
Second Primary Tumors in Patients with Gastrointestinal Stromal Tumors: A Single-Center Experience

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Patients
3.2. Features of GISTs
3.2.1. Symptomatology
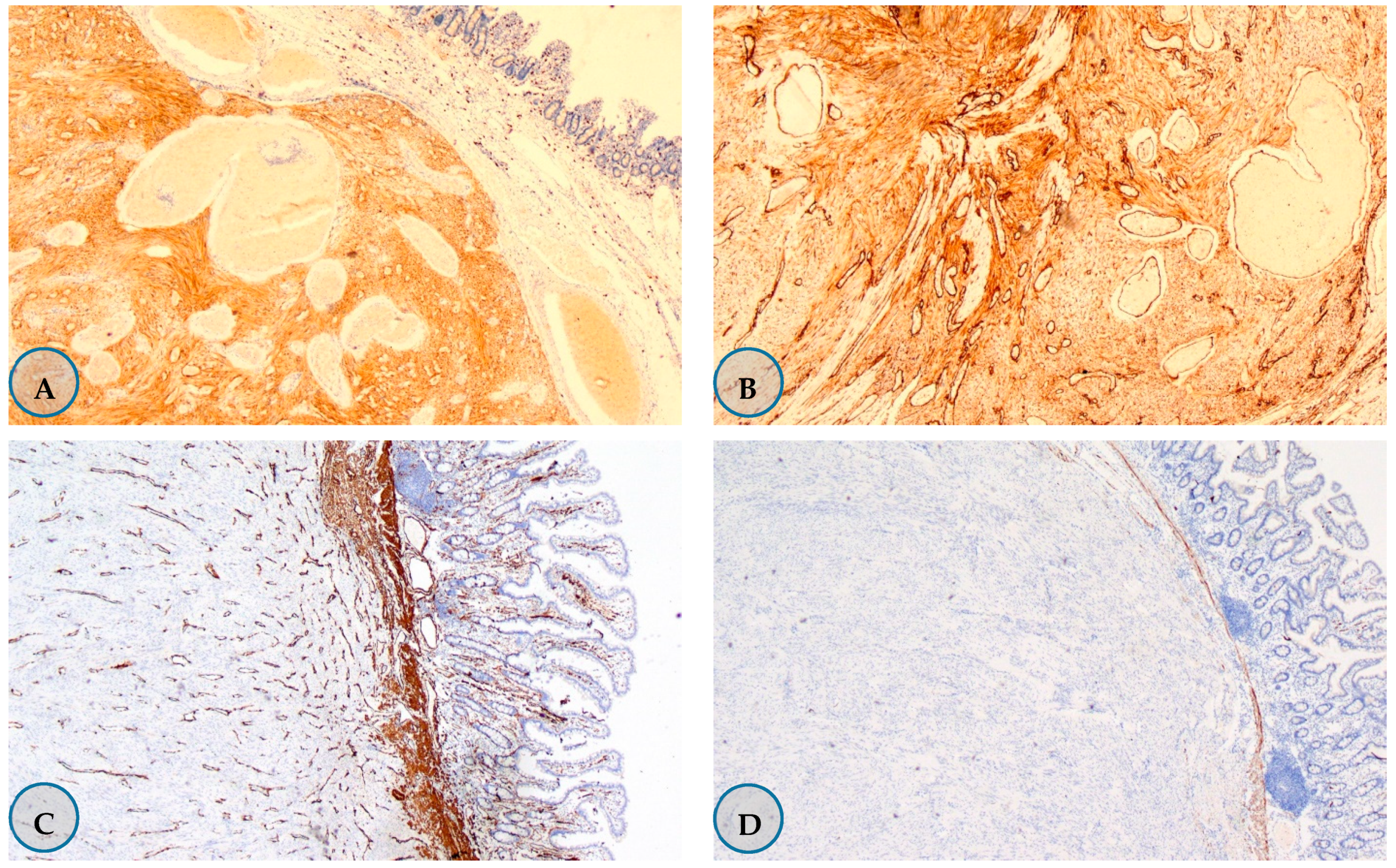
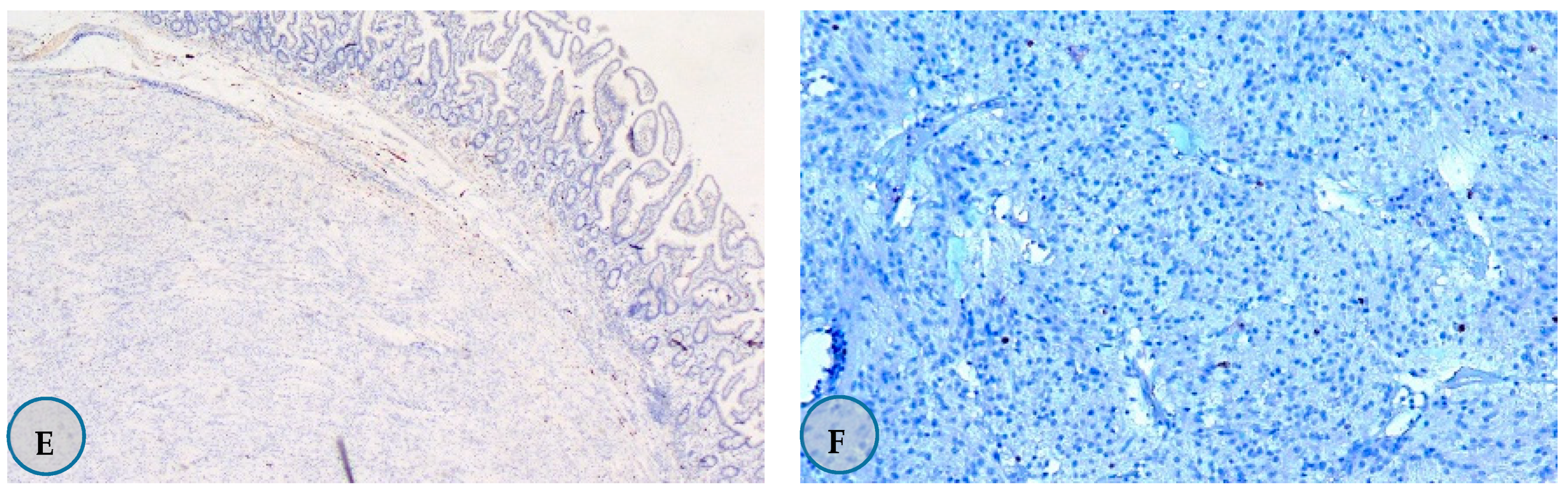
3.2.2. Pathological Tumor Features
3.2.3. Localization of the Tumors
3.2.4. Tumor Stage-Recurrence Risk
3.2.5. Treatment
3.3. SPMT Features
3.4. GIST-SPMT Emergence Time Relationship
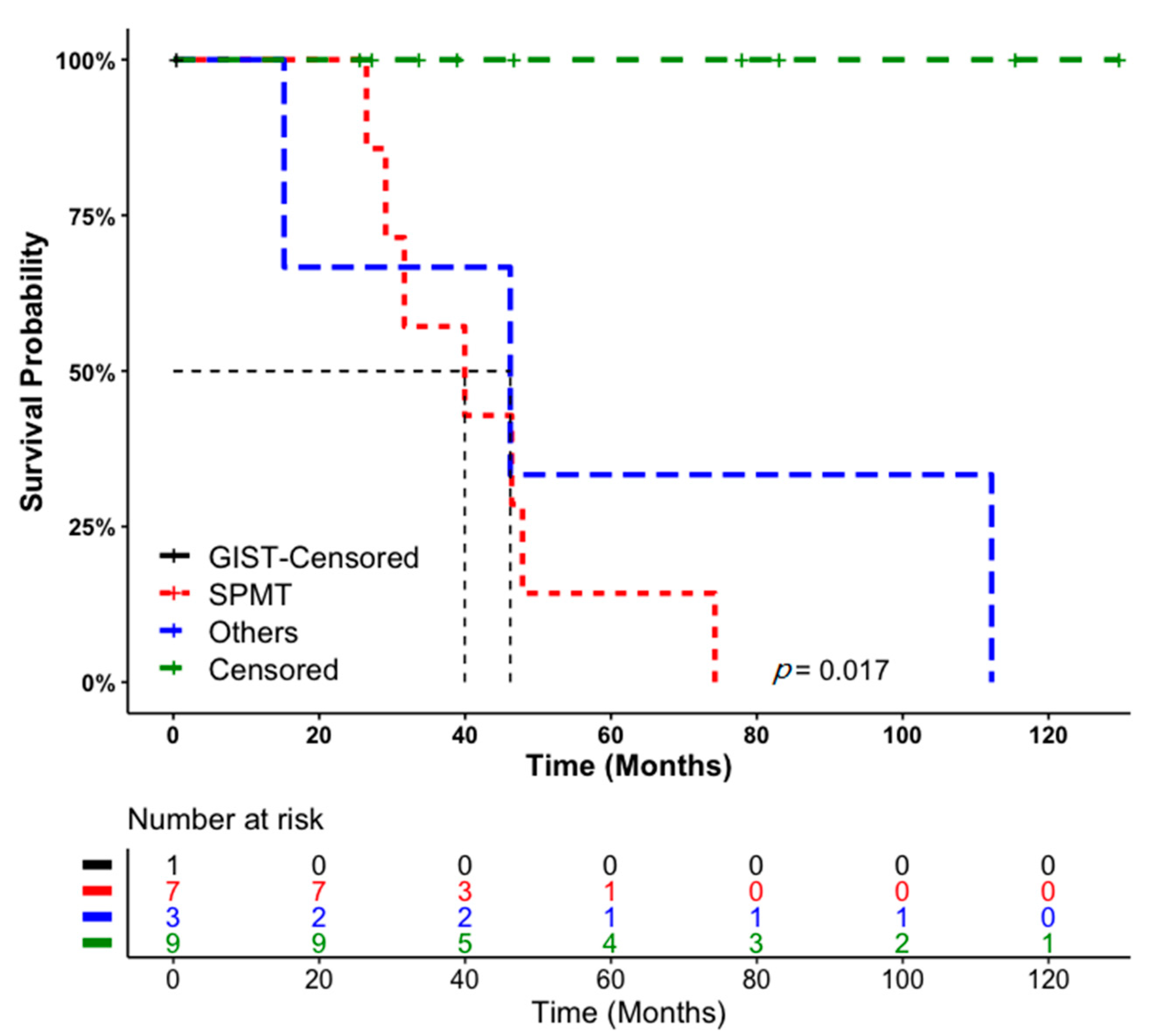
3.5. Patient Follow-Up and Survival Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed consent statement
Data Availability Statement
Conflicts of Interest
References
- Núñez-Martín, R.; Cervera, R.C.; Pulla, M.P. El tumor del estroma gastrointestinal y la aparición de segundos tumores: Revisión de la bibliografía. Med. Clínica 2017, 149, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Søreide, K.; Sandvik, O.M.; Søreide, J.A.; Giljaca, V.; Jureckova, A.; Bulusu, V.R. Global epidemiology of gastrointestinal stromal tumours (GIST): A systematic review of population-based cohort studies. Cancer Epidemiol. 2016, 40, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Miettinen, M.; Lasota, J. Gastrointestinal stromal tumors (GISTs): Definition, occurrence, pathology, differential diagnosis and molecular genetics. Pol. J. Pathol. 2003, 54, 3–24. [Google Scholar] [PubMed]
- Ahmed, M. Recent advances in the management of gastrointestinal stromal tumor. World J. Clin. Cases 2020, 8, 3142–3155. [Google Scholar] [CrossRef]
- Steigen, S.E.; Eide, T.J. Gastrointestinal stromal tumors (GISTs): A review. APMIS 2009, 117, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Gronchi, A.; Hohenberger, P.; Bonvalot, S.; Schöffski, P.; Bauer, S.; Fumagalli, E.; Nyckowski, P.; Nguyen, B.-P.; Kerst, J.M.; et al. Neoadjuvant Imatinib in Locally Advanced Gastrointestinal Stromal Tumors (GIST): The EORTC STBSG Experience. Ann. Surg. Oncol. 2013, 20, 2937–2943. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, H.; Eriksson, M.; Hall, K.S.; Hartmann, J.T.; Pink, D.; Schütte, J.; Ramadori, G.; Hohenberger, P.; Duyster, J.; Al-Batran, S.-E.; et al. One vs Three Years of Adjuvant Imatinib for Operable Gastrointestinal Stromal Tumor. JAMA 2012, 307, 1265–1272. [Google Scholar] [CrossRef] [Green Version]
- Blanke, C.D.; Demetri, G.D.; Von Mehren, M.; Heinrich, M.C.; Eisenberg, B.; Fletcher, J.A.; Corless, C.L.; Fletcher, C.D.M.; Roberts, P.J.; Heinz, D.; et al. Long-Term Results from a Randomized Phase II Trial of Standard- Versus Higher-Dose Imatinib Mesylate for Patients with Unresectable or Metastatic Gastrointestinal Stromal Tumors Expressing KIT. J. Clin. Oncol. 2008, 26, 620–625. [Google Scholar] [CrossRef]
- Agaimy, A.; Wünsch, P.H.; Sobin, L.H.; Lasota, J.; Miettinen, M. Occurrence of other malignancies in patients with gastrointestinal stromal tumors. Semin. Diagn. Pathol. 2006, 23, 120–129. [Google Scholar] [CrossRef]
- Gonçalves, R.; Linhares, E.; Albagli, R.; Valadão, M.; Vilhena, B.; Romano, S.; Gil Ferreira, C. Occurrence of other tumors in patients with GIST. Surg. Oncol. 2010, 19, e140–e143. [Google Scholar] [CrossRef]
- Waidhauser, J.; Bornemann, A.; Trepel, M.; Märkl, B. Frequency, localization, and types of gastrointestinal stromal tumor-associated neoplasia. World J. Gastroenterol. 2019, 25, 4261–4277. [Google Scholar] [CrossRef]
- Petrelli, F.; Tomasello, G.; Barni, S.; Varricchio, A.; Costanzo, A.; Rampulla, V.; Cabiddu, M.; Turati, L.; Russo, A.; Seghezzi, S.; et al. Risk of second primary tumors in GIST survivors: A systematic review and meta-analysis. Surg. Oncol. 2019, 29, 64–70. [Google Scholar] [CrossRef]
- Smith, M.J.; Smith, H.G.; Mahar, A.L.; Law, C.; Ko, Y.-J. The impact of additional malignancies in patients diagnosed with gastrointestinal stromal tumors. Int. J. Cancer 2016, 139, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Rodriquenz, M.G.; Rossi, S.; Ricci, R.; Martini, M.; Larocca, M.; Dipasquale, A.; Quirino, M.; Schinzari, G.; Basso, M.; D’Argento, E.; et al. Gastrointestinal stromal tumors (GISTs) and second malignancies. Medicine 2016, 95, e4718. [Google Scholar] [CrossRef]
- Vassos, N.; Agaimy, A.; Hohenberger, W.; Croner, R.S. Coexistence of gastrointestinal stromal tumours (GIST) and malignant neoplasms of different origin: Prognostic implications. Int. J. Surg. 2014, 12, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sevinc, A.; Seker, M.; Bilici, A.; Ozdemir, N.Y.; Yildiz, R.; Ustaalioglu, B.O.; Kalender, M.E.; Dane, F.; Karaca, H.; Gemici, C.; et al. Co-existence of gastrointestinal stromal tumors with other primary neoplasms. Hepatogastroenterology 2011, 58, 824–830. [Google Scholar]
- Wronski, M.; Ziarkiewicz-Wroblewska, B.; Gornicka, B.; Cebulski, W.; Slodkowski, M.; Wasiutynski, A.; Krasnodebski, I.W. Synchronous occurrence of gastrointestinal stromal tumors and other primary gastrointestinal neoplasms. World J. Gastroenterol. 2006, 12, 5360–5362. [Google Scholar] [CrossRef] [PubMed]
- Kramer, K.; Wolf, S.; Mayer, B.; Schmidt, S.; Agaimy, A.; Henne-Bruns, D.; Knippschild, U.; Schwab, M.; Schmieder, M. Frequence, spectrum and prognostic impact of additional malignancies in patients with gastrointestinal stromal tumors. Neoplasia 2015, 17, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Comandini, D.; Grassi, M.; Prelaj, A.; Martelli, V.; Damiani, A.; Damiano, G.; Rebuzzi, S.E. Gastrointestinal stromal tumors and second primary malignancies: A retrospective monocentric analysis. Neoplasma 2021, 67, 1416–1423. [Google Scholar] [CrossRef]
- Podda, M.; Ferraro, G.; Di Saverio, S.; Cois, A.; Nardello, O.; Poillucci, G.; Marino, M.V.; Pisanu, A. Association Between Gastrointestinal Stromal Tumors and Other Malignancies: It Is Only a Matter of Time? A Case Series and an Overview of Systematic Reviews. J. Gastrointest. Cancer 2020, 51, 914–924. [Google Scholar] [CrossRef]
- Du, J.; Shen, N.; He, H.-S.; Fu, X.-L.; Wang, J.-Z.; Mao, C.-Z. Synchronous gastrointestinal cancer and gastrointestinal stromal tumors: A single-institution experience. World J. Surg. Oncol. 2016, 14, 130. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.D.; Ma, G.L.; Baumgartner, J.M.; Madlensky, L.; Burgoyne, A.M.; Tang, C.-M.; Martinez, M.E.; Sicklick, J.K. Increased risk of additional cancers among patients with gastrointestinal stromal tumors: A population-based study. Cancer 2015, 121, 2960–2967. [Google Scholar] [CrossRef] [PubMed]
- Mayr, P.; Märkl, B.; Agaimy, A.; Kriening, B.; Dintner, S.; Schenkirsch, G.; Schneider-Stock, R. Malignancies associated with GIST: A retrospective study with molecular analysis of KIT and PDGFRA. Langenbeck’s Arch. Surg. 2019, 404, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, J.; Bonetti, A. The Occurrence of Gastrointestinal Stromal Tumors and Second Malignancies. J. Gastrointest. Cancer 2015, 46, 408–412. [Google Scholar] [CrossRef]
- Hechtman, J.F.; DeMatteo, R.; Nafa, K.; Chi, P.; Arcila, M.E.; Dogan, S.; Oultache, A.; Chen, W.; Hameed, M. Additional Primary Malignancies in Patients with Gastrointestinal Stromal Tumor (GIST): A Clinicopathologic Study of 260 Patients with Molecular Analysis and Review of the Literature. Ann. Surg. Oncol. 2015, 22, 2633–2639. [Google Scholar] [CrossRef] [Green Version]
- Pandurengan, R.K.; Dumont, A.G.; Araujo, D.M.; Ludwig, J.A.; Ravi, V.; Patel, S.; Garber, J.; Benjamin, R.S.; Strom, S.S.; Trent, J.C. Survival of patients with multiple primary malignancies: A study of 783 patients with gastrointestinal stromal tumor. Ann. Oncol. 2010, 21, 2107–2111. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.S.; Werutsky, G.; Toneto, M.G.; Alves, J.M.; Piantá, C.D.; Breunig, R.C.; da Rocha, A.B.; Grivicich, I.; Garicochea, B. Synchronous gastrointestinal stromal tumors (GIST) and other primary cancers: Case series of a single institution experience. Int. J. Surg. 2010, 8, 314–317. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-J.; Yang, Z.; Hao, L.-S.; Xia, L.; Jia, Q.-B.; Wu, X.-T. Synchronous incidental gastrointestinal stromal and epithelial malignant tumors. World J. Gastroenterol. 2009, 15, 2027–2031. [Google Scholar] [CrossRef] [PubMed]
- Diamantis, A.; Bouliaris, K.; Christodoulidis, G.; Vasdeki, D.; Perivoliotis, K.; Tepetes, K. Gastrointestinal stromal tumors and synchronous intra-abdominal malignancies: Review of the literature. J. BUON Off. J. Balk. Union Oncol. 2019, 23, 1573–1579. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 20 (%) | |
|---|---|
| Age | |
| Mean Age ± SD | 63.8 ± 10.81 |
| Median age (years) | 68 (39–77) |
| Sex | |
| Male | 10 (50) |
| Female | 10 (50) |
| Symptomatology | |
| Asymptomatic | 13 (65) |
| Obstruction of small bowel | 1 (5) |
| Perforation of the small bowel | 1 (5) |
| Abdominal pain | 1 (5) |
| Mass in the abdomen | 1 (5) |
| Abdominal pain + abdominal mass | 1 (5) |
| Dyspeptic complaints (heartburn, nausea, vomiting, bloating) | 2 (10) |
| Treatment | |
| Yes | 19 (95) |
| Surgery (R0/R1) | 18 (90) (100/0) |
| Neoadjuvant therapy | 1 (5) |
| Adjuvant therapy | 0 (0) |
| No | 1 (5) |
| Tumor Characteristics | n = 20 (%) | |
|---|---|---|
| Tm diameter (cm) | ≤2 | 10 (50) |
| >2, ≤5 | 5 (25) | |
| >5, ≤10 | 1 (5) | |
| >10 | 4 (20) | |
| Mitosis rate (HPF) | ≤5/50 | 17 (85) |
| >5/50 | 3 (15) | |
| Ki-67 (Unknown/0–9/≥10) | 3/15/2 (15/75/10) | |
| Rupture (Yes/No/Unknown) | 0/20/0 (0/100/0) | |
| Necrosis (Yes/No/Unknown) | 3/11/6 (15/55/30) | |
| Ulceration (Yes/No/Unknown) | 2/10/8 (10/50/40) | |
| Cell type (Spindle/Epithelioid/Mixt (Spindle + Epithelioid)/Unknown) | 15/0/1/4 (75/0/5/20) | |
| Immunohistochemical Staining Properties | C Kit (Positive/Negative/Unknown) | 20/0/0 (100/0/0) |
| CD 34 (Positive/Negative/Unknown) | 16/2/2 (80/10/10) | |
| SMA (Positive/Negative/Unknown) | 3/12/5 (15/60/25) | |
| Desmin (Positive/Negative/Unknown) | 2/9/9 (10/45/45) | |
| S-100 (Positive/Negative/Unknown) | 0/13/7 (0/65/35) | |
| Recurrence risk (n = 19) | AFIP (None/Very low/Low/Medium/High) | 10/2/2/2/3 (50/10/10/10/15) |
| Modified NIH (Very low/Low/Mid/High) | 10/4/0/5 (50/20/0/25) | |
| Localization | Esophagogastric | 1 (5) |
| Stomach | 12 (60) | |
| Small intestine | 5 (25) | |
| Small intestine + Stomach | 1 (5) | |
| Extragastrointestinal | 1 (5) | |
| Stage (TNM) | 1 | 14 (70) |
| 2 | 2 (10) | |
| 3 | 3 (15) | |
| 4 | 1 (5) | |
| Patients | Gastrointestinal Stromal Tumor | Second Primary Malign Tumor | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | M/F | Age (y) | Localization | Symptom | TD (cm) | M (HPF) | Risk | Localization | Histological Type | Time of Diagnosis (from GIST) | Stage | Last Status | |
| AFIP | MNIH | ||||||||||||
| 1 | M | 77 | GO | Asymptomatic | 0.70 | ≤5/50 | NO | VL | Stomach | Adenocarcinoma -TPT | Synchronous | 2 | SPMT-EX |
| 2 | M | 70 | Stomach | Asymptomatic | 0.50 | ≤5/50 | NO | VL | Stomach | Adenocarcinoma | Synchronous | 3 | SPMT-EX |
| 3 | F | 61 | Stomach | A.P + M.A | 19.40 | ≤5/50 | Middle | High | Lung | Adenocarcinoma | 50 m later | 3 | SPMT-EX |
| 4 | M | 67 | S.I | A.P | 2.50 | ≤5/50 | Low | Low | Skin | SCC in situ | 82 m later | 0 | Alive |
| 5 | F | 75 | Stomach | D.Complaints | 5.00 | ≤5/50 | VL | Low | Thyroid | Papillary carcinoma | 273 m before | L | NT-EX |
| 6 | F | 51 | Stomach | Asymptomatic | 3.00 | ≤5/50 | VL | Low | Rectum | Carcinoma in situ | 100 m later | 0 | Alive |
| 7 | F | 74 | Stomach + S.I | Asymptomatic | 0.40 | ≤5/50 | NO | VL | Stomach | SRCC.Carcinoma | Synchronous | 3 | SPMT-EX |
| 8 | M | 72 | Stomach | Asymptomatic | 1.00 | ≤5/50 | NO | VL | Pancreas | Adenocarcinoma | Synchronous | 1 | SPMT-EX |
| 9 | F | 41 | S.I | Asymptomatic | 6.50 | ≤5/50 | Middle | High | Breast | DCIS | 40 m later | 0 | Alive |
| 10 | F | 61 | Stomach | Asymptomatic | 1.50 | ≤5/50 | NO | VL | D.C | Adenocarcinoma | Synchronous | 3 | Alive |
| 11 | F | 71 | S.I | E.O | 11.00 | ≤5/50 | High | High | Rectum | Adenocarcinoma | 45 m later | 4 | SPMT-EX |
| 12 | M | 61 | Stomach | Asymptomatic | 0.70 | ≤5/50 | NO | VL | Stomach | Adenocarcinoma-SRCC | Synchronous | 2 | NT-EX |
| 13 | F | 62 | S.I | E.O | 5.00 | >5/50 | High | High | Breast | Invasive carcinoma | 29 m later | 1 | Alive |
| 14 | M | 70 | S.I | Asymptomatic | 3.50 | ≤5/50 | Low | Low | D.C | Adenocarcinoma | Synchronous | 2 | Alive |
| 15 | M | 74 | Stomach | Asymptomatic | 0.50 | ≤5/50 | NO | VL | Sigmoid | M. Adenocarcinoma | 36 m before | 2 | Alive |
| 16 | M | 69 | Stomach | Asymptomatic | 0.40 | ≤5/50 | NO | VL | H.F | M. Adenocarcinoma | Synchronous | 2 | Alive |
| 17 | M | 69 | Stomach | D.Complaints | 11.90 | >5/50 | High | High | B.M | Multiple Myeloma | 7 m later | E | NT-EX |
| 18 | M | 54 | Stomach | Asymptomatic | 0.70 | ≤5/50 | NO | VL | Sigmoid | Adenocarcinoma | Synchronous | 4 | SPMT-EX |
| 19 | F | 39 | EG | M.A | 18.00 | >5/50 | Met. | Met. | Breast | Invasive carcinoma | 47 m before | 3 | GIST-EX |
| 20 | F | 58 | Stomach | Asymptomatic | 0.50 | ≤5/50 | NO | VL | Ovary | Serous carcinoma | Synchronous | 1 | Alive |
| n = 20 (%) | |
|---|---|
| Mean follow-up time ± SD | 45.6 months ± 34.1 |
| Final situation | |
| Alive | 9 (45) |
| Expired | 11 (55) |
| Due to GIST | 1 (5) |
| Due to SPMT | 7 (35) |
| Non-tumor-related | 3 (15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koçer, M.; Muallaoğlu, S.; Çetin, B.; Coşkun, H.Ş.; Karahan, N.; Gürdal, O. Second Primary Tumors in Patients with Gastrointestinal Stromal Tumors: A Single-Center Experience. Medicina 2021, 57, 494. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050494
Koçer M, Muallaoğlu S, Çetin B, Coşkun HŞ, Karahan N, Gürdal O. Second Primary Tumors in Patients with Gastrointestinal Stromal Tumors: A Single-Center Experience. Medicina. 2021; 57(5):494. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050494
Chicago/Turabian StyleKoçer, Murat, Sadık Muallaoğlu, Bülent Çetin, Hasan Şenol Coşkun, Nermin Karahan, and Osman Gürdal. 2021. "Second Primary Tumors in Patients with Gastrointestinal Stromal Tumors: A Single-Center Experience" Medicina 57, no. 5: 494. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050494