
Unicompartmental Knee Arthroplasty: Minimal Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessment Instruments
2.1.1. FJS-12
2.1.2. OKS
2.2. Statistical Analysis
2.2.1. Distribution-Based Approach for MCID
2.2.2. Anchor Approaches for MCID
2.2.3. Calculation Methods for PASS
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 0.5 SD | 0.5 standard deviation |
| CD | Change Difference |
| FJS-12 | Forgotten Joint Score-12 |
| MC | Mean Change |
| MCID | Minimum Clinically Important Difference |
| MDC | minimum detectable change |
| MIC | Minimum Important Change |
| OKS | The Oxford Knee Score |
| PASS | Patient Acceptable Symptom State |
| PROMs | Patient-reported outcome measure |
| ROC/AUC | Receiver operating characteristic |
| SEM | Standard Error of Measurement |
| SF-36 | Short Form Health Survey |
| TKA | Total Knee Arthroplasty |
| UKA | Unicompartmental Knee Arthroplasty |
| WOMAC | Western Ontario and McMaster University Osteoarthritis Index |
References
- Wilson, H.A.; Middleton, R.; Abram, S.G.F.; Smith, S.; Alvand, A.; Jackson, W.F.; Bottomley, N.; Hopewell, S.; Price, A.J. Patient relevant outcomes of unicompartmental versus total knee replacement: Systematic review and meta-analysis. BMJ 2019, 364, l352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arirachakaran, A.; Choowit, P.; Putananon, C.; Muangsiri, S.; Kongtharvonskul, J. Is unicompartmental knee arthroplasty (UKA) superior to total knee arthroplasty (TKA)? A systematic review and meta-analysis of randomized controlled trial. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Trovato, U.; Rizzello, G.; Maffulli, N.; Denaro, V. No difference between unicompartmental versus total knee arthroplasty for the management of medial osteoarthtritis of the knee in the same patient: A systematic review and pooling data analysis. Br. Med. Bull. 2015, 114, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Drager, J.; Hart, A.; Khalil, J.A.; Zukor, D.J.; Bergeron, S.G.; Antoniou, J. Shorter Hospital Stay and Lower 30-Day Readmission After Unicondylar Knee Arthroplasty Compared to Total Knee Arthroplasty. J. Arthroplast. 2016, 31, 356–361. [Google Scholar] [CrossRef]
- Wang, Z.; Deng, W.; Shao, H.; Zhou, Y.; Li, H. Forgotten Joint Score Thresholds for Forgotten Joint Status and Patient Satisfaction after Unicompartmental Knee Arthroplasty in Chinese Patients. J. Arthroplast. 2020, 35, 2825–2829. [Google Scholar] [CrossRef]
- Putman, S.; Dartus, J.; Migaud, H.; Pasquier, G.; Girard, J.; Preda, C.; Duhamel, A. Can the minimal clinically important difference be determined in a French-speaking population with primary hip replacement using one PROM item and the Anchor strategy? Orthop. Traumatol. Surg. Res. 2021, 102830. [Google Scholar] [CrossRef]
- Wiklund, I. Assessment of patient-reported outcomes in clinical trials: The example of health-related quality of life. Fundam. Clin. Pharmacol. 2004, 18, 351–363. [Google Scholar] [CrossRef]
- Sedaghat, A.R. Understanding the Minimal Clinically Important Difference (MCID) of Patient-Reported Outcome Measures. Otolaryngol. Head Neck Surg. 2019, 161, 551–560. [Google Scholar] [CrossRef]
- Walker, L.C.; Clement, N.D.; Deehan, D.J. Predicting the Outcome of Total Knee Arthroplasty Using the WOMAC Score: A Review of the Literature. J. Knee Surg. 2019, 32, 736–741. [Google Scholar] [CrossRef]
- Giesinger, J.M.; Hamilton, D.F.; Jost, B.; Behrend, H.; Giesinger, K. WOMAC, EQ-5D and Knee Society Score Thresholds for Treatment Success After Total Knee Arthroplasty. J. Arthroplast. 2015, 30, 2154–2158. [Google Scholar] [CrossRef] [Green Version]
- Ethgen, O.; Bruyère, O.; Richy, F.; Dardennes, C.; Reginster, J.Y. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J. Bone Joint Surg. Am. 2004, 86, 963–974. [Google Scholar] [CrossRef]
- Roos, E.M.; Toksvig-Larsen, S. Knee injury and Osteoarthritis Outcome Score (KOOS) - validation and comparison to the WOMAC in total knee replacement. Health Qual. Life Outcomes 2003, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.S.; Koh, I.J.; Choi, Y.J.; Lee, J.Y.; In, Y. Differences in Patient-Reported Outcomes Between Unicompartmental and Total Knee Arthroplasties: A Propensity Score-Matched Analysis. J. Arthroplast. 2017, 32, 1453–1459. [Google Scholar] [CrossRef]
- Sansone, V.; Fennema, P.; Applefield, R.C.; Marchina, S.; Ronco, R.; Pascale, W.; Pascale, V. Translation, cross-cultural adaptation, and validation of the Italian language Forgotten Joint Score-12 (FJS-12) as an outcome measure for total knee arthroplasty in an Italian population. BMC Musculoskelet. Disord. 2020, 21, 23. [Google Scholar] [CrossRef]
- Behrend, H.; Giesinger, K.; Giesinger, J.M.; Kuster, M.S. The “forgotten joint” as the ultimate goal in joint arthroplasty: Validation of a new patient-reported outcome measure. J. Arthroplast. 2012, 27, 430–436.e431. [Google Scholar] [CrossRef]
- Giesinger, K.; Hamilton, D.F.; Jost, B.; Holzner, B.; Giesinger, J.M. Comparative responsiveness of outcome measures for total knee arthroplasty. Osteoarthr. Cartil. 2014, 22, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Niama Natta, D.D.; Thienpont, E.; Bredin, A.; Salaun, G.; Detrembleur, C. Rasch analysis of the Forgotten Joint Score in patients undergoing knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1984–1991. [Google Scholar] [CrossRef]
- Longo, U.G.; De Salvatore, S.; Piergentili, I.; Indiveri, A.; Di Naro, C.; Santamaria, G.; Marchetti, A.; Marinis, M.G.; Denaro, V. Total Hip Arthroplasty: Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score 12. Int. J. Environ. Res. Public Health 2021, 18, 2267. [Google Scholar] [CrossRef]
- Holtz, N.; Hamilton, D.F.; Giesinger, J.M.; Jost, B.; Giesinger, K. Minimal important differences for the WOMAC osteoarthritis index and the Forgotten Joint Score-12 in total knee arthroplasty patients. BMC Musculoskelet. Disord. 2020, 21, 401. [Google Scholar] [CrossRef]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Wu, P.T.; Shao, C.J.; Wu, K.C.; Wu, T.T.; Chern, T.C.; Kuo, L.C.; Jou, I.M. Pain in patients with equal radiographic grades of osteoarthritis in both knees: The value of gray scale ultrasound. Osteoarthr. Cartil. 2012, 20, 1507–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvien, T.K.; Heiberg, T.; Hagen, K.B. Minimal clinically important improvement/difference (MCII/MCID) and patient acceptable symptom state (PASS): What do these concepts mean? Ann. Rheum. Dis. 2007, 66 (Suppl. 3), iii40–iii41. [Google Scholar] [CrossRef] [PubMed]
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; et al. Evaluation of clinically relevant states in patient reported outcomes in knee and hip osteoarthritis: The patient acceptable symptom state. Ann. Rheum. Dis. 2005, 64, 34–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.T. Unicompartmental Knee Arthroplasty. Knee Surg. Relat. Res. 2018, 30, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Ingelsrud, L.H.; Roos, E.M.; Terluin, B.; Gromov, K.; Husted, H.; Troelsen, A. Minimal important change values for the Oxford Knee Score and the Forgotten Joint Score at 1 year after total knee replacement. Acta Orthop. 2018, 89, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, D.F.; Loth, F.L.; Giesinger, J.M.; Giesinger, K.; MacDonald, D.J.; Patton, J.T.; Simpson, A.H.; Howie, C.R. Validation of the English language Forgotten Joint Score-12 as an outcome measure for total hip and knee arthroplasty in a British population. Bone Joint J. 2017, 99, 218–224. [Google Scholar] [CrossRef]
- Den Oudsten, B.L.; Zijlstra, W.P.; De Vries, J. The minimal clinical important difference in the World Health Organization Quality of Life instrument—100. Support. Care Cancer 2013, 21, 1295–1301. [Google Scholar] [CrossRef]
- Kwakkenbos, L.; Fransen, J.; Vonk, M.C.; Becker, E.S.; Jeurissen, M.; van den Hoogen, F.H.; van den Ende, C.H. A comparison of the measurement properties and estimation of minimal important differences of the EQ-5D and SF-6D utility measures in patients with systemic sclerosis. Clin. Exp. Rheumatol. 2013, 31, 50–56. [Google Scholar]
- Beard, D.J.; Harris, K.; Dawson, J.; Doll, H.; Murray, D.W.; Carr, A.J.; Price, A.J. Meaningful changes for the Oxford hip and knee scores after joint replacement surgery. J. Clin. Epidemiol. 2015, 68, 73–79. [Google Scholar] [CrossRef]
- Revicki, D.; Hays, R.D.; Cella, D.; Sloan, J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J. Clin. Epidemiol. 2008, 61, 102–109. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Robinson, P.G.; Rankin, C.S.; Murray, I.R.; Maempel, J.F.; Gaston, P.; Hamilton, D.F. The forgotten joint score-12 is a valid and responsive outcome tool for measuring success following hip arthroscopy for femoroacetabular impingement syndrome. Knee Surg. Sports Traumatol. Arthrosc. 2020. [Google Scholar] [CrossRef]
- Behrend, H.; Zdravkovic, V.; Giesinger, J.M.; Giesinger, K. Joint awareness after ACL reconstruction: Patient-reported outcomes measured with the Forgotten Joint Score-12. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1454–1460. [Google Scholar] [CrossRef]
- Bin Abd Razak, H.R.; Acharyya, S.; Tan, S.M.; Pang, H.N.; Tay, K.D.; Chia, S.L.; Lo, N.N.; Yeo, S.J. Predictors of Midterm Outcomes after Medial Unicompartmental Knee Arthroplasty in Asians. Clin. Orthop. Surg. 2017, 9, 432–438. [Google Scholar] [CrossRef]
- Xia, Z.; Liow, M.H.L.; Goh, G.S.; Chong, H.C.; Lo, N.N.; Yeo, S.J. Body mass index changes after unicompartmental knee arthroplasty do not adversely influence patient outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1691–1697. [Google Scholar] [CrossRef]
- Liow, M.H.L.; Goh, G.S.; Pang, H.N.; Tay, D.K.; Chia, S.L.; Lo, N.N.; Yeo, S.J. Should patients aged 75 years or older undergo medial unicompartmental knee arthroplasty? A propensity score-matched study. Arch. Orthop. Trauma Surg. 2020, 140, 949–956. [Google Scholar] [CrossRef]
- Sloan, J.A.; Cella, D.; Hays, R.D. Clinical significance of patient-reported questionnaire data: Another step toward consensus. J. Clin. Epidemiol. 2005, 58, 1217–1219. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Wyrwich, K.W.; Nienaber, N.A.; Tierney, W.M.; Wolinsky, F.D. Linking clinical relevance and statistical significance in evaluating intra-individual changes in health-related quality of life. Med. Care 1999, 37, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E. Understanding the relevance of measured change through studies of responsiveness. Spine 2000, 25, 3192–3199. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.L.; Adogwa, O.; Mendenhall, S.K.; Shau, D.N.; Anderson, W.N.; Cheng, J.S.; Devin, C.J.; McGirt, M.J. Determination of minimum clinically important difference (MCID) in pain, disability, and quality of life after revision fusion for symptomatic pseudoarthrosis. Spine J. 2012, 12, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.D.; Woolley, J.M. The concept of clinically meaningful difference in health-related quality-of-life research. How meaningful is it? Pharmacoeconomics 2000, 18, 419–423. [Google Scholar] [CrossRef]
- Copay, A.G.; Glassman, S.D.; Subach, B.R.; Berven, S.; Schuler, T.C.; Carreon, L.Y. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J. 2008, 8, 968–974. [Google Scholar] [CrossRef]
- Çelik, D.; Çoban, Ö.; Kılıçoğlu, Ö. Minimal clinically important difference of commonly used hip-, knee-, foot-, and ankle-specific questionnaires: A systematic review. J. Clin. Epidemiol. 2019, 113, 44–57. [Google Scholar] [CrossRef]
- MacKay, C.; Clements, N.; Wong, R.; Davis, A.M. A systematic review of estimates of the minimal clinically important difference and patient acceptable symptom state of the Western Ontario and McMaster Universities Osteoarthritis Index in patients who underwent total hip and total knee replacement. Osteoarthr. Cartil. 2019, 27, 1408–1419. [Google Scholar] [CrossRef]
- Maredupaka, S.; Meshram, P.; Chatte, M.; Kim, W.H.; Kim, T.K. Minimal clinically important difference of commonly used patient-reported outcome measures in total knee arthroplasty: Review of terminologies, methods and proposed values. Knee Surg. Relat. Res. 2020, 32, 19. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| MCID | Cut-Off Value | Anchor |
|---|---|---|
| 0.5 SD | 8.8 | / |
| SEM | 5.7 | / |
| MDC | 15.7 | / |
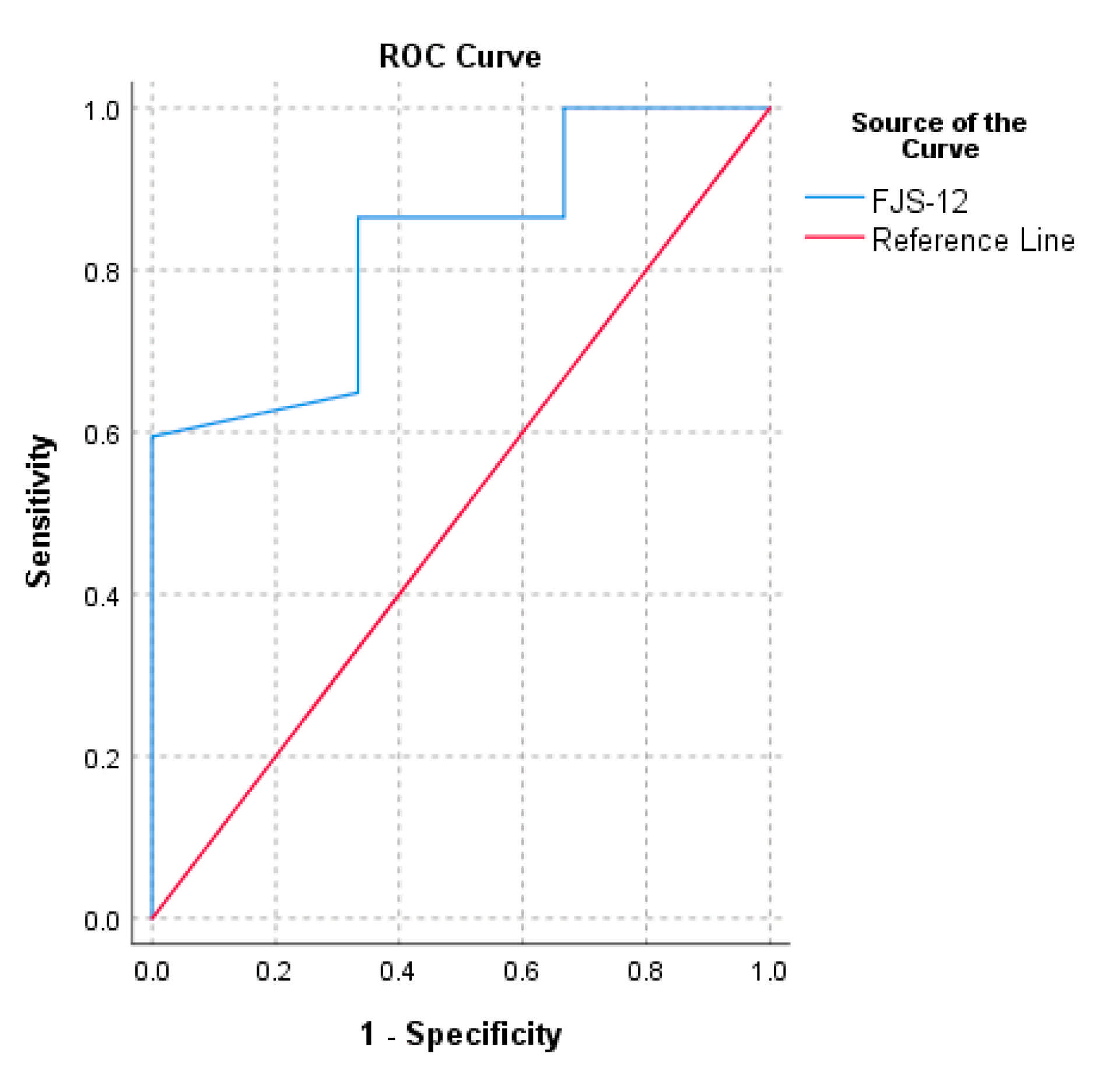
| ROC (AUC) | 12.5 (0.8) | OKS > 5 |
| CD | 19.8 | OKS > 5 |
| MC | 15.7 | OKS > 5 |
| PASS | Cut-Off Value | Anchor |
|---|---|---|
| ROC (AUC) | 72.9 (0.8) | In general, would you say that your health is at least good? |
| 75th percentile | 92.7 | In general, would you say that your health is at least good? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; De Salvatore, S.; Candela, V.; Berton, A.; Casciaro, C.; Sciotti, G.; Cirimele, G.; Marchetti, A.; Piergentili, I.; De Marinis, M.G.; et al. Unicompartmental Knee Arthroplasty: Minimal Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score. Medicina 2021, 57, 324. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57040324
Longo UG, De Salvatore S, Candela V, Berton A, Casciaro C, Sciotti G, Cirimele G, Marchetti A, Piergentili I, De Marinis MG, et al. Unicompartmental Knee Arthroplasty: Minimal Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score. Medicina. 2021; 57(4):324. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57040324
Chicago/Turabian StyleLongo, Umile Giuseppe, Sergio De Salvatore, Vincenzo Candela, Alessandra Berton, Carlo Casciaro, Gaia Sciotti, Giada Cirimele, Anna Marchetti, Ilaria Piergentili, Maria Grazia De Marinis, and et al. 2021. "Unicompartmental Knee Arthroplasty: Minimal Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score" Medicina 57, no. 4: 324. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57040324