
Diabetes Mellitus Promotes Smooth Muscle Cell Proliferation in Mouse Ureteral Tissue through the P-ERK/P-JNK/VEGF/PKC Signaling Pathway


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Study
2.2. Histopathological Examination
2.3. Western Blotting
2.4. Statistical Analyses
3. Results
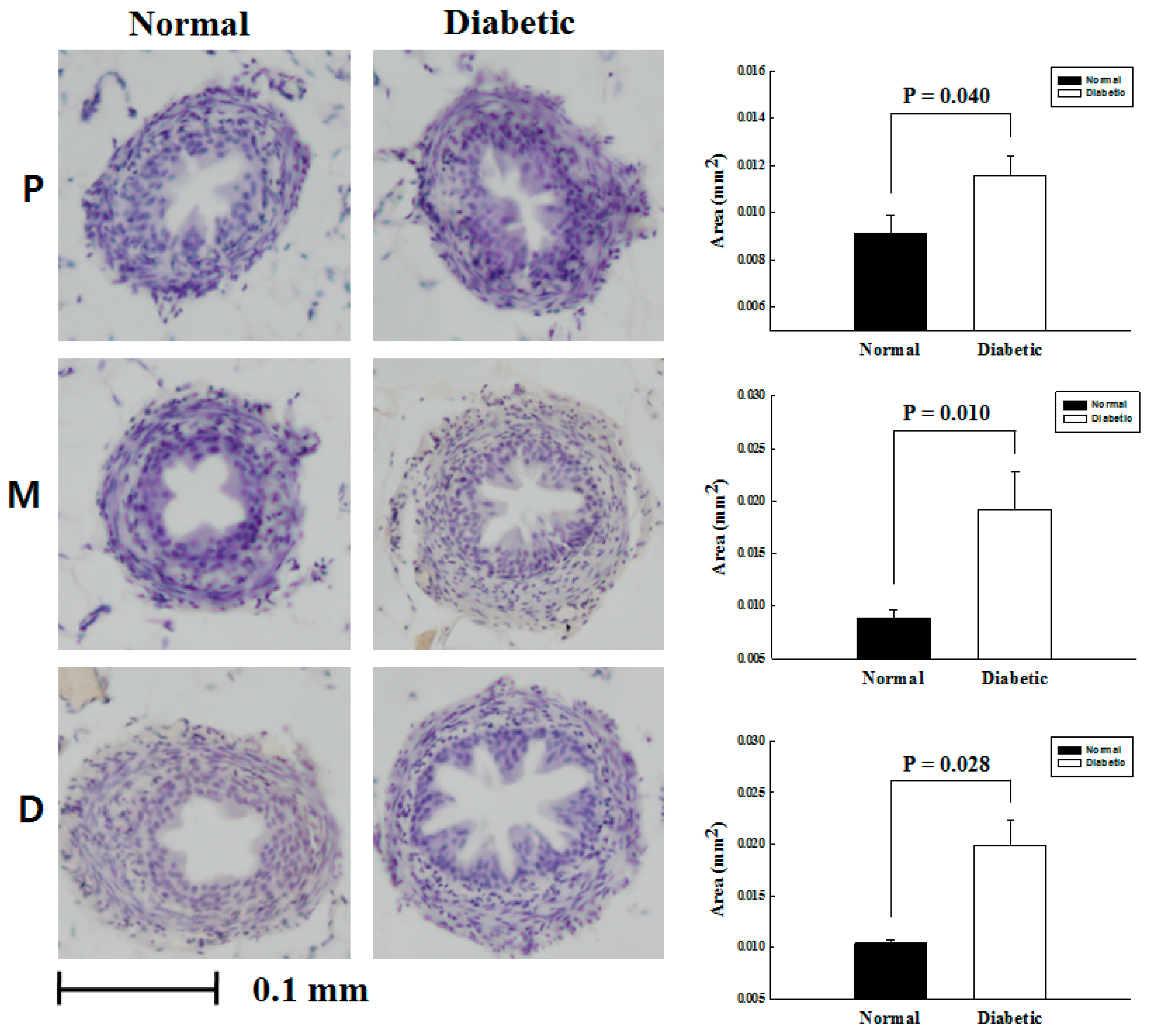
3.1. The Comparative Analysis on the Cross Sectional Area of Ureteral Smooth Muscle
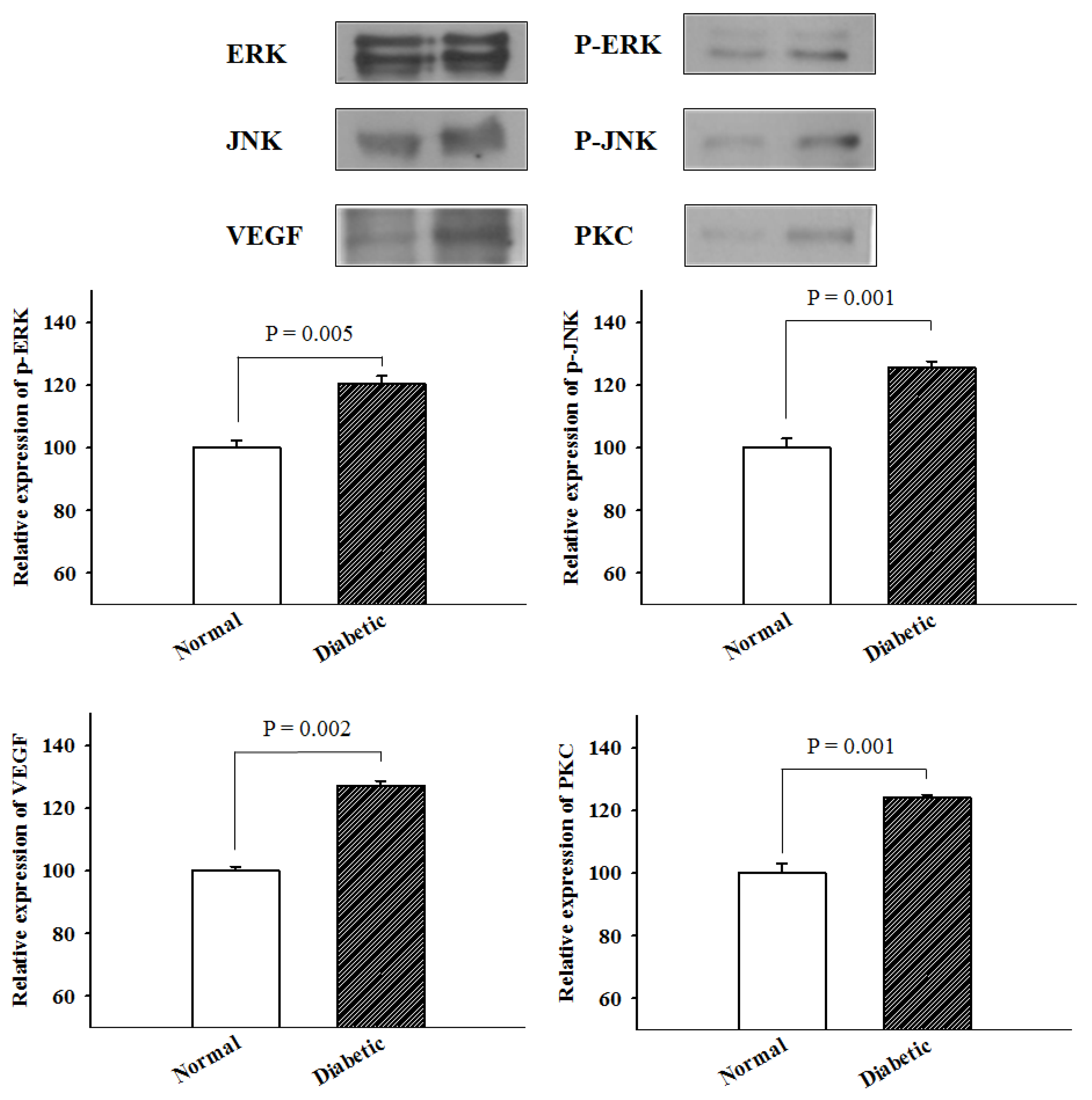
3.2. The Analysis of Protein Expression by Western Blotting
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sancak, E.B.; Resorlu, M.; Akbas, A.; Gulpinar, M.T.; Arslan, M.; Resorlu, B. Do Hypertension, diabetes mellitus and obesity increase the risk of severity of nephrolithiasis? Pak. J. Med. Sci. 2015, 31, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Thompson, C.S.; Calvert, R.C.; Mikhailidis, D.P.; Morgan, R.J. Decreased urinary bladder apoptosis in a rabbit model of diabetes mellitus. Urol. Res. 2002, 30, 79–83. [Google Scholar] [PubMed]
- Choi, T.; Yoo, K.H.; Choi, S.K.; Kim, D.S.; Lee, D.G.; Min, G.E.; Jeon, S.H.; Lee, H.L.; Jeong, I.K. Analysis of factors affecting spontaneous expulsion of ureteral stones that may predict unfavorable outcomes during watchful waiting periods: What is the influence of diabetes mellitus on the ureter? Korean J. Urol. 2015, 56, 455–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daneshgari, F.; Moore, C. Diabetic uropathy. Semin. Nephrol. 2006, 26, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Lieske, J.C.; de la Vega, L.S.; Gettman, M.T.; Slezak, J.M.; Bergstralh, E.J.; Melton, L.J., 3rd; Leibson, C.L. Diabetes mellitus and the risk of urinary tract stones: A population-based case-control study. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2006, 48, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Friedlander, J.I.; Moreira, D.M.; Elsamra, S.E.; Smith, A.D.; Okeke, Z. Differences in 24-h urine composition between nephrolithiasis patients with and without diabetes mellitus. BJU Int. 2015, 115, 619–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyarsky, S.; Labay, P.; Pfautz, C.J. The effect of nicotine upon ureteral peristalsis. South. Med. J. 1968, 61, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Davenport, K.; Timoney, A.G.; Keeley, F.X., Jr. Effect of smooth muscle relaxant drugs on proximal human ureteric activity in vivo: A pilot study. Urol. Res. 2007, 35, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Roshani, H.; Dabhoiwala, N.F.; Dijkhuis, T.; Pfaffendorf, M.; Boon, T.A.; Lamers, W.H. Pharmacological modulation of ureteral peristalsis in a chronically instrumented conscious pig model. I: Effect of cholinergic stimulation and inhibition. J. Urol. 2003, 170, 264–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulman, C.C.; Duarte-Escalante, O.; Boyarsky, S. The ureterovesical innervation. A new concept based on a histochemical study. Br. J. Urol. 1972, 44, 698–712. [Google Scholar] [CrossRef] [PubMed]
- Feliers, D.; Kasinath, B.S. Erk in kidney diseases. J. Signal Transduct. 2011, 2011, 768512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaede, P.; Lund-Andersen, H.; Parving, H.H.; Pedersen, O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N. Engl. J. Med. 2008, 358, 580–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, I.K.; Oh da, H.; Park, S.J.; Kang, J.H.; Kim, S.; Lee, M.S.; Kim, M.J.; Hwang, Y.C.; Ahn, K.J.; Chung, H.Y.; et al. Inhibition of NF-kappaB prevents high glucose-induced proliferation and plasminogen activator inhibitor-1 expression in vascular smooth muscle cells. Exp. Mol. Med. 2011, 43, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Chiong, M.; Morales, P.; Torres, G.; Gutierrez, T.; Garcia, L.; Ibacache, M.; Michea, L. Influence of glucose metabolism on vascular smooth muscle cell proliferation. VASA. Z. Gefasskrankh. 2013, 42, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Manna, P.R.; Stocco, D.M. The role of specific mitogen-activated protein kinase signaling cascades in the regulation of steroidogenesis. J. Signal Transduct. 2011, 2011, 821615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, Y.; Todokoro, K. Requirement of activation of JNK and p38 for environmental stress-induced erythroid differentiation and apoptosis and of inhibition of ERK for apoptosis. Blood 1999, 94, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Ardito, F.; Giuliani, M.; Perrone, D.; Troiano, G.; Lo Muzio, L. The crucial role of protein phosphorylation in cell signaling and its use as targeted therapy (Review). Int. J. Mol. Med. 2017, 40, 271–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebe-Suarez, S.; Zehnder-Fjallman, A.; Ballmer-Hofer, K. The role of VEGF receptors in angiogenesis; complex partnerships. Cell. Mol. Life Sci. CMLS 2006, 63, 601–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.; Zhang, H.; Liu, J.; Wang, G. Serum vascular endothelial growth factor level is elevated in patients with impaired glucose tolerance and type 2 diabetes mellitus. J. Int. Med. Res. 2019, 47, 5584–5592. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, M. Vascular Endothelial Growth Factor (VEGF) and Its Receptor (VEGFR) Signaling in Angiogenesis: A Crucial Target for Anti- and Pro-Angiogenic Therapies. Genes Cancer 2011, 2, 1097–1105. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Normal Mice | DM Mice | ||||
|---|---|---|---|---|---|
| Expression Level | Mean (±SD) | Expression Level | Mean (±SD) | ||
| P-ERK | Proximal | 104.54 | 100 ± 4.08 | 115.08 | 120.35 ± 4.56 |
| Middle | 98.83 | 122.99 | |||
| Distal | 96.63 | 122.99 | |||
| P-JNK | Proximal | 96.65 | 100 ± 5.23 | 126.56 | 125.67 ± 3.44 |
| Middle | 106.03 | 121.88 | |||
| Distal | 97.32 | 128.57 | |||
| VEGF | Proximal | 98.87 | 100 ± 2.35 | 126.35 | 127.25 ± 2.60 |
| Middle | 102.70 | 125.23 | |||
| Distal | 98.42 | 130.18 | |||
| PKC | Proximal | 94.93 | 100 ± 5.31 | 125.81 | 124.04 ± 1.73 |
| Middle | 105.53 | 123.96 | |||
| Distal | 99.54 | 122.35 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, T.; Lee, J.-W.; Kim, S.-K.; Yoo, K.-H. Diabetes Mellitus Promotes Smooth Muscle Cell Proliferation in Mouse Ureteral Tissue through the P-ERK/P-JNK/VEGF/PKC Signaling Pathway. Medicina 2021, 57, 560. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060560
Choi T, Lee J-W, Kim S-K, Yoo K-H. Diabetes Mellitus Promotes Smooth Muscle Cell Proliferation in Mouse Ureteral Tissue through the P-ERK/P-JNK/VEGF/PKC Signaling Pathway. Medicina. 2021; 57(6):560. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060560
Chicago/Turabian StyleChoi, Taesoo, Jeong-Woo Lee, Su-Kang Kim, and Koo-Han Yoo. 2021. "Diabetes Mellitus Promotes Smooth Muscle Cell Proliferation in Mouse Ureteral Tissue through the P-ERK/P-JNK/VEGF/PKC Signaling Pathway" Medicina 57, no. 6: 560. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060560