
Heritability of Cardiothoracic Ratio and Aortic Arch Calcification in Twins

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
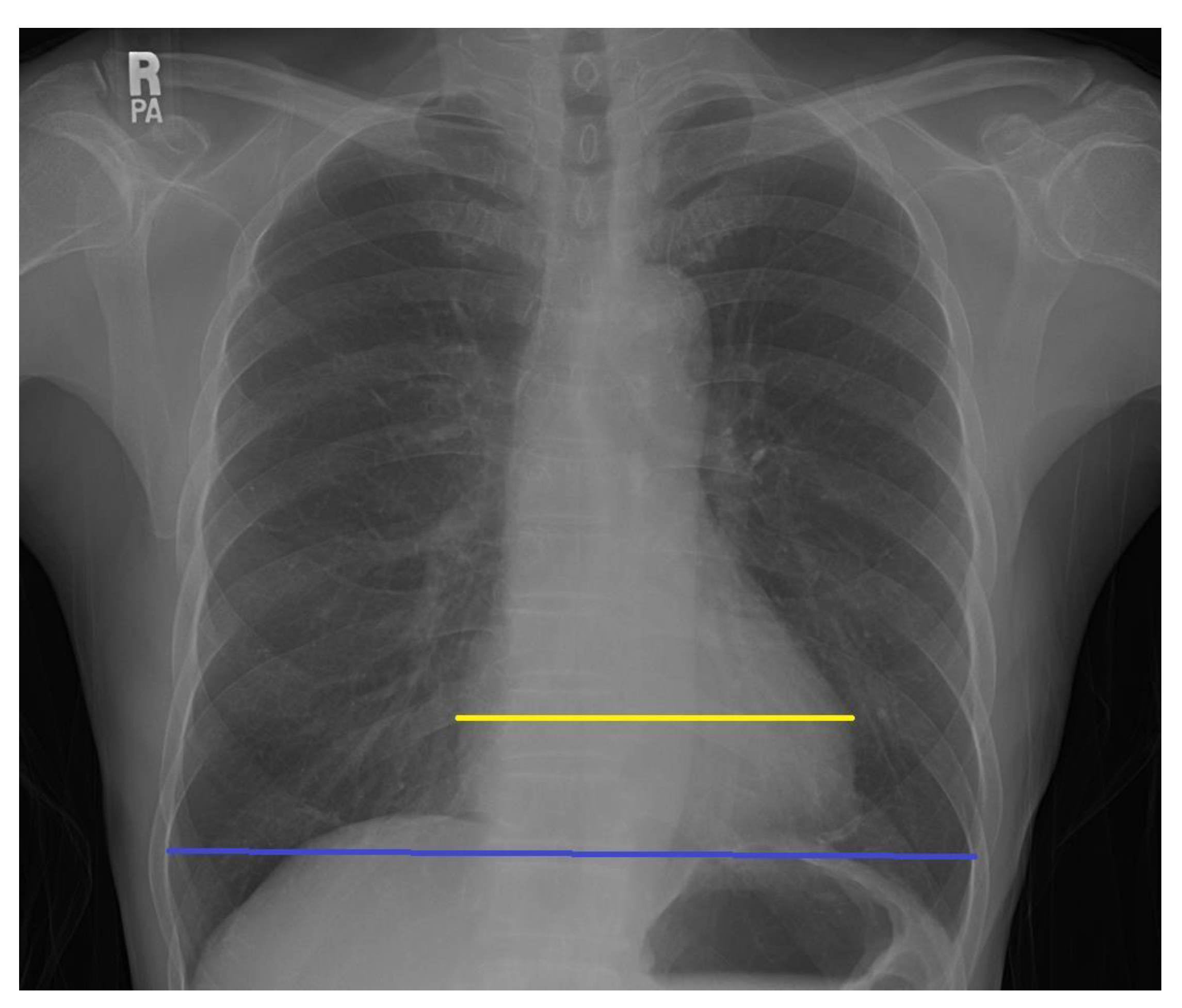
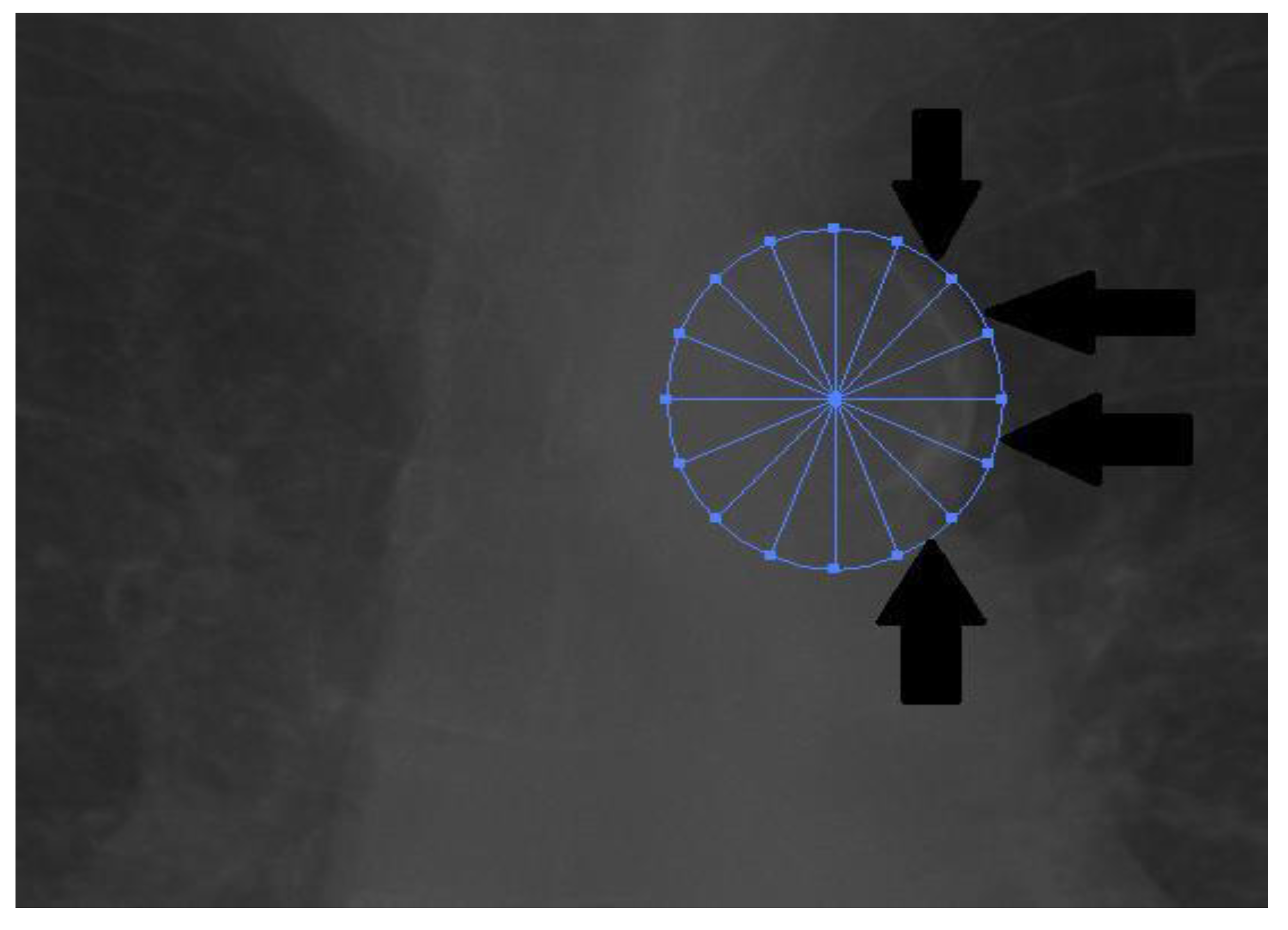
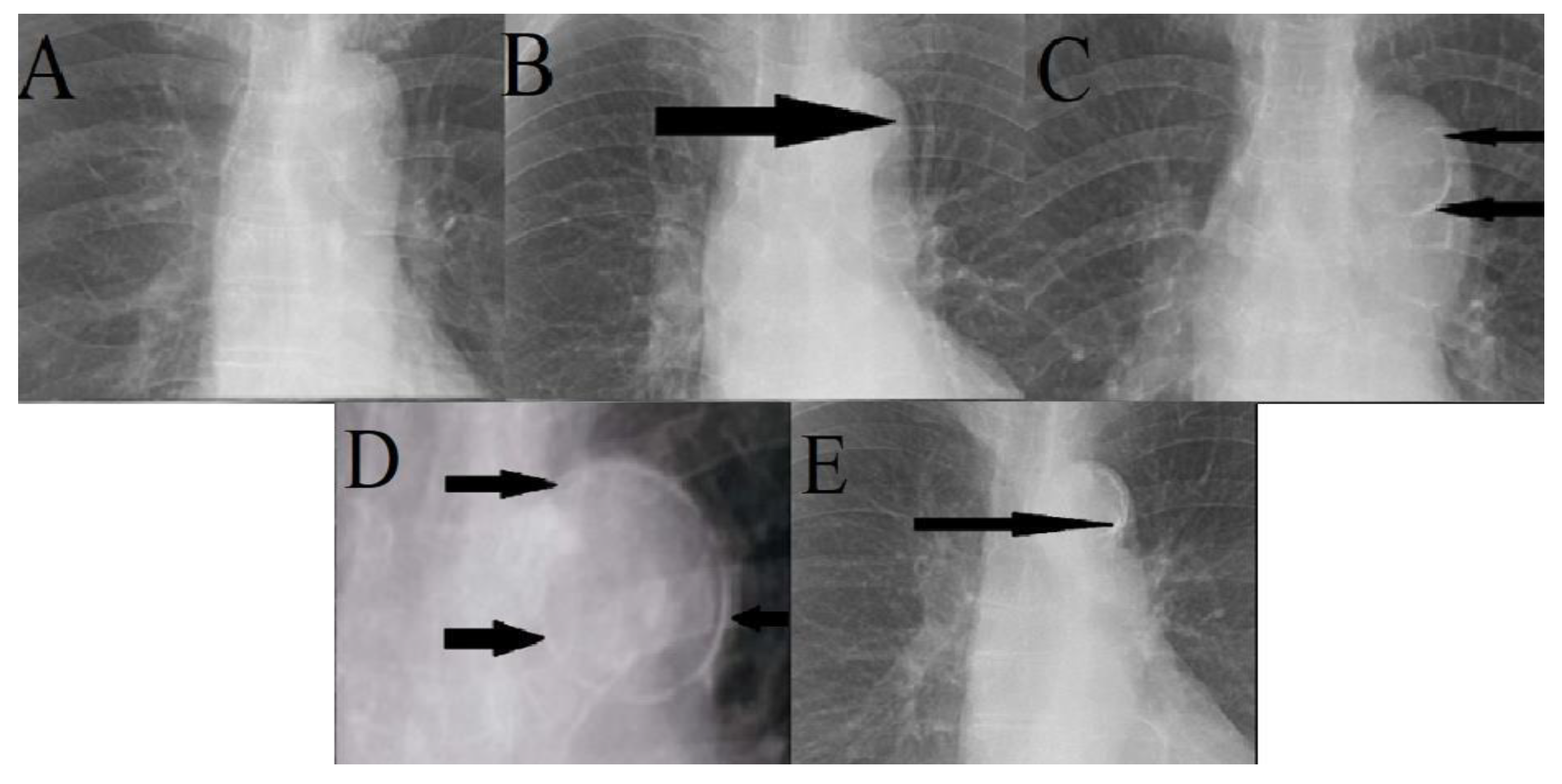
2.2. Measurement
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Cardiac Size, Thoracic Size, and Cardiothoracic Ratio
3.3. Aortic Arch Calcification of MZ and DZ Twins
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lusis, A.J. Atherosclerosis. Nature 2000, 407, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Insull, W., Jr. The pathology of atherosclerosis: Plaque development and plaque responses to medical treatment. Am. J. Med. 2009, 122, S3–S14. [Google Scholar] [CrossRef]
- Bergheanu, S.C.; Bodde, M.C.; Jukema, J.W. Pathophysiology and treatment of atherosclerosis: Current view and future perspective on lipoprotein modification treatment. Neth Heart J. 2017, 25, 231–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molisse, T.A.; Tunick, P.A.; Kronzon, I. Complications of aortic atherosclerosis: Atheroemboli and thromboemboli. Curr. Treat. Options Cardiovasc. Med. 2007, 9, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Mensah, Y.B.; Mensah, K.; Asiamah, S.; Gbadamosi, H.; Idun, E.A.; Brakohiapa, W.; Oddoye, A. Establishing the Cardiothoracic Ratio Using Chest Radiographs in an Indigenous Ghanaian Population: A Simple Tool for Cardiomegaly Screening. Ghana Med. J. 2015, 49, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hada, Y. Cardiothoracic ratio. J. Cardiol. 1995, 26, 51–54. [Google Scholar]
- Iribarren, C.; Sidney, S.; Sternfeld, B.; Browner, W.S. Calcification of the aortic arch: Risk factors and association with coronary heart disease, stroke, and peripheral vascular disease. JAMA 2000, 283, 2810–2815. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Hou, F.; Tian, J.; Zhou, Z.; Ma, Y.; Cheng, Y.; Du, Y.; Shen, H.; Hu, B.; Wang, Z.; et al. Aortic Arch Calcification Is a Strong Predictor of the Severity of Coronary Artery Disease in Patients with Acute Coronary Syndrome. Biomed. Res. Int. 2019, 2019, 7659239. [Google Scholar] [CrossRef] [Green Version]
- Iijima, K.; Hashimoto, H.; Hashimoto, M.; Son, B.K.; Ota, H.; Ogawa, S.; Eto, M.; Akishita, M.; Ouchi, Y. Aortic arch calcification detectable on chest X-ray is a strong independent predictor of cardiovascular events beyond traditional risk factors. Atherosclerosis 2010, 210, 137–144. [Google Scholar] [CrossRef]
- Woo, J.S.; Kim, W.; Kwon, S.H.; Youn, H.C.; Kim, H.S.; Kim, J.B.; Kim, S.J.; Kim, W.S.; Kim, K.S. Aortic arch calcification on chest X-ray combined with coronary calcium score show additional benefit for diagnosis and outcome in patients with angina. J. Geriatr Cardiol. 2016, 13, 218–225. [Google Scholar] [CrossRef]
- Medda, E.; Fagnani, C.; Schillaci, G.; Tarnoki, A.D.; Tarnoki, D.L.; Baracchini, C.; Meneghetti, G.; Fanelli, F.; Alaeddin, A.; Pucci, G.; et al. Heritability of arterial stiffness and carotid intima-media thickness: An Italian twin study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 511–517. [Google Scholar] [CrossRef]
- Joergensen, T.M.; Christensen, K.; Lindholt, J.S.; Larsen, L.A.; Green, A.; Houlind, K. Editor’s Choice—High Heritability of Liability to Abdominal Aortic Aneurysms: A Population Based Twin Study. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Wahlgren, C.M.; Larsson, E.; Magnusson, P.K.; Hultgren, R.; Swedenborg, J. Genetic and environmental contributions to abdominal aortic aneurysm development in a twin population. J. Vasc. Surg. 2010, 51, 3–7, discussion 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, T.; Ishida, H.; Matsuda, N.; Fujiu, A.; Matsuda, A.; Ito, K.; Ando, Y.; Nitta, K. Simple evaluation of aortic arch calcification by chest radiography in hemodialysis patients. Hemodial. Int. 2009, 13, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Iijima, K.; Hashimoto, M.; Son, B.K.; Ota, H.; Ogawa, S.; Eto, M.; Akishita, M.; Ouchi, Y. Validity and usefulness of aortic arch calcification in chest X-ray. J. Atheroscler. Thromb. 2009, 16, 256–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagard, R.; Van Den Broeke, C.; Bielen, E.; Amery, A. Maximum oxygen uptake and cardiac size and function in twins. Am. J. Cardiol. 1987, 60, 1362–1367. [Google Scholar] [CrossRef]
- Busjahn, A.; Li, G.H.; Faulhaber, H.D.; Rosenthal, M.; Becker, A.; Jeschke, E.; Schuster, H.; Timmermann, B.; Hoehe, M.R.; Luft, F.C. beta-2 adrenergic receptor gene variations, blood pressure, and heart size in normal twins. Hypertension 2000, 35, 555–560. [Google Scholar] [CrossRef] [Green Version]
- Bellenger, N.G.; Davies, L.C.; Francis, J.M.; Coats, A.J.; Pennell, D.J. Reduction in sample size for studies of remodeling in heart failure by the use of cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2000, 2, 271–278. [Google Scholar] [CrossRef]
- Strohm, O.; Schulz-Menger, J.; Pilz, B.; Osterziel, K.J.; Dietz, R.; Friedrich, M.G. Measurement of left ventricular dimensions and function in patients with dilated cardiomyopathy. J. Magn. Reson. Imaging 2001, 13, 367–371. [Google Scholar] [CrossRef]
- Busjahn, C.A.; Schulz-Menger, J.; Abdel-Aty, H.; Rudolph, A.; Jordan, J.; Luft, F.C.; Busjahn, A. Heritability of left ventricular and papillary muscle heart size: A twin study with cardiac magnetic resonance imaging. Eur. Heart J. 2009, 30, 1643–1647. [Google Scholar] [CrossRef]
- Adams, T.D.; Yanowitz, F.G.; Fisher, A.G.; Ridges, J.D.; Nelson, A.G.; Hagan, A.D.; Williams, R.R.; Hunt, S.C. Heritability of cardiac size: An echocardiographic and electrocardiographic study of monozygotic and dizygotic twins. Circulation 1985, 71, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Williams-Blangero, S.; Blangero, J.; Beall, C.M. Genetic analysis of chest dimensions in a high altitude Tibetan population from upper Chumik, Nepal. Am. J. Hum. Biol. 1993, 5, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Das, N.; Chatterjee, P. The estimation of the heritability of anthropometric measurements. Appl. Human Sci. 1999, 18, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Rutsch, F.; Nitschke, Y.; Terkeltaub, R. Genetics in arterial calcification: Pieces of a puzzle and cogs in a wheel. Circ. Res. 2011, 109, 578–592. [Google Scholar] [CrossRef] [PubMed]
- Thanassoulis, G.; Campbell, C.Y.; Owens, D.S.; Smith, J.G.; Smith, A.V.; Peloso, G.M.; Kerr, K.F.; Pechlivanis, S.; Budoff, M.J.; Harris, T.B.; et al. Genetic associations with valvular calcification and aortic stenosis. N. Engl. J. Med. 2013, 368, 503–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, C.J.; Chazaro, I.; Wilson, P.W.; Fox, C.; Hannan, M.T.; Kiel, D.P.; Cupples, L.A. Evidence for heritability of abdominal aortic calcific deposits in the Framingham Heart Study. Circulation 2002, 106, 337–341. [Google Scholar] [CrossRef] [Green Version]
- Cecelja, M.; Jiang, B.; Bevan, L.; Frost, M.L.; Spector, T.D.; Chowienczyk, P.J. Arterial stiffening relates to arterial calcification but not to noncalcified atheroma in women. A twin study. J. Am. Coll. Cardiol. 2011, 57, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Cecelja, M.; Hussain, T.; Greil, G.; Botnar, R.; Preston, R.; Moayyeri, A.; Spector, T.D.; Chowienczyk, P. Multimodality imaging of subclinical aortic atherosclerosis: Relation of aortic stiffness to calcification and plaque in female twins. Hypertension 2013, 61, 609–614. [Google Scholar] [CrossRef] [Green Version]
- Adams, H.H.; Ikram, M.A.; Vernooij, M.W.; van Dijk, A.C.; Hofman, A.; Uitterlinden, A.G.; van Duijn, C.M.; Koudstaal, P.J.; Franco, O.H.; van der Lugt, A.; et al. Heritability and Genome-Wide Association Analyses of Intracranial Carotid Artery Calcification: The Rotterdam Study. Stroke 2016, 47, 912–917. [Google Scholar] [CrossRef] [Green Version]
- Adelmann, G.A. Cardiology Essentials in Clinical Practice; Media, L.S.S.B., Ed.; Springer: London, UK, 2010. [Google Scholar]
- Inoue, T.; Ogawa, T.; Ishida, H.; Ando, Y.; Nitta, K. Aortic arch calcification evaluated on chest X-ray is a strong independent predictor of cardiovascular events in chronic hemodialysis patients. Heart Vessels 2012, 27, 135–142. [Google Scholar] [CrossRef]
- Messerli, M.; Giannopoulos, A.A.; Leschka, S.; Warschkow, R.; Wildermuth, S.; Hechelhammer, L.; Bauer, R.W. Diagnostic accuracy of chest X-ray dose-equivalent CT for assessing calcified atherosclerotic burden of the thoracic aorta. Br. J. Radiol. 2017, 90, 20170469. [Google Scholar] [CrossRef] [PubMed]
- Kalsch, H.; Lehmann, N.; Moebus, S.; Hoffmann, B.; Stang, A.; Jockel, K.H.; Erbel, R.; Mahabadi, A.A. Aortic Calcification Onset and Progression: Association With the Development of Coronary Atherosclerosis. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsakiris, A.; Doumas, M.; Nearchos, N.; Mavrokefalos, A.; Mpatakis, N.; Skoufas, P. Aortic calcification is associated with age and sex but not left ventricular mass in essential hypertension. J. Clin. Hypertens Greenwich 2004, 6, 65–70. [Google Scholar] [CrossRef] [PubMed]
- El-Saed, A.; Curb, J.D.; Kadowaki, T.; Okamura, T.; Sutton-Tyrrell, K.; Masaki, K.; Seto, T.B.; Takamiya, T.; Choo, J.; Edmundowicz, D.; et al. The prevalence of aortic calcification in Japanese compared to white and Japanese-American middle-aged men is confounded by the amount of cigarette smoking. Int. J. Cardiol. 2013, 167, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 684) | MZ Twins (n = 522) | DZ Twins (n = 162) | |
|---|---|---|---|
| Age (years) | 38.6 ± 8.0 | 38.3 ** ± 8.0 | 39.8 ** ± 7.7 |
| Sex | Males: 264 (39%) | Males: 192 (37%) | Males: 72 (44%) |
| Females: 420 (61%) | Females: 330 (63%) | Females: 90 (56%) | |
| Height (cm) | 162.2 ± 8.3 | 161.9 * ± 8.1 | 163.2 * ± 8.7 |
| Weight (kg) | 61.3 ± 11.7 | 60.8 * ± 11.2 | 62.9 * ± 12.9 |
| Waist (cm) | 79.0 ± 8.9 | 78.8 ± 8.6 | 79.8 ± 9.5 |
| BMI (kg/m2) | 23.2 ± 3.1 | 23.1 ± 3.0 | 23.4 ± 3.4 |
| Systolic blood pressure, left (mmHg) | 109.5 ± 15.9 | 107.8 *** ± 15.6 | 115.0 *** ± 15.6 |
| Diastolic blood pressure, left (mmHg) | 69.4 ± 10.7 | 68.5 *** ± 10.9 | 72.2 *** ± 9.4 |
| Systolic blood pressure, right (mmHg) | 109.7 ± 16.0 | 108.0 *** ± 15.5 | 115.4 *** ± 16.1 |
| Diastolic blood pressure, right (mmHg) | 69.4 ± 10.7 | 68.5 *** ± 10.9 | 72.1 *** ± 9.8 |
| Mean systolic blood pressure (mmHg) | 111.0 ± 16.1 | 109.2 *** ± 15.8 | 116.8 *** ± 16.0 |
| Mean diastolic blood pressure (mmHg) | 70.2 ± 11.0 | 69.3 *** ± 11.1 | 73.1 *** ± 9.9 |
| Smoking n (%) | 241 (35%) | 177 (33%) | 64 (40%) |
| History of stroke, n (%) | 1 (0.1%) | 1 (0.2%) | 0 (0%) |
| History of myocardial infarction, n (%) | 9 (1%) | 5 (1%) | 4 (2%) |
| Hypertension, n (%) | 63 (9%) | 40 (8%) | 23 (14%) |
| Hyperlipidemia, n (%) | 55 (8%) | 42 (8%) | 13 (8%) |
| Diabetes mellitus, n (%) | 22 (3%) | 18 (3%) | 4 (2%) |
| Cardiac width (cm) | 22.9 ± 3.1 | 22.8 ± 3.0 | 23.0 ± 3.4 |
| Thoracic width (cm) | 50.0 ± 5.2 | 49.8 * ± 4.8 | 50.8 * ± 6.3 |
| Cardiothoracic ratio | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.5 ± 0.1 |
| No visible calcification | 0.98 ± 0.13 | 0.98 ± 0.12 | 0.98 ± 0.16 |
| Small spots or single thin area | 0.01 ± 0.12 | 0.01 ± 0.11 | 0.02 ± 0.16 |
| One or more areas of thick calcification | 0 ± 0.05 | 0 ± 0.06 | 0 ± 0 |
| Circular calcification | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| No visible calcification_2 | 0.98 ± 0.13 | 0.98 ± 0.12 | 0.98 ± 0.16 |
| <50% calc_2 | 0.02 ± 0.13 | 0.01 ± 0.11 | 0.02 ± 0.16 |
| >50% calc_2 | 0 ± 0.04 | 0 ± 0.04 | 0 ± 0 |
| Circular calcification_2 | 0 ± 0 | 0 ± 0 | 0 ± 0 |
| Number of calcificated segments | 0.07 ± 0.58 | 0.06 ± 0.59 | 0.08 ± 0.56 |
| Aortic calcification score | 0 ± 0.04 | 0 ± 0.04 | 0.01 ± 0.03 |
| ACE model 1 | Results (95% CI) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Thoracic width | AIC | BIC | -2LL | df | DiffLL | p value | A | C | E |
| ACE | 3171.247 | 3175.550 | 3156.912 | 7 | Reference | Reference | 0.67 (0.39, 0.73) | 0 (0, 0.261) | 0.33 (0.28, 0.41) |
| AE * | 3169.162 | 3172.887 | 3156.912 | 6 | 0 | 1 | 0.67 (0.59, 0.73) | 0 | 0.33 (0.28, 0.41) |
| CE | 3190.850 | 3194.575 | 3178.599 | 6 | −21.688 | 0 | 0 | 0.57 (0.49, 0.64) | 0.43 (0.36, 0.51) |
| E | 3320.370 | 3323.504 | 3310.191 | 5 | −153.28 | 0 | 0 | 0 | 1 |
| SAT | 3175.126 | 3181.087 | Rmz: 0.66 (0.585 0.724) | Rdz: 0.307 (0.092 0.495) | |||||
| ACE model 2 | Results (95% CI) | ||||||||
| Cardiac width | AIC | BIC | -2LL | df | DiffLL | p value | A | C | E |
| ACE | 2939.857 | 2944.159 | 2925.521 | 7 | Reference | Reference | 0.42 (0.05, 0.62) | 0.12 (0, 0.459) | 0.46 (0.38, 0.56) |
| AE* | 2938.092 | 2941.817 | 2925.841 | 6 | −0.32 | 0.572 | 0.54 (0.45, 0.62) | 0 | 0.46 (0.38, 0.55) |
| CE | 2942.754 | 2946.479 | 2930.504 | 6 | −4.982 | 0.026 | 0 | 0.49 (0.40, 0.56) | 0.51 (0.44, 0.60) |
| E | 3026.992 | 3030.127 | 3016.814 | 5 | −91.292 | 0 | 0 | 0 | 1 |
| SAT | 2945.265 | 2951.227 | Rmz: 0.537 (0.442 0.62) | Rdz: 0.324 (0.113 0.506) | |||||
| ACE model 3 | Results (95% CI) | ||||||||
| Cardiothoracic ratio | AIC | BIC | -2LL | df | DiffLL | p value | A | C | E |
| ACE | −2400 | −2395.697 | −2414.335 | 7 | Reference | Reference | 0.46 (0.18, 0.61) | 0.07 (0, 0.38) | 0.47 (0.39, 0.56) |
| AE* | −2401.937 | −2398.212 | −2414.188 | 6 | −0.148 | 0.701 | 0.54 (0.44, 0.62) | 0 | 0.46 (0.39, 0.56) |
| CE | −2395.032 | −2391.307 | −2407.283 | 6 | −7.052 | 0.008 | 0 | 0.46 (0.37, 0.54) | 0.54 (0.46, 0.63) |
| E | −2316.544 | −2313.410 | −2326.722 | 5 | −87.613 | 0 | 0 | 0 | 1 |
| SAT | −2399.927 | −2393.966 | Rmz: 0.508 (0.412 0.593) | Rdz: 0.348 (0.142 0.525) | |||||
| MZ Twin-Pairs | Type of Calcification | Percentage of Calcification (%) | Number of Calcified Segments | Aortic Calcification Score | ||||
|---|---|---|---|---|---|---|---|---|
| Pair 1 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 2 | Twin B: 0 | Twin A: 0.125 | Twin B: 0 |
| Pair 2 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 5 | Twin B: 0 | Twin A: 0.313 | Twin B: 0 |
| Pair 3 | Twin A: One or more areas of thick calcification | Twin B: No visible calcification | Twin A: >50 | Twin B: 0 | Twin A: 10 | Twin B: 0 | Twin A: 0.625 | Twin B: 0 |
| Pair 4 | Twin A: One or more areas of thick calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 2 | Twin B: 0 | Twin A: 0.125 | Twin B: 0 |
| Pair 5 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 3 | Twin B: 0 | Twin A: 0.188 | Twin B: 0 |
| Pair 6 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 3 | Twin B: 0 | Twin A: 0.188 | Twin B: 0 |
| Pair 7 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 4 | Twin B: 0 | Twin A: 0.250 | Twin B: 0 |
| Pair 8 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 4 | Twin B: 0 | Twin A: 0.250 | Twin B: 0 |
| DZ Twin-Pairs | Type of Calcification | Percentage of Calcification (%) | Number of Calcified Segments | Aortic Calcification Score | ||||
|---|---|---|---|---|---|---|---|---|
| Pair 1 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 3 | Twin B: 0 | Twin A: 0.188 | Twin B: 0 |
| Pair 2 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 4 | Twin B: 0 | Twin A: 0.250 | Twin B: 0 |
| Pair 3 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 5 | Twin B: 0 | Twin A: 0.313 | Twin B: 0 |
| Pair 4 | Twin A: Small spots or a single, thin area of calcification | Twin B: No visible calcification | Twin A: <50 | Twin B: 0 | Twin A: 1 | Twin B: 0 | Twin A: 0.063 | Twin B: 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jokkel, Z.; Forgo, B.; Hani-Gaius Ghattas, C.; Piroska, M.; Szabó, H.; Tarnoki, D.L.; Tarnoki, A.D.; Lee, S.; Sung, J. Heritability of Cardiothoracic Ratio and Aortic Arch Calcification in Twins. Medicina 2021, 57, 421. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050421
Jokkel Z, Forgo B, Hani-Gaius Ghattas C, Piroska M, Szabó H, Tarnoki DL, Tarnoki AD, Lee S, Sung J. Heritability of Cardiothoracic Ratio and Aortic Arch Calcification in Twins. Medicina. 2021; 57(5):421. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050421
Chicago/Turabian StyleJokkel, Zsofia, Bianka Forgo, Christopher Hani-Gaius Ghattas, Marton Piroska, Helga Szabó, David L. Tarnoki, Adam D. Tarnoki, Sooji Lee, and Joohon Sung. 2021. "Heritability of Cardiothoracic Ratio and Aortic Arch Calcification in Twins" Medicina 57, no. 5: 421. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050421