. Evaluation of gatifloxacin for its potential to induce antioxidant imbalance and retinopathy in rabbits. Hum. Exp. Toxicol. 2014, 34, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Kaur, K.; Fayad, R.; Saxena, A.; Frizzell, N.; Chanda, A.; Das, S.; Chatterjee, S.; Hegde, S.; Baliga, M.S.; Ponemone, V.; et al. Fluoroquinolone-related neuropsychiatric and mitochondrial toxicity: A collaborative investigation by scientists and members of a social network. J. Community Support. Oncol. 2016, 14, 54–65. [Google Scholar] [CrossRef]
- Karakan, T.; Ozkul, C.; Akkol, E.K.; Bilici, S.; Sobarzo-Sánchez, E.; Capasso, R. Gut-Brain-Microbiota Axis: Antibiotics and Functional Gastrointestinal Disorders. Nutrients 2021, 13, 389. [Google Scholar] [CrossRef]
- Black, C.J.; Drossman, D.A.; Talley, N.J.; Ruddy, J.; Ford, A.C. Functional gastrointestinal disorders: Advances in understanding and management. Lancet 2020, 396, 1664–1674. [Google Scholar] [CrossRef]
- Nord, C. The effect of antimicrobial agents on the ecology of the human intestinal microflora. Veter. Microbiol. 1993, 35, 193–197. [Google Scholar] [CrossRef]
- Dethlefsen, L.; Relman, D.A. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc. Natl. Acad. Sci. USA 2010, 108, 4554–4561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donskey, C.J.; Hujer, A.M.; Das, S.M.; Pultz, N.J.; Bonomo, R.A.; Rice, L.B. Use of denaturing gradient gel electrophoresis for analysis of the stool microbiota of hospitalized patients. J. Microbiol. Methods 2003, 54, 249–256. [Google Scholar] [CrossRef]
- Nau, R.; Sörgel, F.; Eiffert, H. Penetration of Drugs through the Blood-Cerebrospinal Fluid/Blood-Brain Barrier for Treatment of Central Nervous System Infections. Clin. Microbiol. Rev. 2010, 23, 858–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Drug | Total Cases | Total Serious Cases | Total Death Cases | Total Gastro-Intestinal Cases |
|---|---|---|---|---|
| Cipro/CPX | 45,485 | 36,993 (81.33%) | 3193 (7.02%) | 9098 (20.00%) |
| Levaquin/LVX | 49,116 | 41,470 (84.43%) | 3124 (6.36%) | 7283 (14.82%) |
| Avelox/MFX | 20,705 | 14,558 (70.31%) | 1252 (6.05%) | 4347 (20%) |
| OFX | 10,003 | 7695 (76.93%) | 1493 (14.92%) | 1590 (15.89%) |
| NFX | 3022 | 2526 (83.59%) | 331 (10.95%) | 540 (17.86%) |
| LMX | 1500 | 1270 (84.67%) | 12 (0.8%) | 223 (14.86%) |
| Drug | GI Total Cases | GI Serious Cases | GI Disabled Cases | GI Death Cases |
|---|---|---|---|---|
| Cipro/CPX | 9098 | 7943 (87.30%) | 1181 (12.98%) | 649 (7.13%) |
| Levaquin/LVX | 7283 | 6438 (88.40%) | 778 (10.68%) | 569 (7.81%) |
| Avelox/MFX | 4347 | 3018 (69.43%) | 191 (4.39%) | 243 (5.59%) |
| OFX | 1590 | 1192 (74.97%) | 73 (4.59%) | 214 (13.46%) |
| NFX | 540 | 442 (81.85%) | 51 (9.44%) | 33 (6.11%) |
| LMX | 223 | 188 (84.30%) | 1 (0.45%) | 2 (0.9%) |
| Duration of Treatment | Dosage (mg) | Frequency (per Diem) | |||
|---|---|---|---|---|---|
| Response | n | Response | n | Response | n |
| Taken once only | 17 | 50 | 2 | Once | 85 |
| 2–5 days | 70 | 100 | 1 | Twice | 171 |
| 5–7 days | 42 | Between 200 and 300 | 16 | 3× | 20 |
| >7 days | 101 | Between 300 and 400 | 16 | 4× | 4 |
| >14 days | 33 | 500 | 153 | Unknown | 26 |
| >21 days | 12 | >500 | 22 | ||
| >1 month | 22 | Unknown | 94 | ||
| Unknown | 9 | FQ not in pill form | 2 | ||
| Irritable Bowel Syndrome | Functional Dyspepsia | Bowel Habits | Pain | |||||
|---|---|---|---|---|---|---|---|---|
| Drug | R2 Value | Drug | R2 Value | Drug | R2 Value | Drug | R2 Value | |
| Dosage | CPX | 0.00002 | CPX | 0.0008 | CPX | 0.0006 | CPX | 0.008 |
| LVX | 0.03 | LVX | 0.03 | LVX | 0.01 | LVX | 0.03 | |
| Other | 0 | Other | 0.04 | Other | 0.27 | Other | 0.06 | |
| Combo | 0.016 | Combo | 0.005 | Combo | 0.006 | Combo | 0.001 | |
| Duration of treatment | CPX | 0.02 | CPX | 0.07 | CPX | 0.04 | CPX | 0.04 |
| LVX | 0.05 | LVX | 0.11 | LVX | 0.04 | LVX | 0.1 | |
| Other | 0.07 | Other | 0.28 | Other | 0.14 | Other | 0.28 | |
| Combo | 0.006 | Combo | 0.003 | Combo | 0.01 | Combo | 0.0003 | |
| Frequency per diem | CPX | 0.001 | CPX | 0.0001 | CPX | 0.006 | CPX | 0.0003 |
| LVX | 0.02 | LVX | 0.04 | LVX | 0.01 | LVX | 0.03 | |
| Other | 0.006 | Other | 0.17 | Other | 0.04 | Other | 0.15 | |
| Combo | 0.002 | Combo | 0.001 | Combo | 0.006 | Combo | 0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cannizzaro, D.N.; Naughton, L.F.; Freeman, M.Z.; Martin, L.; Bennett, C.L.; Bove, C. A New Criterion for Fluoroquinolone-Associated Disability Diagnosis: Functional Gastrointestinal Disorders. Medicina 2021, 57, 1371. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121371
Cannizzaro DN, Naughton LF, Freeman MZ, Martin L, Bennett CL, Bove C. A New Criterion for Fluoroquinolone-Associated Disability Diagnosis: Functional Gastrointestinal Disorders. Medicina. 2021; 57(12):1371. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121371
Chicago/Turabian StyleCannizzaro, Deanna N., Lydia F. Naughton, Maya Z. Freeman, Linda Martin, Charles L. Bennett, and Cecilia Bove. 2021. "A New Criterion for Fluoroquinolone-Associated Disability Diagnosis: Functional Gastrointestinal Disorders" Medicina 57, no. 12: 1371. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121371