
Heterotopic Quadruplet Pregnancy. Literature Review and Case Report

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
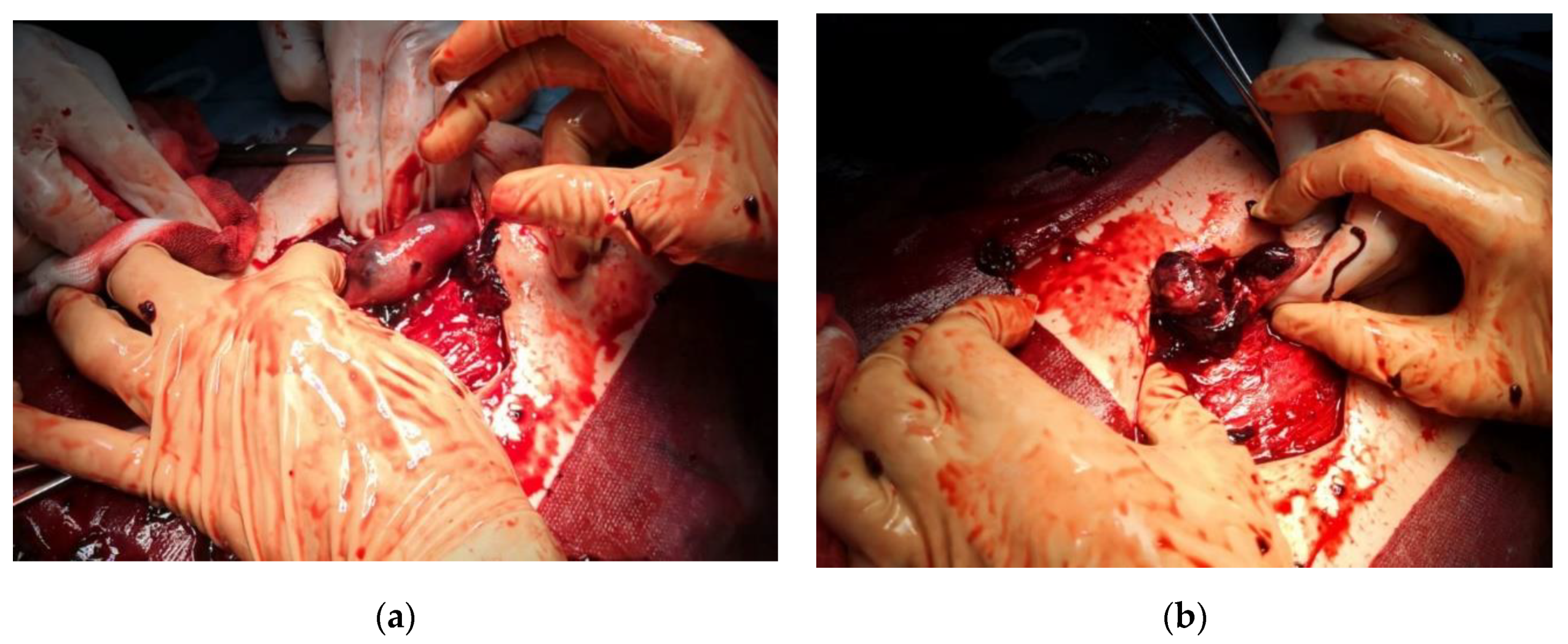
4. Case Presentation
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luo, X.; Lim, C.E.; Huang, C.; Wu, J.; Wong, W.S.; Cheng, N.C. Heterotopic pregnancy following in vitro fertilization and embryo transfer: 12 cases report. Arch. Gynecol. Obstet. 2009, 280, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Chin, H.Y.; Chen, F.P.; Wang, C.J.; Shui, L.T.; Liu, Y.H.; Soong, Y.K. Heterotopic pregnancy after in-vitro fertilization–embryo transfer. Int. J. Gynecol. Obstet. 2004, 86, 411–416. [Google Scholar] [CrossRef]
- Reece, E.A.; Petrie, R.H.; Sirmans, M.F.; Finster, M.; Todd, W.D. Combined intrauterine and extrauterine gestations: A review. Am. J. Obstet. Gynecol. 1983, 146, 323–330. [Google Scholar] [CrossRef]
- Refaat, B.; Dalton, E.; Ledger, W.L. Ectopic pregnancy secondary to in vitro fertilization-embryo transfer: Pathogenic mechanisms and management strategies. Reprod. Biol. Endocrinol. 2015, 13, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.R.; Moon, M.J.; Ahn, E.H.; Baek, M.J.; Cho, H.D. Case report. Heterotopic quadruplet pregnancy: Conservative managment with ultrasonographically-guided KCl injection of cornual pregnancy and laparoscopic operation of tubal pregnancy. Fetal. Diagn. Ther. 2009, 26, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.; Lee, J.N.; Yang, C.H.; Hsu, S.C.; Tsai, E.M. Case report. An unexpected quadruplet heterotopic pregnancy after bilateral salpingectomy and replacement of three embryos. Fertil. Steril. 2003, 80, 218–220. [Google Scholar] [CrossRef]
- Tamhane, N.A.; Parikh, A.; Joshi, V.M. Heterotopic Quadruplet Pregnancy After ICSI Conception. J. Obstet. Gynaecol. India 2018, 68, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.; Duarte, C.; Oliveira, P.; Andrade, A.; Furtado, J. Heterotopic Quadruplet Gestation after Uncontrolled Ovulation Induction: A Case Report. J. Preg. Child. Health 2019, 6. [Google Scholar] [CrossRef]
- Omosh, R.K.; Fayez, I.A.; Alfayez, N.D.; Karaki, M.M.A. Quadruplet Heterotopic Pregnancy: A Case Report. Jordan Int. Med. 2017, 63, 1–3. [Google Scholar] [CrossRef]
- Uysal, F.; Uysal, A.; Oztekin, D.C.; Avcı, M.S. Heterotopic quadruplet pregnancy and successful twin outcome. Arch. Gynecol. Obstet. 2013, 288, 715–717. [Google Scholar]
- Sherer, D.M.; Scibetta, J.J.; Sanko, S.R. Heterotopic quadruplet gestation with laparoscopic resection of ruptured interstitial pregnancy and subsequent successful outcome of triplets. Am. J. Obstet. Gynecol. 1995, 172, 216–217. [Google Scholar] [CrossRef]
- Aguemon, C.T.; Denakpo, J.; Hounkpatin, B.B.; Tossa, L.B.; Adisso, S.; Sacca, J.; de Souza, J. Heterotopic pregnancy in the University Clinic of Gynecology and Obstetrics of the National Hospital and University of Benin Hubert Maga Koutoukou: Report of a case of quadruple pregnancy; 3 fetal intrauterine and 1 abdominal fetal. Pan Afr. Med. J. 2015, 22, 394. [Google Scholar]
- Lavanya, R.; Deepika, K.; Patil, K. Successful pregnancy following medical management of heterotopic pregnancy. J. Hum. Reprod. Sci. 2009, 2, 35–40. [Google Scholar] [CrossRef]
- Habana, A.; Dokras, A.; Giraldo, J.L.; Jones, E.E. Cornual heterotpic pregnancy: Contemporary management options. Am. J. Obstet. Gynecol. 2000, 182, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Siraj, S.H.M.; Wee-Stekly, W.W.; Chern, B.S.M. Heterotopic pregnancy in a natural conception cycle presenting as acute abdomen: A case report and literature review. Gynecol. Minim. Invasive Ther. 2014, 3, 100–102. [Google Scholar] [CrossRef] [Green Version]
- Sentilhes, L.; Bouet, P.E.; Gromez, A.; Poilblanc, M.; Lefebvre-Lacoeuille, C.; Descamps, P. Successful expectant management for a cornual heterotopic pregnancy. Fertil. Steril. 2009, 91, 934.e11–934.e13. [Google Scholar] [CrossRef] [PubMed]
- Kwon, B.; Kang, S.; Lee, H.J.; Kim, M.; Lee, Y.H.; Im, J.; Moon, M.J.; Ahn, E.H.; Kim, Y.R. Non-surgical management and obstetric outcomes of heterotopic interstitial pregnancies. Minim. Invasive Ther. Allied Technol. 2020, 29, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Guideline of the European Society of Human Reproduction and Embryology ESHRE. Guideline Group on Good Practice in IVF Labs. December 2015. Available online: https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Revised-guidelines-for-good-practice-in-IVF-laboratories-(2015).aspx (accessed on 28 March 2021).
- Gica, N.; Gana, N.; Mat, C.; Panaitescu, A.M.; Peltecu, G.; Vayna, A.M. Conjoined twins-early prenatal diagnosis. J. Obstet. Gynaecol. 2020, 40, 723–724. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Age (y) | Past History | GA(w) | Method | Intrauterine | Ectopic | Symptoms | Intervention | Obstetric Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Park HR [5] | 30 | None | NA | NA | Twins | Cornual and tubal | NA | -cornual pregnancy: US guided transvaginal injection of KCl -tubal pregnancy laparoscopy | Elective CS at 37 w twins |
| Chan [6] | 31 | bilateral salpingectomy | 7 | IVF | Twins | interstitial twins | painless vaginal spotting 35 days after ET | Laparotomy | Elective CS at 38 w twins |
| Tamhane NA [7] | 32 | Medically managed ectopic pregnancy | 10 | ICSI | TCTA triplets | Tubal | abdominal pain, vaginal spotting | -10 weeks: Tubal pregnancy- laparotomy -12 weeks: ER triplets to twins | CS after PPROM at 34 w twins |
| Soares A [8] | 31 | Primary infertility | 9 | Ovulation induction | Triplets only 1 viable | Tubal | abdominal pain | Laparotomy | Term delivery singleton-agenesis of one distal phalanx of the hand and agenesis of distal phalanges of all toes |
| Omosh RK [9] | 20 | Primary infertility | 10 | Ovulation induction + IUI | Triplets | Tubal | abdominal pain | Laparotomy | NA pregnancy outcome; at 23 weeks all 3 viable |
| Uysal F [10] | 30 | Primary infertility | 7 | IUI | Triplets | Tubal | abdominal pain | -7 weeks: Laparoscopy -13 weeks: 1 spontaneous fetal loss | Elective CS at 37 w twins |
| Sherer DM [11] | 32 | Unremarkable | 8 | IVF | Triplets | Interstitial | abdominal pain, anemia, marked weakness, and right shoulder pain | Laparoscopy | CS after PPROM at 33 w triplets |
| Aguemon CT [12] | 22 | Unremarkable | 34 | Spontaneous | TCTA triplets | Abdominal | severe preeclampsia + periumbilical pain | Laparotomy and CS -abdominal: Multiple malformation alive; + administration of methotrexate -livebirth of TCTA triplets | 3 Neonatal deaths, 1 survivor Maternal heart failure- 6 months F/U stable |
| Lavanya R [13] | NA | Primary infertility | 12 | Ovulation induction | Twins | Twins | abdominal pain, vaginal bleed | None viable intrauterine twin + methotrexate | None |
| Our case | 35 | Primary infertility | 10 | Ovulation induction + IVF | TCTA triplets | tubal | abdominal pain | Laparotomy 12 weeks: Only 2 fetus alive | CS after PPROM at 35 w twins |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimpoca, B.; Moldoveanu, A.; Gică, N.; Gică, C.; Ciobanu, A.M.; Panaitescu, A.M.; Oprescu, D. Heterotopic Quadruplet Pregnancy. Literature Review and Case Report. Medicina 2021, 57, 483. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050483
Cimpoca B, Moldoveanu A, Gică N, Gică C, Ciobanu AM, Panaitescu AM, Oprescu D. Heterotopic Quadruplet Pregnancy. Literature Review and Case Report. Medicina. 2021; 57(5):483. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050483
Chicago/Turabian StyleCimpoca, Brîndușa, Amira Moldoveanu, Nicolae Gică, Corina Gică, Anca Marina Ciobanu, Anca Maria Panaitescu, and Dana Oprescu. 2021. "Heterotopic Quadruplet Pregnancy. Literature Review and Case Report" Medicina 57, no. 5: 483. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050483