
Deep Learning and Device-Assisted Enteroscopy: Automatic Detection of Gastrointestinal Angioectasia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
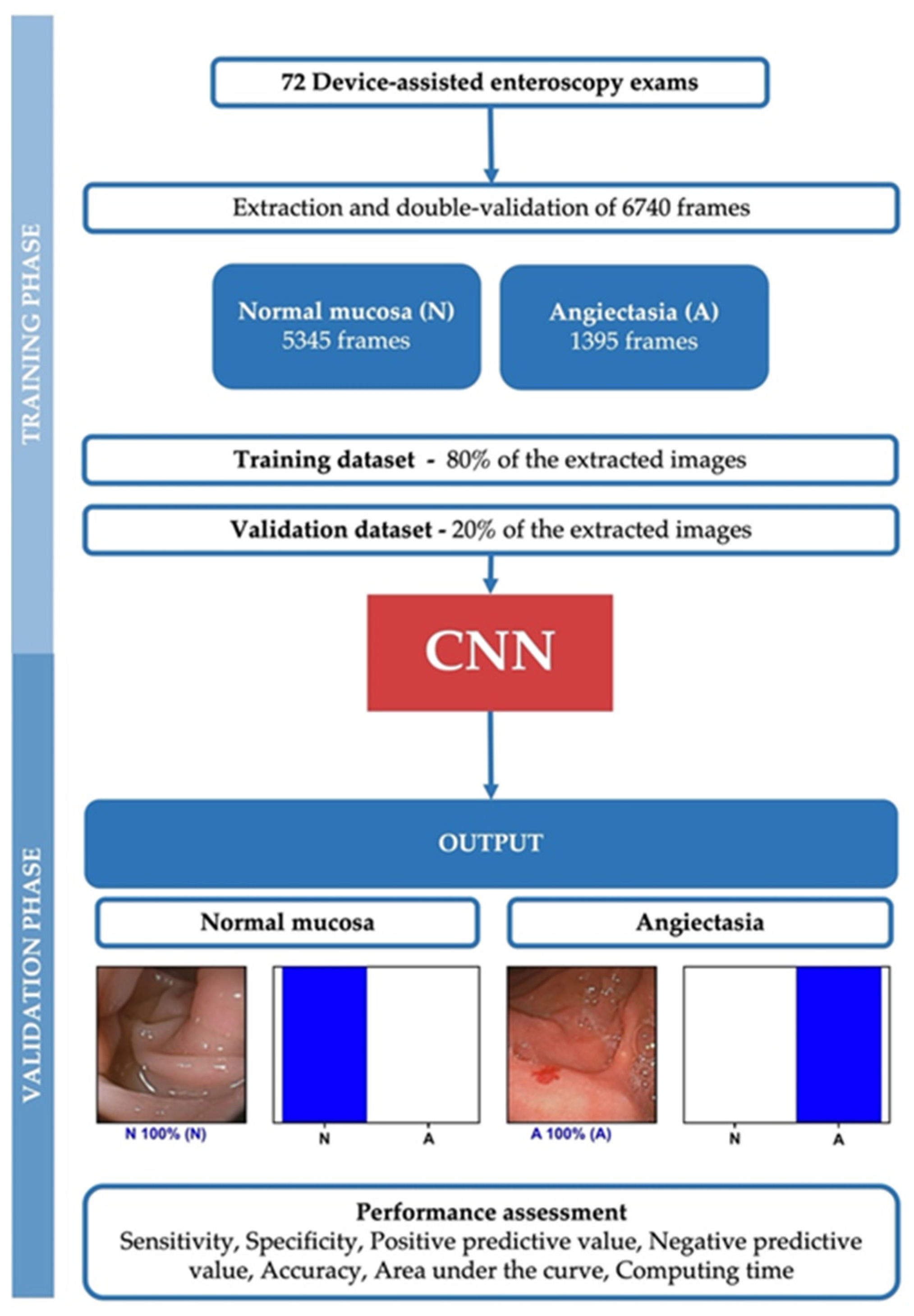
2.1. Study Design
2.2. Device-Assisted Enteroscopy Procedure, Data Collection and Definition
2.3. Development of the CNN
2.4. Model Performance and Statistical Analysis
3. Results
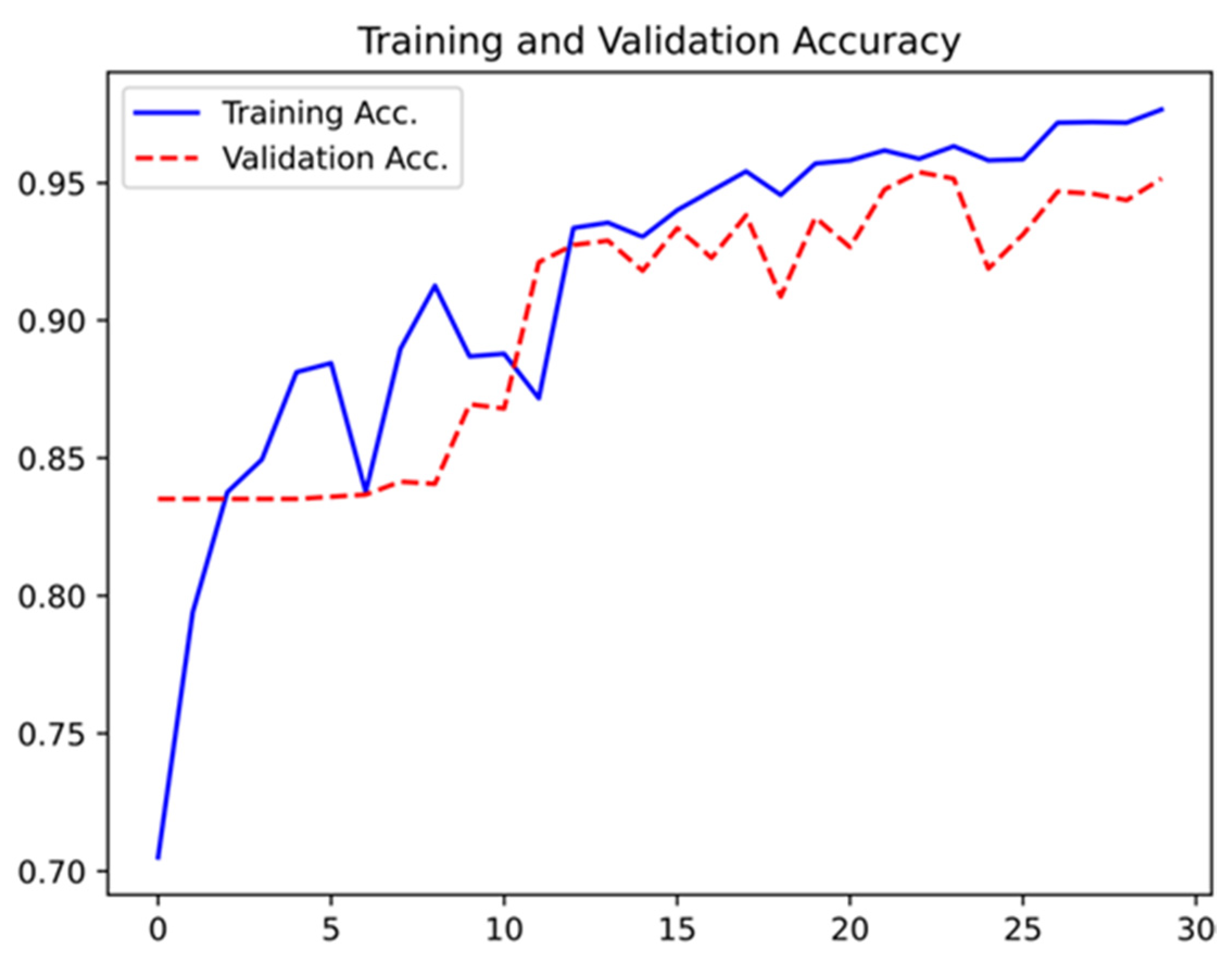
3.1. Construction of the Network
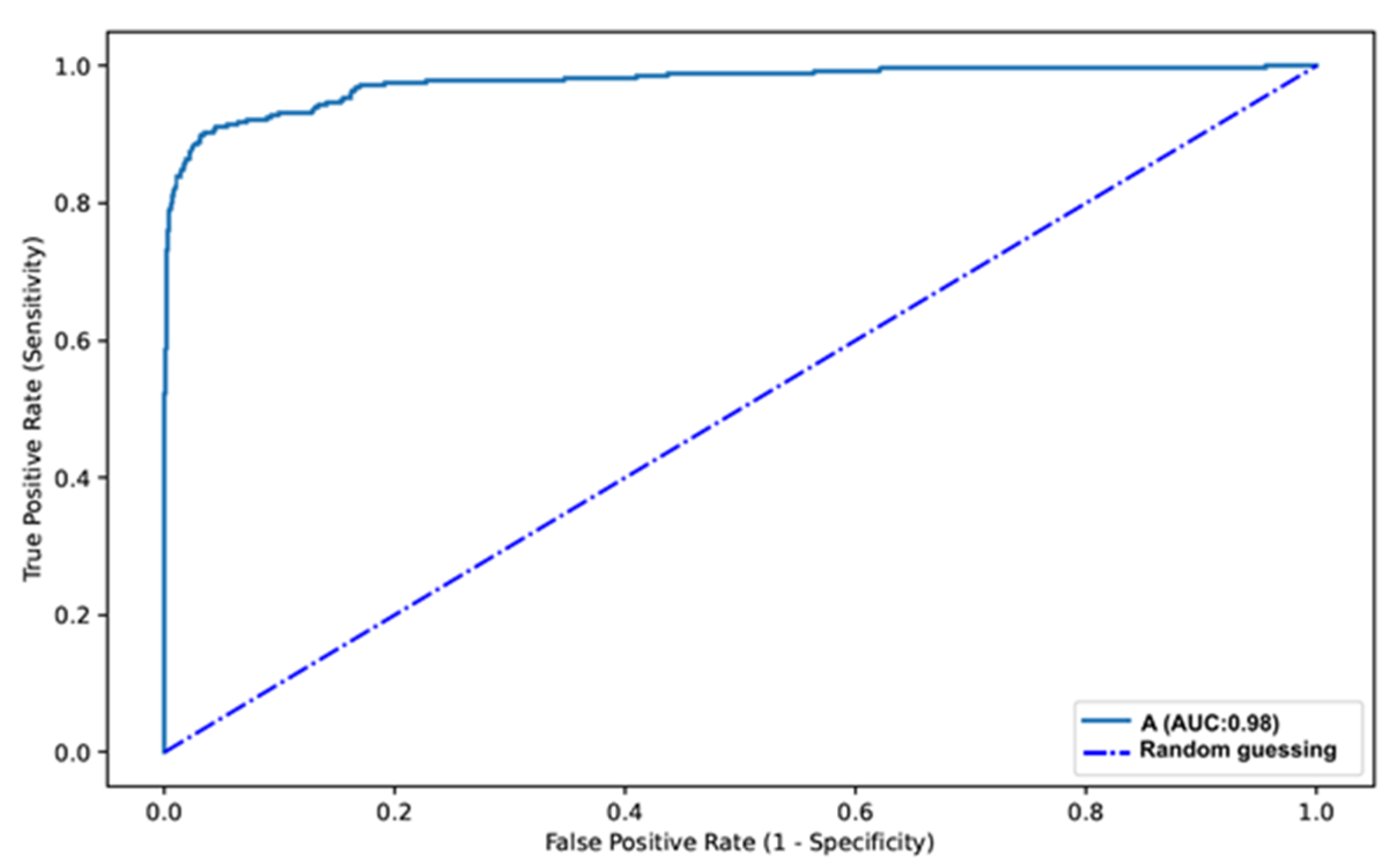
3.2. Overall Performance of the Network
3.3. Computational Performance of the CNN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heine, G.D.; Hadithi, M.; Groenen, M.J.; Kuipers, E.J.; Jacobs, M.A.; Mulder, C.J. Double-Balloon Enteroscopy: Indications, Diagnostic Yield, and Complications in a Series of 275 Patients with Suspected Small-Bowel Disease. Endoscopy 2006, 38, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Ohmiya, N.; Yano, T.; Yamamoto, H.; Arakawa, D.; Nakamura, M.; Honda, W.; Itoh, A.; Hirooka, Y.; Niwa, Y.; Maeda, O.; et al. Diagnosis and treatment of obscure GI bleeding at double balloon endoscopy. Gastrointest. Endosc. 2007, 66, S72–S77. [Google Scholar] [CrossRef]
- Gerson, L.B.; Fidler, J.L.; Cave, D.R.; A Leighton, J. ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding. Am. J. Gastroenterol. 2015, 110, 1265–1287. [Google Scholar] [CrossRef] [PubMed]
- Gurudu, S.R.; Bruining, D.H.; Acosta, R.D.; Eloubeidi, M.A.; Faulx, A.L.; Khashab, M.A.; Kothari, S.; Lightdale, J.R.; Muthusamy, V.R.; Yang, J.; et al. The role of endoscopy in the management of suspected small-bowel bleeding. Gastrointest. Endosc. 2017, 85, 22–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teshima, C.W.; Kuipers, E.J.; van Zanten, S.V.; Mensink, P. Double balloon enteroscopy and capsule endoscopy for obscure gas-trointestinal bleeding: An updated meta-analysis. J. Gastroenterol. Hepatol. 2011, 26, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Rajan, E.; Cheng, S.; Shen, R.; Zhang, C.; Zhang, S.; Wu, Y.; Zhong, J. Diagnostic Yield and Therapeutic Impact of Double-Balloon Enteroscopy in a Large Cohort of Patients with Obscure Gastrointestinal Bleeding. Am. J. Gastroenterol. 2006, 101, 2011–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasha, S.F.; Leighton, J.A.; Das, A.; Harrison, M.E.; Decker, G.A.; Fleischer, D.E.; Sharma, V.K. Double-Balloon Enteroscopy and Capsule Endoscopy Have Comparable Diagnostic Yield in Small-Bowel Disease: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2008, 6, 671–676. [Google Scholar] [CrossRef]
- Fry, L.C.; Bellutti, M.; Neumann, H.; Malfertheiner, P.; Mönkemüller, K. Incidence of bleeding lesions within reach of conventional upper and lower endoscopes in patients undergoing double-balloon enteroscopy for obscure gastrointestinal bleeding. Aliment. Pharmacol. Ther. 2009, 29, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, R.; Requa, J.; Dao, T.; Ninh, A.; Tran, E.; Mai, D.; Lugo, M.; Chehade, N.E.-H.; Chang, K.J.; Karnes, W.; et al. Artificial intelligence using convolutional neural networks for real-time detection of early esophageal neoplasia in Barrett’s esophagus (with video). Gastrointest. Endosc. 2020, 91, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Săftoiu, A.; Vilmann, P.; Dietrich, C.F.; Iglesias-Garcia, J.; Hocke, M.; Seicean, A.; Ignee, A.; Hassan, H.; Streba, C.T.; Ioncică, A.M.; et al. Quantitative contrast-enhanced harmonic EUS in differential diagnosis of focal pancreatic masses (with videos). Gastrointest. Endosc. 2015, 82, 59–69. [Google Scholar] [CrossRef]
- Sousa Ferreira, J.P.; da Quinta e Costa de Mascarenhas Saraiva, M.J.; Lima Afonso, J.M.; Carneiro Ribeiro, T.F.; Casal Cardoso, H.M.; Ribeiro Andrade, A.P.; Lages Parente, M.P.; Jorge, R.N.; Lopes, S.I.O.; de Macedo, G.M.G.; et al. Identification of Ulcers and Erosions by the Novel Pillcam™ Crohn’s Capsule Using a Convolutional Neural Network: A Multicentre Pilot Study. J. Crohns Colitis 2021, jjab117. [Google Scholar] [CrossRef]
- Rodriguez-Diaz, E.; Baffy, G.; Lo, W.-K.; Mashimo, H.; Vidyarthi, G.; Mohapatra, S.S.; Singh, S.K. Real-time artificial intelligence-based histologic classification of colorectal polyps with augmented visualization. Gastrointest. Endosc. 2021, 93, 662–670. [Google Scholar] [CrossRef]
- Guimarães, P.; Keller, A.; Fehlmann, T.; Lammert, F.; Casper, M. Deep learning-based detection of eosinophilic esophagitis. Endoscopy 2021. [Google Scholar] [CrossRef]
- Grooteman, K.V.; Holleran, G.; Matheeuwsen, M.; Van Geenen, E.J.M.; McNamara, D.; Drenth, J.P.H. A Risk Assessment of Factors for the Presence of Angiodysplasias During Endoscopy and Factors Contributing to Symptomatic Bleeding and Rebleeds. Dig. Dis. Sci. 2019, 64, 2923–2932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraiva, M.M.; Ribeiro, T.; Ferreira, J.P.; Boas, F.V.; Afonso, J.; Santos, A.L.; Parente, M.P.; Jorge, R.N.; Pereira, P.; Macedo, G. Artificial intelligence for automatic diagnosis of biliary stricture malignancy status in single-operator cholangioscopy: A pilot study. Gastrointest. Endosc. 2021. [Google Scholar] [CrossRef]
- Ponte, A.; Robles, E.P.-C.; Pinho, R.; Rodrigues, A.; Delgado, P.E.; Silva, J.; Rodrigues, J.; Carvalho, J.; Martínez, E.P.-C. High short-term rebleeding rate in patients undergoing a second endoscopic therapy for small-bowel angioectasias after recurrent bleeding. Rev. Española Enferm. Dig. 2017, 110, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Rahmi, G.; Samaha, E.; Vahedi, K.; Delvaux, M.; Gay, G.; Lamouliatte, H.; Filoche, B.; Saurin, J.; Ponchon, T.; Le Rhun, M.; et al. Long-term follow-up of patients undergoing capsule and double-balloon enter-oscopy for identification and treatment of small-bowel vascular lesions: A prospective, multicenter study. Endoscopy 2014, 46, 591–597. [Google Scholar]
- Samaha, E.; Rahmi, G.; Landi, B.; Lorenceau-Savale, C.; Malamut, G.; Canard, J.-M.; Bloch, F.; Jian, R.; Chatellier, G.; Cellier, C. Long-Term Outcome of Patients Treated with Double Balloon Enteroscopy for Small Bowel Vascular Lesions. Am. J. Gastroenterol. 2012, 107, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Gomes, C.; Mateos, J.M.R.; Pinho, R.T.; Ponte, A.; Rodrigues, A.; Gayosso, M.F.; Delgado, P.E.; Silva, J.C.; Afecto, E.; Carvalho, J. The rebleeding rate in patients evaluated for obscure gastrointestinal bleeding after negative small bowel findings by device assisted enteroscopy. Rev. Española Enferm. Dig. 2020, 112, 262–268. [Google Scholar] [CrossRef]
- Shinozaki, S.; Yano, T.; Sakamoto, H.; Sunada, K.; Hayashi, Y.; Sato, H.; Lefor, A.K.; Yamamoto, H. Long-Term Outcomes in Patients with Overt Obscure Gastrointestinal Bleeding After Negative Double-Balloon Endoscopy. Dig. Dis. Sci. 2015, 60, 3691–3696. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Badalamenti, M.; Maselli, R.; Correale, L.; Radaelli, F.; Rondonotti, E.; Ferrara, E.; Spadaccini, M.; Alkandari, A.; Fugazza, A.; et al. Efficacy of Real-Time Computer-Aided Detection of Colorectal Neoplasia in a Randomized Trial. Gastroenterology 2020, 159, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Wang, J.; Han, Z.; Yu, Y.; Chen, Z.; Huang, F.; Xu, Y.; Cai, J.; Zhang, Q.; Qiao, W.; et al. Artificial intelligence−enhanced white-light colonoscopy with attention guidance predicts colorectal cancer invasion depth. Gastrointest. Endosc. 2021, 94, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Zhou, W.; Wu, L.; Zhang, J.; Wang, J.; Mu, G.; Huang, X.; Li, Y.; Yuan, J.; Zeng, Z.; et al. Artificial intelligence in the diagnosis of gastric precancerous conditions by image-enhanced endoscopy: A multicenter, diagnostic study (with video). Gastrointest. Endosc. 2021, 94, 540–548. [Google Scholar] [CrossRef] [PubMed]
- FDA News Release: FDA Authorizes Marketing of First Device that Uses Artificial Intelligence to Help Detect Potential Signs of Colon Cancer. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-device-uses-artificial-intelligence-help-detect-potential-signs-colon (accessed on 5 October 2021).
- Noya, F.; Alvarez-Gonzalez, M.A.; Benitez, R. Automated angiodysplasia detection from wireless capsule endoscopy. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; IEEE: Manhattan, NY, USA, 2017; Volume 2017, pp. 3158–3161. [Google Scholar]
- Leenhardt, R.; Vasseur, P.; Philippe, M.; Saurin, J.C.; Rahmi, G.; Cholet, F.; Becq, A.; Marteau, P.; Histace, A.; Dray, X.; et al. A neural network algorithm for detection of GI angiectasia during small-bowel capsule endoscopy. Gastrointest. Endosc. 2019, 89, 189–194. [Google Scholar] [CrossRef]
- Tsuboi, A.; Oka, S.; Aoyama, K.; Saito, H.; Aoki, T.; Yamada, A.; Matsuda, T.; Fujishiro, M.; Ishihara, S.; Nakahori, M.; et al. Artificial intelligence using a convolutional neural network for automatic detection of small-bowel angioectasia in capsule endoscopy images. Dig. Endosc. 2020, 32, 382–390. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Final Diagnosis | |||
|---|---|---|---|
| Angioectasia | Normal Mucosa | ||
| CNN | Angioectasia | 247 | 31 |
| Normal mucosa | 32 | 1038 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mascarenhas Saraiva, M.; Ribeiro, T.; Afonso, J.; Andrade, P.; Cardoso, P.; Ferreira, J.; Cardoso, H.; Macedo, G. Deep Learning and Device-Assisted Enteroscopy: Automatic Detection of Gastrointestinal Angioectasia. Medicina 2021, 57, 1378. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121378
Mascarenhas Saraiva M, Ribeiro T, Afonso J, Andrade P, Cardoso P, Ferreira J, Cardoso H, Macedo G. Deep Learning and Device-Assisted Enteroscopy: Automatic Detection of Gastrointestinal Angioectasia. Medicina. 2021; 57(12):1378. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121378
Chicago/Turabian StyleMascarenhas Saraiva, Miguel, Tiago Ribeiro, João Afonso, Patrícia Andrade, Pedro Cardoso, João Ferreira, Hélder Cardoso, and Guilherme Macedo. 2021. "Deep Learning and Device-Assisted Enteroscopy: Automatic Detection of Gastrointestinal Angioectasia" Medicina 57, no. 12: 1378. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121378