
Renal Morphology in Coronavirus Disease: A Literature Review

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Pathogenesis
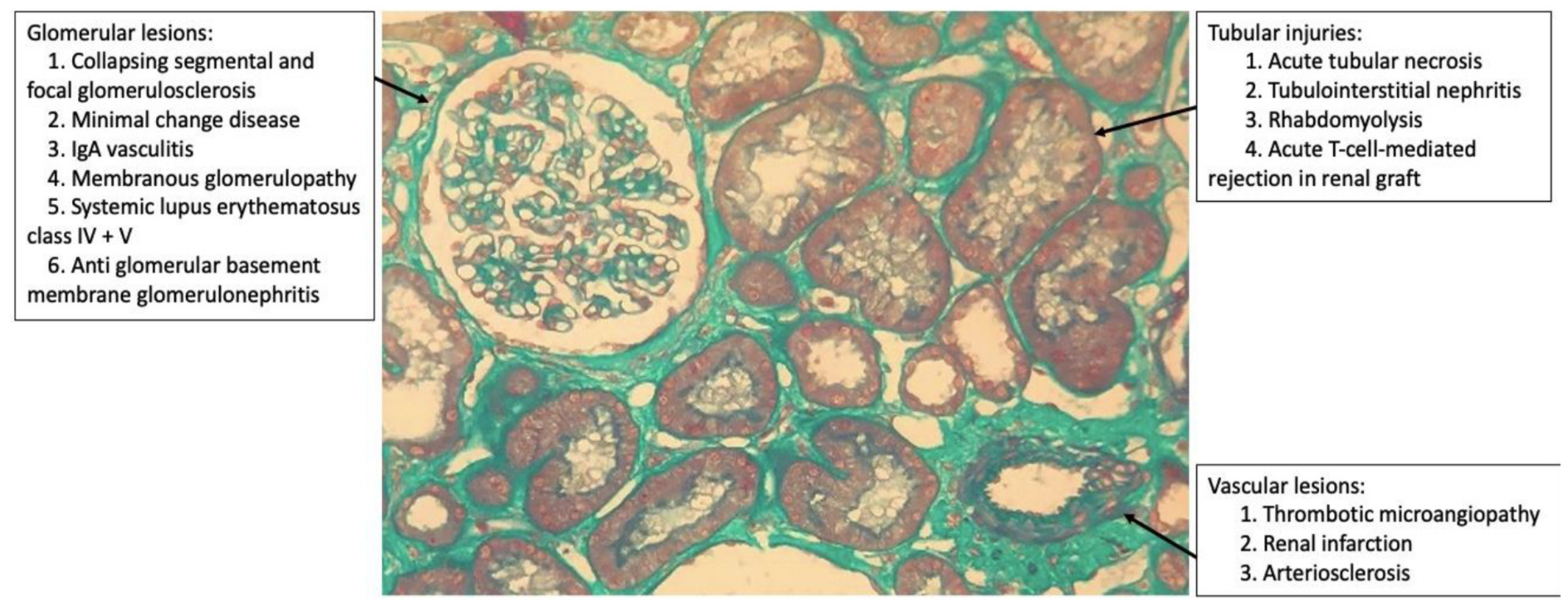
3. Morphological Kidney Findings in COVID-19
3.1. Glomerular Injury
3.2. Tubular Injury
3.3. Vascular Injury
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE-2 | Angiotensin-converter enzyme receptor 2 |
| AKI | Acute kidney injury |
| AIN | Acute interstitial nephritis |
| APOL1 (G1/G2) | Apolipoprotein L1 (genotype 1 e 2) |
| ARDS | Acute respiratory distress syndrome |
| anti-GBM | Antiglomerular basement membrane glomerulonephritis |
| cFSGS | Collapsing focal segmental glomerulosclerosis |
| COVAN | COVID-19-associated nephropathy |
| COVID-19 | Coronavirus disease 2019 |
| HIV | Human immunodeficiency virus |
| HIVAN | HIV-associated nephropathy |
| HLA | Human leukocyte antigen |
| IgA | Immunoglobulin A |
| MCD | Minimal change disease |
| MG | Membranous glomerulopathy |
| PLA2R | Phospholipase A2 174 receptor |
| RNA | Ribonucleic acid |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SLE | Systemic lupus erythematosus |
| TMPRSS2 | Transmembrane serine protease 2 |
References
- Sharma, Y.; Nasr, S.H.; Larsen, C.P.; Kemper, A.; Ormsby, A.H.; Williamson, S.R. COVID-19-Associated Collapsing Focal Segmental Glomerulosclerosis: A Report of 2 Cases. Kidney Med. 2020, 2, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Yang, M.; Wan, C.; Yi, L.X.; Tang, F.; Zhu, H.Y.; Yi, F.; Yang, H.C.; Fogo, A.B.; Nie, X.; et al. Renal Histopathological Analysis of 26 Postmortem Findings of Patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.E.; Brealey, J.K. Visualization of Putative Coronavirus in Kidney. Kidney Int. 2020, 98, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S.; et al. Multiorgan and Renal Tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Feng, Z.; Wang, C.; Wang, H.; Liu, L.; Wang, C.; Wang, R.; Liu, Y.; Liu, Y.; Wang, G.; et al. Human Kidney Is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. medRxiv 2020, preprint. [Google Scholar] [CrossRef] [Green Version]
- Larsen, C.P.; Bourne, T.D.; Wilson, J.D.; Saqqa, O.; Sharshir, M.A. Collapsing Glomerulopathy in a Patient with COVID-19. Kidney Int. Rep. 2020, 5, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Couturier, A.; Ferlicot, S.; Chevalier, K.; Guillet, M.; Essig, M.; Jauréguiberry, S.; Collarino, R.; Dargelos, M.; Michaut, A.; Geri, G.; et al. Indirect Effects of Severe Acute Respiratory Syndrome Coronavirus 2 on the Kidney in Coronavirus Disease Patients. Clin. Kidney J. 2020, 13, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; et al. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef] [PubMed]
- Peleg, Y.; Kudose, S.; D’Agati, V.; Siddall, E.; Ahmad, S.; Kisselev, S.; Gharavi, A.; Canetta, P. Acute Kidney Injury Due to Collapsing Glomerulopathy Following COVID-19 Infection. Kidney Int. Rep. 2020, 5, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, F.; Ismael, S.; Sannier, A.; Tarhini, H.; Volpe, T.; Greze, C.; Verpont, M.C.; Zouhry, I.; Rioux, C.; Lescure, F.X.; et al. Tubuloreticular Inclusions in COVID-19-related Collapsing Glomerulopathy. Kidney Int. 2020, 98, 241. [Google Scholar] [CrossRef] [PubMed]
- Magoon, S.; Bichu, P.; Malhotra, V.; Alhashimi, F.; Hu, Y.; Khanna, S.; Berhanu, K. COVID-19-Related Glomerulopathy: A Report of 2 Cases of Collapsing Focal Segmental Glomerulosclerosis. Kidney Med. 2020, 2, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Lazareth, H.; Péré, H.; Binois, Y.; Chabannes, M.; Schurder, J.; Bruneau, T.; Karras, A.; Thervet, E.; Rabant, M.; Veyer, D.; et al. COVID-19-Related Collapsing Glomerulopathy in a Kidney Transplant Recipient. Am. J. Kidney Dis. 2020, S0272–6386, 30790–30793. [Google Scholar] [CrossRef]
- Wu, H.; Larsen, C.P.; Hernandez-Arroyo, C.F.; Mohamed, M.M.B.; Caza, T.; Sharshir, M.; Chughtai, A.; Xie, L.; Gimenez, J.M.; Sandow, T.A.; et al. AKI and Collapsing Glomerulopathy Associated with COVID-19 and APOL1 High-Risk Genotype. J. Am. Soc. Nephrol. 2020, 31, 1688–1695. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Bhargava, R.; Shaukat, A.A.; Albert, E.; Leggat, J. Spectrum of Podocytopathies in New-Onset Nephrotic Syndrome Following COVID-19 Disease: A Report of 2 Cases. BMC Nephrol. 2020, 21, 326. [Google Scholar] [CrossRef] [PubMed]
- Kadosh, B.S.; Pavone, J.; Wu, M.; Reyentovich, A.; Gidea, C. Collapsing Glomerulopathy Associated with COVID-19 Infection in a Heart Transplant Recipient. J. Heart Lung Transplant. 2020, 39, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Noble, R.; Tan, M.Y.; McCulloch, T.; Shantier, M.; Byrne, C.; Hall, M.; Jesky, M. Collapsing Glomerulopathy Affecting Native and Transplant Kidneys in Individuals with COVID-19. Nephron 2020, 144, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Kissling, S.; Rotman, S.; Gerber, C.; Halfon, M.; Lamoth, F.; Comte, D.; Lhopitallier, L.; Sadallah, S.; Fakhouri, F. Collapsing Glomerulopathy in a COVID-19 Patient. Kidney Int. 2020, 98, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Vardhana, S.A.; Wolchok, J.D. The Many Faces of the Anti-COVID Immune Response. J. Exp. Med. 2020, 217, e20200678. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.A.L., Jr.; de Menezes Neves, P.D.M.; Lages, J.S.; de Araújo Cunha, K.; Muniz, M.P.R.; de Araújo Brito, D.J.; Watanabe, A.; Watanabe, E.H.; Onuchic, L.F.; Nunes, L.L.A.; et al. Brazilian consortium for the study on renal diseases associated with COVID-19: A multicentric effort to understand SARS-CoV-2-related nephropathy. Front. Med. 2020, 7, 584235. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case | Sex | Age(y) | Race | Comorbidities | Alb (g/dL) | PTN (g) | Hm | Cr Baseline (mg/dL) | Cr at RB (mg/dL) | HD | Follow-Up | Ref |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 47 | AA | HTN, DLP, OSAS, DM2, GERD | 4.0 | 3.3 | N | 1.0 | 8.27 | Y | HD | Sharma [1] 1 |
| 2 | M | 49 | AA | HTN, CI, PAOD, arthritis | 3.1 | 2.6 | N | 0.95 | 10.1 | Y | HD | Sharma [1] 2 |
| 3 | F | 44 | AA | HTN, DM2, CKD, DLP | 2.5 | 25.0 | Y | 1.4 | 11.0 | Y | HD | Larsen [6] |
| 4 | M | 53 | AA | HTN, CI | 1.3 | 16.5 | N | 1.02 | 2.19 | N | CT | Couturier [7] 1 |
| 5 | M | 53 | AA | HTN, HBV | 2.2 | 2.65 | N | 1.35 | 5.98 | N | CT | Couturier [7] 2 |
| 6 | M | 46 | AA | Obese, OSAS | 3.1 | 5.8 | N | 1.1 | 12.5 | Y | HD | Kudose [8] 1 |
| 7 | M | 62 | AA | HTN, prostate carcinoma | 3.1 | 12.1 | N | 2.0 | 10.7 | N | CT | Kudose [8] 2 |
| 8 | M | 62 | AA | HTN, prostate carcinoma, DM2 | 2.4 | 19.0 | N | 1.0 | 11.6 | N | CT | Kudose [8] 3 |
| 9 | M | 57 | AA | HTN, HCV | 2.5 | 6.2 | N | 1.1 | 4.9 | N | CT | Kudose [8] 4 |
| 10 | M | 61 | AA | HTN, Obese | 2.5 | 9.0 | N | Normal | 15.0 | Y | HD | Kudose [8] 5 |
| 11 | M | 46 | AA | Obese, OSAS | 2.9 | 5.8 | Y | 1.1 | 19.9 | Y | HD | Peleg [9] |
| 12 | M | 79 | AA | Stroke, MGUS, CKD III, HTN | 2.9 | 11.4 | N | N/A | 2,5 | Y | HD | Gailard [10] |
| 13 | F | 28 | AA | Asthma | 1.6 | 2.0 | N | 0.99 | >6.5 | Y | CT | Magoon [11]1 |
| 14 | M | 56 | AA | HTN, CKD | 0.8 | 21.0 | N | 2.0 | 7.72 | Y | CT | Magoon [11]2 |
| 15 | M | 29 | AA | CKD (urinary schistosomiasis), kidney transplant, cell rejection | 2.8 | 4.3 | N | 2.0 | 6.04 | N | CT | Lazareth [12] |
| 16 | M | 63 | AA | N/A | 2.1 | 12.7 | N | 1.3 | 4.9 | Y | HD | Wu [13] 1 |
| 17 | F | 64 | AA | N/A | 2.4 | 4.6 | N | 1.5 | 4.2 | N | CT | Wu [13] 2 |
| 18 | F | 65 | AA | N/A | 2.6 | 13.6 | N | 1.3 | 2.9 | Y | HD Death | Wu [13] 3 |
| 19 | M | 44 | AA | N/A | 2.5 | 25.0 | Y | 1.4 | 11.4 | Y | HD | Wu [13] 4 |
| 20 | M | 37 | AA | N/A | 3.0 | N/A | N | 1.0 | 9.0 | Y | HD Death | Wu [13] 5 |
| 21 | M | 56 | AA | N/A | 2.9 | 3.6 | Y | 1.2 | 6.7 | Y | CT | Wu [13] 6 |
| 22 | M | 71 | AS | HTN, DM2, BPH | 2.0 | 18.5 | N | 1.19 | 4.49 | Y | HD | Gupta [14] 1 |
| 23 | M | 54 | AA | HTN. DM2, former smoker | 1.6 | 16.0 | N | 1.29 | 4.67 | N | CT | Gupta [14] 2 |
| 24 | M | 56 | AA | CI, cardiac transplant, CKD | N/A | 7.4 | N | 1.86 | 7.78 | N | CT | Kadosh [15] |
| 25 | M | 54 | AA | HTN, Obese, CKD | N/A | 3.2 | Y | 1.41 | 13.6 | Y | CT | Noble [16] 1 |
| 26 | M | 45 | AA | DM2,Obese, CKD, HTN, kidney transplant | N/A | 1.9 | Y | 3.2 | 14.05 | Y | HD | Noble [16] 2 |
| 27 | M | 63 | AA | HTN | 2.3 | 5.0 | N | 1.2 | 8.4 | N | CT | Kissling [17] |
| Case | APOL1 | ATI | TIN | IFTA | VS | TRI | VP | vRNA | Ref |
|---|---|---|---|---|---|---|---|---|---|
| 1 | G1/G2 | Diffuse | N/A | Mild | N/A | Y | N | N | Sharma [1] 1 |
| 2 | G1/G2 | Diffuse | Mild | N/A | N/A | Y | N | N | Sharma [1] 2 |
| 3 | G1/G1 | Important | Present | Moderate | N/A | Y | N | N | Larsen [6] |
| 4 | G1/G1 | N/A | N/A | Mild | N/A | N/A | N/A | N | Couturier [7] 1 |
| 5 | G1/G2 | Present | Present | Mild | Present | N/A | N/A | N | Couturier [7] 2 |
| 6 | Note 1 | Present | Focal | Mild | Mild | N/A | N | N | Kudose [8] 1 |
| 7 | Note 1 | Present | Focal | Moderate | Moderate to severe | Y | N | N | Kudose [8] 2 |
| 8 | Note 1 | Present | N/A | Moderate | Moderate | N | N | N | Kudose [8] 3 |
| 9 | Note 1 | Present | Focal | Severe | Mild | N/A | N/A | N | Kudose [8] 4 |
| 10 | Note 1 | Present | Focal | Severe | Mild to moderate | N | N | N | Kudose [8] 5 |
| 11 | G1/G1 | Severe | Mild to moderate | Mild | Mild to moderate | N | N | N | Peleg [9] |
| 12 | N/A | Present | N/A | N/A | N/A | Y | N | N | Gailard [10] |
| 13 | G1/G1 | Moderate to severe | Diffuse | Mild | N/A | N | N | N/A | Magoon [11] 1 |
| 14 | G1/G2 | Moderate | Mild | Mild | Severe | N | N | N/A | Magoon [11] 2 |
| 15 | Note 2 | Severe | N/A | N/A | N/A | N/A | N/A | N | Lazareth [12] |
| 16 | G1/G1 | Focal | N/A | Mild | N/A | Y | N | N | Wu [13] 1 |
| 17 | G2/G2 | Diffuse | N/A | Mild | N/A | N | N | N | Wu [13] 2 |
| 18 | G1/G1 | Diffuse | N/A | Mild to moderate | N/A | Y | N | N | Wu [13] 3 |
| 19 | G1/G1 | Diffuse | N/A | Moderate | N/A | Y | N | N | Wu [13] 4 |
| 20 | G1/G2 | Diffuse | N/A | Moderate | N/A | N | N | N | Wu [13] 5 |
| 21 | G1/G1 | Diffuse | N/A | Mild | N/A | N/A | N/A | N | Wu [13] 6 |
| 22 | N/A | Moderate to severe | N/A | N/A | Severe | N | Y | N/A | Gupta [14] 1 |
| 23 | N/A | Moderate | Mild | N/A | N/A | N | Y | N/A | Gupta [14] 2 |
| 24 | N/A | Present | N/A | N/A | N/A | N | Y | N/A | Kadosh [15] |
| 25 | N/A | Severe | N/A | Mild | N/A | Y | Y | N/A | Noble [16] 1 |
| 26 | N/A | Severe | Present | Mild | Present | N/A | N/A | N/A | Noble [16] 2 |
| 27 | G1/G1 | Present | N/A | N/A | N/A | N | Y | N | Kissling [17] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira, P.; Cunha, K.; Neves, P.; Muniz, M.; Gatto, G.; Salgado Filho, N.; Guedes, F.; Silva, G. Renal Morphology in Coronavirus Disease: A Literature Review. Medicina 2021, 57, 258. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030258
de Oliveira P, Cunha K, Neves P, Muniz M, Gatto G, Salgado Filho N, Guedes F, Silva G. Renal Morphology in Coronavirus Disease: A Literature Review. Medicina. 2021; 57(3):258. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030258
Chicago/Turabian Stylede Oliveira, Patrick, Kaile Cunha, Precil Neves, Monique Muniz, Giuseppe Gatto, Natalino Salgado Filho, Felipe Guedes, and Gyl Silva. 2021. "Renal Morphology in Coronavirus Disease: A Literature Review" Medicina 57, no. 3: 258. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030258