
Oral Anticoagulant Treatment in Patients with Atrial Fibrillation and Chronic Kidney Disease

 ,
,
Abstract
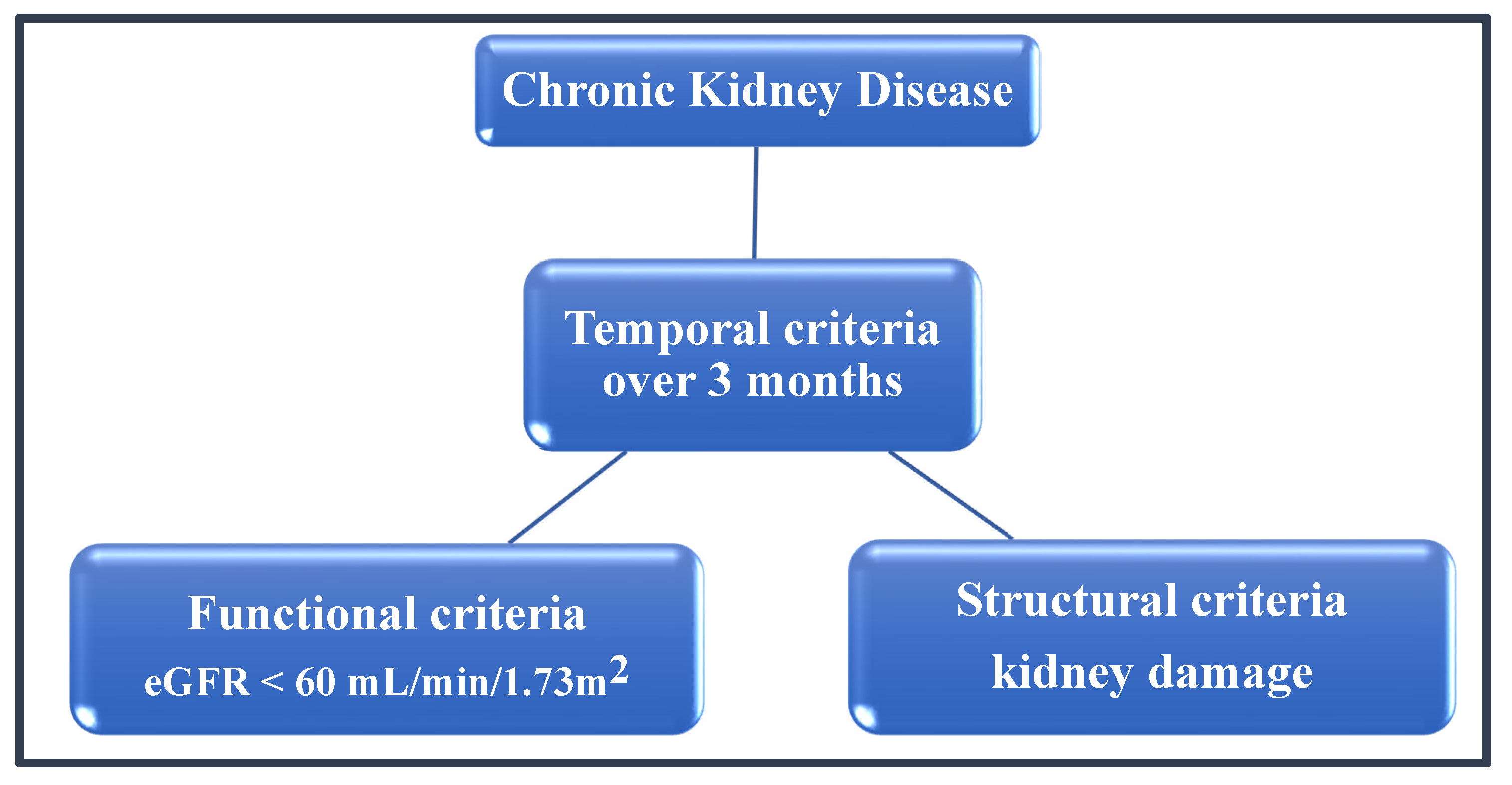
:1. Introduction
2. Coexistence of AF and CKD
3. Oral Anticoagulation in Patients with Atrial Fibrillation—What Does Available Evidence Tell Us?
4. The Use of NOACs in Patients with AF and Concomitant CKD
5. Current International Guidelines for Oral Anticoagulation Treatment in CKD
6. Currently Ongoing Studies on Oral Anticoagulation in ESRD
7. Conclusions
- In mild-to-moderate CKD (eGFR 30–50 mL/min or higher), the registry evidence discussed above suggests that NOACs are preferred options over VKAs for both efficacy and safety. Dose adjustments may be appropriate as directed for the specific agents.
- In severely impaired kidney function (eGFR < 30 mL/min), there is limited evidence to predict how NOACs may compare VKAs, although evidence for superior efficacy and safety over warfarin continues to accumulate. There is no RCT based evidence to support anticoagulation therapy in ESRD. OAT should only be initiated after careful consideration of benefit and harm. Warfarin is generally preferred over a NOAC in patients who require long-term anticoagulation.
- In AF patients that had a history of major bleeding and contraindications to OAT, catheter-based occlusion of the left atrial appendage could be considered.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lloyd-Jones, D.M.; Wang, T.J.; Leip, E.P.; Larson, M.G.; Levy, D.; Vasan, R.S.; D’Agostino, R.B.; Massaro, J.M.; Beiser, A.; Wolf, P.A.; et al. Lifetime risk for development of atrial fibrillation: The Framingham Heart Study. Circulation 2004, 110, 1042–1046. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.M.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar] [CrossRef] [Green Version]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Couser, W.G.; Remuzzi, G.; Mendis, S.; Tonelli, M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011, 80, 1258–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Nahas, A.M.; Bello, A.K. Chronic kidney disease: The global challenge. Lancet 2005, 365, 331–340. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G. National Kidney Foundation Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Ann. Intern. Med. 2003, 139, 137. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A. Estimating GFR Using the CKD Epidemiology Collaboration (CKD-EPI) Creatinine Equation: More Accurate GFR Estimates, Lower CKD Prevalence Estimates, and Better Risk Predictions. Am. J. Kidney Dis. 2010, 55, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S. A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Ann. Intern. Med. 1999, 130, 461. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604. [Google Scholar] [CrossRef]
- Coresh, J.; Stevens, L. Kidney function estimating equations: Where do we stand? Curr. Opin. Nephrol. Hypertens. 2006, 15, 276–284. [Google Scholar] [CrossRef]
- Lamb, E. Assessment of kidney function in adults. Medicine 2019, 47, 482–488. [Google Scholar] [CrossRef]
- Botev, R.; Mallié, J.-P.; Wetzels, J.F.M.; Couchoud, C.; Schück, O. The Clinician and Estimation of Glomerular Filtration Rate by Creatinine-based Formulas: Current Limitations and Quo Vadis. Clin. J. Am. Soc. Nephrol. 2011, 6, 937–950. [Google Scholar] [CrossRef] [Green Version]
- Briasoulis, A.; Bakris, G.L. Chronic Kidney Disease as a Coronary Artery Disease Risk Equivalent. Curr. Cardiol. Rep. 2013, 15, 340. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Blankestijn, P.J.; Carrero, J.-J.; Clase, C.M.; Deo, R.; Herzog, C.A.; Kasner, S.E.; Passman, R.S.; Pecoits-Filho, R.; Reinecke, H.; et al. Chronic kidney disease and arrhythmias: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Eur. Heart J. 2018, 39, 2314–2325. [Google Scholar] [CrossRef] [PubMed]
- Soliman, E.Z.; Prineas, R.J.; Go, A.S.; Xie, D.; Lash, J.P.; Rahman, M.; Ojo, A.; Teal, V.L.; Jensvold, N.G.; Robinson, N.L.; et al. Chronic kidney disease and prevalent atrial fibrillation: The Chronic Renal Insufficiency Cohort (CRIC). Am. Heart J. 2010, 159, 1102–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, H.; Watanabe, T.; Sasaki, S.; Nagai, K.; Roden, D.M.; Aizawa, Y. Close bidirectional relationship between chronic kidney disease and atrial fibrillation: The Niigata preventive medicine study. Am. Heart J. 2009, 158, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Schlaich, M.P. Sympathetic activation in chronic kidney disease: Out of the shadow. Hypertension 2011, 57, 683–685. [Google Scholar] [CrossRef] [Green Version]
- Shlipak, M.G.; Fried, L.F.; Crump, C.; Bleyer, A.J.; Manolio, T.A.; Tracy, R.P.; Furberg, C.D.; Psaty, B.M. Elevations of inflammatory and procoagulant biomarkers in elderly persons with renal insufficiency. Circulation 2003, 107, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Nattel, S.; Burstein, B.; Dobrev, D. Atrial remodeling and atrial fibrillation: Mechanisms and implications. Circ. Arrhythm. Electrophysiol. 2008, 1, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Bansal, N.; Xie, D.; Tao, K.; Chen, J.; Deo, R.; Horwitz, E.; Hsu, C.; Kallem, R.K.; Keane, M.G.; Lora, C.M.; et al. Atrial Fibrillation and Risk of ESRD in Adults with CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 1189–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney Disease as a Risk Factor for Development of Cardiovascular Disease: A Statement From the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108, 2154–2169. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Lopez, F.L.; Matsushita, K.; Loehr, L.R.; Agarwal, S.K.; Chen, L.Y.; Soliman, E.Z.; Astor, B.C.; Coresh, J. Chronic Kidney Disease Is Associated with the Incidence of Atrial Fibrillation. Circulation 2011, 123, 2946–2953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, D.; Sood, M.M.; Rigatto, C.; Holden, R.M.; Hiremath, S.; Clase, C.M. Systematic review and meta-analysis of incidence, prevalence and outcomes of atrial fibrillation in patients on dialysis. Nephrol. Dial. Transplant. 2012, 27, 3816–3822. [Google Scholar] [CrossRef] [Green Version]
- Glorieux, G.; Cohen, G.; Jankowski, J.; Vanholder, R. Platelet/Leukocyte Activation, Inflammation, and Uremia. Semin. Dial. 2009, 22, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Boccardo, P.; Remuzzi, G.; Galbusera, M. Platelet Dysfunction in Renal Failure. Semin. Thromb. Hemost. 2004, 30, 579–589. [Google Scholar] [CrossRef]
- Caturano, A.; Galiero, R.; Pafundi, P.C. Atrial Fibrillation and Stroke. A Review on the Use of Vitamin K Antagonists and Novel Oral Anticoagulants. Medicina 2019, 55, 617. [Google Scholar] [CrossRef] [Green Version]
- Jain, N.; Reilly, R.F. Clinical Pharmacology of Oral Anticoagulants in Patients with Kidney Disease. Clin. J. Am. Soc. Nephrol. 2019, 14, 278–287. [Google Scholar] [CrossRef] [Green Version]
- Ansell, J.; Hirsh, J.; Hylek, E.; Jacobson, A.; Crowther, M.; Palareti, G. Pharmacology and Management of the Vitamin K Antagonists. Chest 2008, 133, 160S–198S. [Google Scholar] [CrossRef]
- Grove, E.L.; Skjøth, F.; Nielsen, P.B.; Christensen, T.D.; Larsen, T.B. Effectiveness and safety of self-managed oral anticoagulant therapy compared with direct oral anticoagulants in patients with atrial fibrillation. Sci. Rep. 2018, 8, 15805. [Google Scholar] [CrossRef]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Andò, G.; Capranzano, P. Non-vitamin K antagonist oral anticoagulants in atrial fibrillation patients with chronic kidney disease: A systematic review and network meta-analysis. Int. J. Cardiol. 2017, 231, 162–169. [Google Scholar] [CrossRef]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [Green Version]
- Dewald, T.A.; Becker, R.C. The pharmacology of novel oral anticoagulants. J. Thromb. Thrombolysis 2014, 37, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Kustos, S.; Fasinu, P. Direct-Acting Oral Anticoagulants and Their Reversal Agents—An Update. Medicines 2019, 6, 103. [Google Scholar] [CrossRef] [Green Version]
- Kanuri, S.H.; Kreutz, R.P. Pharmacogenomics of Novel Direct Oral Anticoagulants: Newly Identified Genes and Genetic Variants. J. Pers. Med. 2019, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Fawzy, A.M.; Lip, G.Y.H. Pharmacokinetics and pharmacodynamics of oral anticoagulants used in atrial fibrillation. Expert Opin. Drug Metab. Toxicol. 2019, 15, 381–398. [Google Scholar] [CrossRef] [PubMed]
- Gelosa, P.; Castiglioni, L.; Tenconi, M.; Baldessin, L.; Racagni, G.; Corsini, A.; Bellosta, S. Pharmacokinetic drug interactions of the non-vitamin K antagonist oral anticoagulants (NOACs). Pharmacol. Res. 2018, 135, 60–79. [Google Scholar] [CrossRef] [PubMed]
- Anghel, L.; Sascău, R.; Trifan, A.; Zota, I.M.; Stătescu, C. Non-Vitamin K Antagonist Oral Anticoagulants and the Gastrointestinal Bleeding Risk in Real-World Studies. J. Clin. Med. 2020, 9, 1398. [Google Scholar] [CrossRef] [PubMed]
- Marinigh, R.; Lane, D.A.; Lip, G.Y.H. Severe Renal Impairment and Stroke Prevention in Atrial Fibrillation. J. Am. Coll. Cardiol. 2011, 57, 1339–1348. [Google Scholar] [CrossRef] [Green Version]
- Vio, R.; Proietti, R.; Rigato, M.; Calò, L.A. Clinical Evidence for the Choice of the Direct Oral Anticoagulant in Patients with Atrial Fibrillation According to Creatinine Clearance. Pharmaceuticals 2021, 14, 279. [Google Scholar] [CrossRef]
- Stanifer, J.W.; Pokorney, S.D.; Chertow, G.M.; Hohnloser, S.H.; Wojdyla, D.M.; Garonzik, S.; Byon, W.; Hijazi, Z.; Lopes, R.D.; Alexander, J.H.; et al. Apixaban Versus Warfarin in Patients with Atrial Fibrillation and Advanced Chronic Kidney Disease. Circulation 2020, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.T.; Neuen, B.L.; Cheng, L.P.; Jun, M.; Toyama, T.; Gallagher, M.P.; Jardine, M.J.; Sood, M.M.; Garg, A.X.; Palmer, S.C.; et al. Benefits and harms of oral anticoagulant therapy in chronic kidney disease. Ann. Intern. Med. 2019, 171, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Siontis, K.C.; Zhang, X.; Eckard, A.; Bhave, N.; Schaubel, D.E.; He, K.; Tilea, A.; Stack, A.G.; Balkrishnan, R.; Yao, X.; et al. Outcomes associated with apixaban use in patients with end-stage kidney disease and atrial fibrillation in the United States. Circulation 2018, 138, 1519–1529. [Google Scholar] [CrossRef]
- Feldberg, J.; Patel, P.; Farrell, A.; Sivarajahkumar, S.; Cameron, K.; Ma, J.; Battistella, M. A systematic review of direct oral anticoagulant use in chronic kidney disease and dialysis patients with atrial fibrillation. Nephrol. Dial. Transplant. 2019, 34, 265–277. [Google Scholar] [CrossRef] [Green Version]
- Gorczyca, I.; Jelonek, O.; Uziębło-Życzkowska, B.; Chrapek, M.; Maciorowska, M.; Wójcik, M.; Błaszczyk, R.; Kapłon-Cieślicka, A.; Gawałko, M.; Budnik, M.; et al. Trends in the Prescription of Non-Vitamin K Antagonist Oral Anticoagulants for Atrial Fibrillation: Results of the Polish Atrial Fibrillation (POL-AF) Registry. J. Clin. Med. 2020, 9, 3565. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 104–132. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Cairns, J.A.; Mitchell, L.B.; Macle, L.; Stiell, I.G.; Gladstone, D.; McMurtry, M.S.; Connolly, S.; Cox, J.L.; Dorian, P.; et al. 2014 Focused Update of the Canadian Cardiovascular Society Guidelines for the Management of Atrial Fibrillation. Can. J. Cardiol. 2014, 30, 1114–1130. [Google Scholar] [CrossRef]
- Andrade, J.G.; Verma, A.; Mitchell, L.B.; Parkash, R.; Leblanc, K.; Atzema, C.; Healey, J.S.; Bell, A.; Cairns, J.; Connolly, S.; et al. 2018 Focused Update of the Canadian Cardiovascular Society Guidelines for the Management of Atrial Fibrillation. Can. J. Cardiol. 2018, 34, 1371–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; En Chiang, C.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Tirucherai, G.; Marbury, T.C.; Wang, J.; Chang, M.; Zhang, D.; Song, Y.; Pursley, J.; Boyd, R.A.; Frost, C. Pharmacokinetics, pharmacodynamics, and safety of apixaban in subjects with end-stage renal disease on hemodialysis. J. Clin. Pharmacol. 2016, 56, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.; Yu, Z.; Shenker, A.; Wang, J.; Pursley, J.; Byon, W.; Boyd, R.A.; LaCreta, F.; Frost, C.E. Effect of renal impairment on the pharmacokinetics, pharmacodynamics, and safety of apixaban. J. Clin. Pharmacol. 2016, 56, 637–645. [Google Scholar] [CrossRef]
- Kuno, T.; Takagi, H.; Ando, T.; Sugiyama, T.; Miyashita, S.; Valentin, N.; Shimada, Y.J.; Kodaira, M.; Numasawa, Y.; Briasoulis, A.; et al. Oral Anticoagulation for Patients with Atrial Fibrillation on Long-Term Hemodialysis. J. Am. Coll. Cardiol. 2020, 75, 273–285. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CKD | eGFR (mL/min/1.73 m2) | A1 < 30 mg/g | A2 30–300 mg/g | A3 > 300 mg/g |
|---|---|---|---|---|
| Stage 1 | >90 | A0 | A1 | A2 |
| Stage 2 | 60–89 | A0 | A1 | A2 |
| Stage 3a | 45–59 | A1 | A2 | A3 |
| Stage 3b | 30–44 | A2 | A3 | A3 |
| Stage 4 | 15–29 | A3 | A3 | A3 |
| Stage 5 | <15 | A3 | A3 | A3 |
| Clinical Trial | Author, Year | Study Population | Study Design | Results Primary Outcome: Stroke or Systemic Embolism (SSE) Safety Outcome: Major Bleeding or Clinically Relevant Major Bleeding |
|---|---|---|---|---|
| RE-LY | Connolly S. et al., 2009 [34] | n = 18,113; CHADS2 ≥ 1; 71 years, 64% men | Dabigatran 110 mg/150 mg twice a day compared to dose-adjusted warfarin 2 years follow-up | Dabigatran 110 mg was noninferior to warfarin with lower rate of ICH and other major hemorrhage; Dabigatran 150 mg was superior to warfarin with lower rate of ICH, similar rate of other major hemorrhage |
| ROCKET AF | Patel et al., 2011 [35] | n = 14,264; CHADS2 ≥ 2; 73 years, 60% men | Rivaroxaban 20 mg (15 mg in patients with moderate renal impairment) once a day compared to dose-adjusted warfarin | Rivaroxaban was noninferior to warfarin with lower rate of ICH, similar rate of other major hemorrhage The reduced dosage showed consistent results with 20 mg once daily in patients with normal renal function |
| ARISTOTLE | Granger et al., 2011 [36] | n = 18201; CHADS2 ≥ 1; 70 years, 65% men | Apixaban 5 mg (2.5 mg in patients with two or more dose-reduction criteria) twice a day compared to dose- adjusted warfarin | Apixaban was superior to warfarin with lower rate of ICH and lower rate of other major hemorrhage The treatment effect and major bleeding were consistent across all major subgroups |
| ENGAGE AF-TIMI 48 | Gugliano et al., 2013 [37] | n = 21,105; CHADS2 ≥ 2; 72 years, 62% men | Edoxaban 30 and 60 mg once a day compared to dose- adjusted warfarin | Both once-daily regimens of edoxaban were noninferior to warfarin with respect to the prevention of SSE and with significantly lower rates of bleeding side effects |
| Characteristics | Warfarin | Dabigatran | Rivaroxaban | Apixaban | Edoxaban |
|---|---|---|---|---|---|
| Mechanism of action | Inhibition of vitamin K dependent clotting factors (II, VII, IX, X) | Factor IIa (thrombin) inhibition | Factor Xa inhibition | Factor Xa inhibition | Factor Xa inhibition |
| Dosing | Variable (INR monitoring) QD | Fixed 150/110 mg BID | Fixed 20/15 mg QD | Fixed 5/2.5 mg BID | Fixed 60/30 mg QD |
| Protein binding | 99% | 35% | 90% | 87% | 40–59% |
| Metabolism | Extensive metabolism by CYP2C9 | Esterase mediated hydrolysis (no CYP450) | Metabolized in liver by CYP3A4/ 2J2 (65%) | Metabolized in liver by CYP3A4 (75%) | Metabolized in liver by CYP3A4 (50%) |
| Interactions | Multiple food-drug and drug-drug | P-gP | CYP3A4/2J2 P-gP | CYP3A4 P-gP | P-gP |
| Renal excretion | <1% | 80–85% | 35% | 25% | 50% |
| Cmax, hours | 72–96 | 1–2 | 2–4 | 3–4 | 1–2 |
| t½, hours | 40 | 12–14 | 6–13 | 12 | 10–14 |
| Dialyzable | No | Yes | No | Small | No |
| Antidote | Yes (Vitamin K) | Yes (Idarucizumab) | Yes (Andexanet alfa) | Yes (Andexanet alfa) | Under development |
| Recommendation in severe renal impairment (eGFR = 15–29 mL/min/1.73 m2) | Strict INR monitoring | Contraindicated (EU)/Dose adjustment (75 mg BID (US)) | Dose adjustment (15 mg QD) | Dose adjustment (15 mg QD in EU)/No action until at least 2 criteria fulfilled (age ≥ 80 y; weight ≤ 60 kg; creatinine ≥ 1.5 mg/dL) | Dose adjustment (30 mg QD) |
| Clinical Trial | Study Design/Enrollment | Methods | Inclusion Criteria | Primary and Secondary End-Point | Expected Completion/Results |
|---|---|---|---|---|---|
| RENAL-AF (NCT02942407) | 2016 Apixaban pharmacokinetics US, Multicenter (n = 762 patient target) | Open-label randomization to apixaban (5/2.5 mg) versus warfarin (INR 2–3) for up to 15 months | ≥18 years AF with CHA2DS2-VASc ≥ 2 ESRD on HD > 3 months OAT candidate | Time to first major or clinically relevant non-major bleeding Stroke or SE Mortality | August 2019 (154 patients enrolled at completion); Similar risks of bleeding and stroke in the 2 groups |
| AXADIA (NCT02933697) | 2017 Apixaban pharmacokinetics Germany, Multicenter (n = 222 patient target) | Open-label randomization to apixaban (2.5 mg) versus phenprocoumon (INR 2–3) for 6–24 months | ≥18 years AF with CHA2DS2-VASc ≥ 2 ESRD on HD > 3 months OAT candidate | Time to first major or clinically relevant non-major bleeding Thromboembolism | July 2022 (Recruiting) |
| AVKDIAL (NCT02886962) | 2017 University Hospital of Strasbourg, France, Multicenter (n = 855 patient target) | Open-label randomization to VKA (INR 2–3) versus no OAT for 24 months | ≥18 years AF with CHA2DS2-VASc ≥ 2 ESRD on HD > 1 months OAT candidate | Cumulative incidence of severe bleeding events and thrombosis | January 2023 Recruiting |
| SAFE-D (NCT03987711) | 2019 Unity Health Toronto, Multicenter (n = 150 patient target) | Open-label randomization to apixaban (5/2.5 mg) versus warfarin (INR 2–3) versus no OAT for 26 weeks | ≥18 years AF with CHA2DS2-VASc ≥ 2 ESRD on HD > 90 days OAT candidate | AF related stroke and SE; risk of bleeding and all-cause mortality | December 2021 Recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoica, M.C.; Gáll, Z.; Gliga, M.L.; Căldăraru, C.D.; Székely, O. Oral Anticoagulant Treatment in Patients with Atrial Fibrillation and Chronic Kidney Disease. Medicina 2021, 57, 422. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050422
Stoica MC, Gáll Z, Gliga ML, Căldăraru CD, Székely O. Oral Anticoagulant Treatment in Patients with Atrial Fibrillation and Chronic Kidney Disease. Medicina. 2021; 57(5):422. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050422
Chicago/Turabian StyleStoica, Mihai Ciprian, Zsolt Gáll, Mirela Liana Gliga, Carmen Denise Căldăraru, and Orsolya Székely. 2021. "Oral Anticoagulant Treatment in Patients with Atrial Fibrillation and Chronic Kidney Disease" Medicina 57, no. 5: 422. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050422