
Comparison of Postoperative Adjuvant Chemotherapy and Concurrent Chemoradiotherapy for FIGO2018 Stage IIIC1 Cervical Cancer: A Retrospective Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.2.1. CCRT
2.2.2. Chemotherapy
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
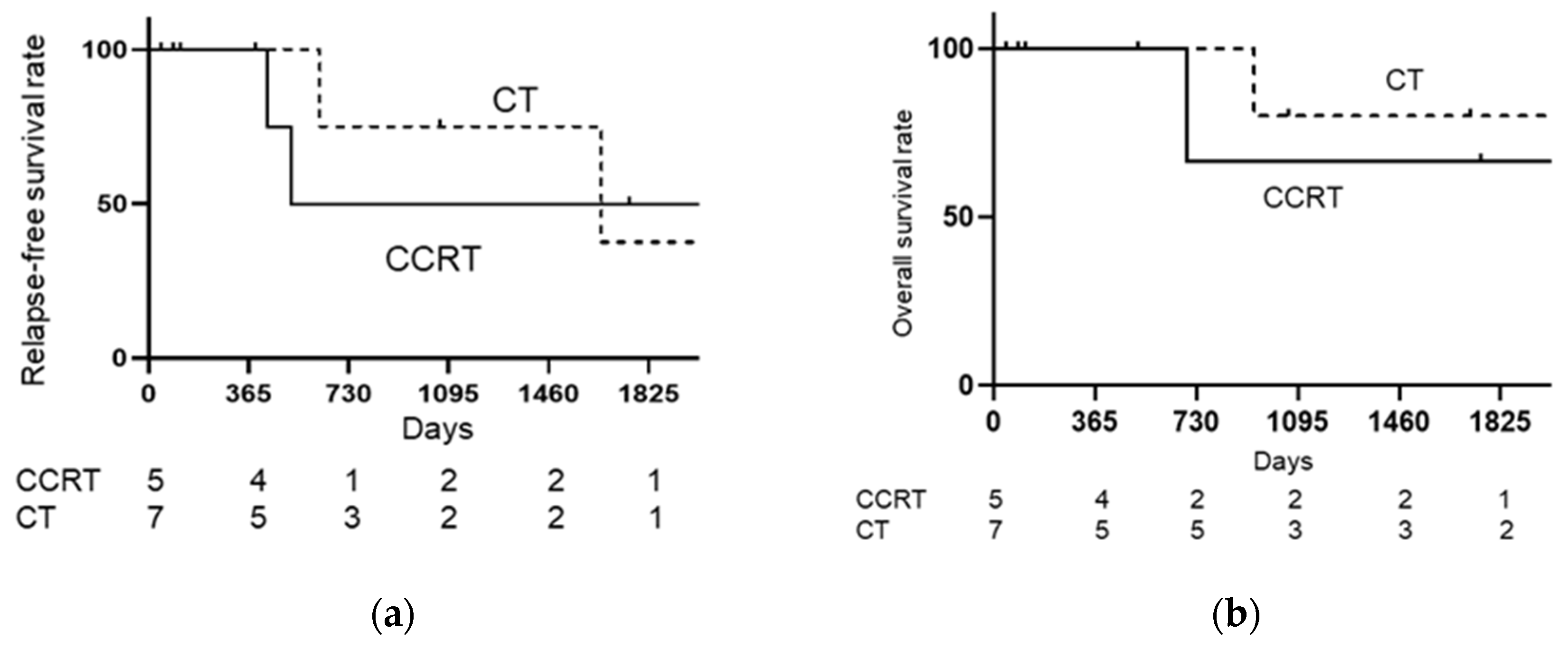
3.2. Treatment Outcomes
3.3. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer. IAfRo Cancer Fact Sheets: Cervical Cancer. Available online: http://gco.iarc.fr/today/data/pdf/fact-sheets/cancers/cancer-fact-sheets-16.pdf (accessed on 11 July 2019).
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri. Int. J. Gynecol. Obstet. 2018, 143, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Takekuma, M.; Kasamatsu, Y.; Kado, N.; Kuji, S.; Tanaka, A.; Takahashi, N.; Abe, M.; Hirashima, Y. The issues regarding postoperative adjuvant therapy and prognostic risk factors for patients with stage I-II cervical cancer: A review. J. Obstet. Gynaecol. Res. 2017, 43, 617–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takekuma, M.; Kasamatsu, Y.; Kado, N.; Kuji, S.; Tanaka, A.; Takahashi, N.; Abe, M.; Hirashima, Y. Reconsideration of postoperative concurrent chemoradiotherapy with fluorouracil and cisplatin for uterine cervical cancer. J. Obstet. Gynaecol. Res. 2015, 41, 1638–1643. [Google Scholar] [CrossRef] [PubMed]
- Matoda, M.; Takeshima, N.; Michimae, H.; Iwata, T.; Yokota, H.; Torii, Y.; Yamamoto, Y.; Takehara, K.; Nishio, S.; Takano, H.; et al. Postoperative chemotherapy for node-positive cervical cancer: Results of a multicenter phase II trial (JGOG1067). Gynecol. Oncol. 2018, 149, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Takekuma, M.; Shimokawa, M.; Nishio, S.; Omi, H.; Tabata, T.; Takei, Y.; Nasu, K.; Takahashi, Y.; Toyota, S.; Ichikawa, Y.; et al. Phase II study of adjuvant chemotherapy with paclitaxel and nedaplatin for uterine cervical cancer with lymph node metastasis. Cancer Sci. 2018, 109, 1602–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, W.A., 3rd; Liu, P.Y.; Barrett, R.J., 2nd; Stock, R.J.; Monk, B.J.; Berek, J.S.; Souhami, L.; Grigsby, P.; Gordon, W., Jr.; Alberts, D.S. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J. Clin. Oncol. 2000, 18, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Takei, Y.; Treilleux, I.; Devouassoux-Shisheboran, M.; Ledermann, J.; Viswanathan, A.N.; Mahner, S.; Provencher, D.M.; Mileshkin, L.; Åvall-Lundqvist, E.; et al. Gynecologic Cancer InterGroup (GCIG) Consensus Review for Small Cell Carcinoma of the Cervix. Int. J. Gynecol. Cancer 2014, 24, S102–S108. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.-M.; Zhang, X.; Ren, Y.-F.; Sun, X.-Y.; Di, N.; Zhou, N.; Pan, R.-K.; Ma, S.-H.; Zhou, L.-X. Chromogranin A (CgA) as Poor Prognostic Factor in Patients with Small Cell Carcinoma of the Cervix: Results of a Retrospective Study of 293 Patients. PLoS ONE 2012, 7, e33674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.-L.; Chang, T.-C.; Jung, S.-M.; Chen, C.-H.; Cheng, Y.-M.; Wu, H.-H.; Liou, W.-S.; Hsu, S.-T.; Ou, Y.-C.; Yeh, L.-S.; et al. Primary treatment and prognostic factors of small cell neuroendocrine carcinoma of the uterine cervix: A Taiwanese Gynecologic Oncology Group study. Eur. J. Cancer 2012, 48, 1484–1494. [Google Scholar] [CrossRef] [PubMed]
- Takekuma, M.; Kasamatsu, Y.; Kado, N.; Kuji, S.; Tanaka, A.; Takahashi, N.; Abe, M.; Hirashima, Y. Adjuvant chemotherapy versus concurrent chemoradiotherapy for high-risk cervical cancer after radical hysterectomy and systematic lymphadenectomy. Int. J. Clin. Oncol. 2016, 21, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Iwasaka, T.; Kamura, T.; Yokoyama, M.; Matsuo, N.; Nakano, H.; Sugimori, H. Adjuvant chemotherapy after radical hysterectomy for cervical carcinoma: A comparison with effects of adjuvant radiotherapy. Obstet Gynecol. 1998, 91, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, N.; Umayahara, K.; Fujiwara, K.; Hirai, Y.; Takizawa, K.; Hasumi, K. Treatment results of adjuvant chemotherapy after radical hysterectomy for intermediate- and high-risk stage IB–IIA cervical cancer. Gynecol. Oncol. 2006, 103, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, M.; Watari, H.; Kato, T.; Odagiri, T.; Konno, Y.; Endo, D.; Mitamura, T.; Kikawa, S.; Suzuki, Y.; Sakuragi, N. Clinical efficacy of paclitaxel/cisplatin as an adjuvant chemotherapy for patients with cervical cancer who underwent radical hysterectomy and systematic lymphadenectomy. J. Surg. Oncol. 2012, 105, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Shimada, M.; Aoki, Y.; Sakamoto, M.; Takeshima, N.; Fujiwara, H.; Matsumoto, T.; Mikami, M.; Sugiyama, T. Comparison of adjuvant therapy for node-positive clinical stage IB-IIB cervical cancer: Systemic chemotherapy versus pelvic irradiation. Int. J. Cancer 2017, 141, 1042–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Feng, Y.L.; Wan, T.; Zhang, Y.N.; Cao, X.P.; Huang, Y.W.; Xiong, Y.; Huang, X.; Zheng, M.; Li, Y.-F.; et al. Effectiveness of Sequential Chemoradiation vs Concurrent Chemoradiation or Radiation Alone in Adjuvant Treatment After Hysterectomy for Cervical Cancer: The STARS Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 361–369. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CCRT (n = 19) | CT (n = 21) | ||
|---|---|---|---|
| Age, years | |||
| Median (range) | 42 (28–67) | 44 (32–61) | |
| TNM stage | |||
| T1B | 11 | 14 | p = 0.04 |
| tumor size < 2 cm | 2 | 0 | |
| 2–3.9 cm | 5 | 6 | |
| >4 cm | 4 | 8 | |
| T2A | 3 | 0 | |
| T2B | 5 | 7 | |
| Histology | |||
| squamous cell carcinoma | 18 | 12 | |
| adenocarcinoma | 1 | 8 | p = 0.006 |
| small-cell carcinoma | 0 | 1 | |
| Number of metastatic lymph nodes | |||
| 1 | 11 | 10 | |
| 2 or more | 8 | 11 | |
| Regimen of CT | |||
| CPT11/NDP | 5 | ||
| CPT11/CDDP | 4 | ||
| PTX/NDP | 4 | ||
| DTX/CBDCA | 5 | ||
| PTX/CBDCA | 3 | ||
| Time to start adjuvant treatment | |||
| Median (range) | 50 (35–71) | 42 (25–87) | p = 0.4514 |
| CCRT | CT | |
|---|---|---|
| Locoregional | ||
| Intrapelvic lymph nodes | 1 | |
| Distant | ||
| Para-aortic lymph nodes | 3 | 3 |
| Lung | 1 | |
| Both | ||
| Vaginal, Para-aortic lymph nodes | 1 | |
| Intrapelvic and Para-aortic lymph nodes | 2 | |
| Lung, Intrapelvic lymph nodes | 1 |
| CCRT | CT | |
|---|---|---|
| Acute toxicities | ||
| Hematological toxicities | ||
| Neutropenia | 12 | |
| Anemia | 0 | |
| Thrombocytopenia | 0 | |
| Nonhematological toxicities | ||
| Nausea | 1 | |
| Vomiting | ||
| Diarrhea | 1 | |
| Late toxicities | ||
| Small intestinal obstruction | 1 | |
| Skin infection | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kagabu, M.; Nagasawa, T.; Tatsuki, S.; Fukagawa, Y.; Tomabechi, H.; Takatori, E.; Kaido, Y.; Shoji, T.; Baba, T. Comparison of Postoperative Adjuvant Chemotherapy and Concurrent Chemoradiotherapy for FIGO2018 Stage IIIC1 Cervical Cancer: A Retrospective Study. Medicina 2021, 57, 548. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060548
Kagabu M, Nagasawa T, Tatsuki S, Fukagawa Y, Tomabechi H, Takatori E, Kaido Y, Shoji T, Baba T. Comparison of Postoperative Adjuvant Chemotherapy and Concurrent Chemoradiotherapy for FIGO2018 Stage IIIC1 Cervical Cancer: A Retrospective Study. Medicina. 2021; 57(6):548. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060548
Chicago/Turabian StyleKagabu, Masahiro, Takayuki Nagasawa, Shunsuke Tatsuki, Yasuko Fukagawa, Hidetoshi Tomabechi, Eriko Takatori, Yoshitaka Kaido, Tadahiro Shoji, and Tsukasa Baba. 2021. "Comparison of Postoperative Adjuvant Chemotherapy and Concurrent Chemoradiotherapy for FIGO2018 Stage IIIC1 Cervical Cancer: A Retrospective Study" Medicina 57, no. 6: 548. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060548