
Prognostic Value of Systemic Immune-Inflammation Index for Major Adverse Cardiac Events and Mortality in Severe Aortic Stenosis Patients after TAVI

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materıal and Methods
2.1. Study Population
2.2. SII
2.3. Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eveborn, G.W.; Schirmer, H.; Heggelund, G.; Lundet, P.; Ralsmussen, K. The evolving epidemiology of valvular aortic stenosis. the Tromsø study. Heart 2013, 99, 396–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galante, A.; Pietroiusti, A.; Vellini, M.; Piccolo, P.; Possati, G.; De Bonis, M.; Grillo, R.L.; Fontana, C.; Favalli, C. C-reactive protein is increased in patients with degenerative aortic valvular stenosis. J. Am. Coll. Cardiol. 2001, 38, 1078–1082. [Google Scholar] [CrossRef] [Green Version]
- Masson, J.B.; Kovac, J.; Schuler, G.; Ye, J.; Cheung, A.; Kapadia, S.; Tuzcu, M.E.; Kodali, S.; Leon, M.B.; Webb, J.G. Transcatheter aortic valve implantation: Review of the nature, management, and avoidance of procedural complications. JACC Cardiovasc. Interv. 2009, 2, 811–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toutouzas, K.; Stathogiannis, K.; Latsios, G.; Synetos, A.; Drakopoulou, M.; Penesopoulou, V.; Michelongona, A.; Tsiamis, E.; Tousoulis, D. Biomarkers in aortic valve stenosis and their clinical significance in transcatheter aortic valve implantation. Curr. Med. Chem. 2019, 26, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Kuno, T.; Hari, Y.; Nakashima, K.; Yokoyama, Y.; Ueyama, H.; Ando, T.; ALICE (All-Literature Investigation of Cardiovascular Evidence) Group. Prognostic impact of baseline C-reactive protein levels on mortality after transcatheter aortic valve implantation. J. Card. Surg. 2020, 35, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic value of systemic immune-inflammation index in cancer: A meta-analysis. J. Cancer 2018, 9, 3295–3302. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.H.; Huang, D.H.; Chen, Z.Y. Prognostic role of systemic immune-inflammation index in solid tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 75381–75388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Candemir, M.; Kiziltunç, E.; Nurkoç, S.; Şahinarslan, A. Relationship Between Systemic Immune-Inflammation Index (SII) and the Severity of Stable Coronary Artery Disease. Angiology 2021, 72, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zhang, Q.; Wang, R.; Ji, H.; Chen, Y.; Quan, X.-Q.; Zhang, C. Systemic Immune-Inflammatory Index Predicts Clinical Outcomes for Elderly Patients with Acute Myocardial Infarction Receiving Percutaneous Coronary Intervention. Med. Sci. Monit. 2019, 25, 9690–9701. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.M.; Aquilino, A.; Cortese, F.; Scicchitano, P.; Sassara, M.; Mola, E.; Rollo, R.; Caldarola, P.; Giorgino, F.; Pomo, V.; et al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc. Health Risk Manag. 2010, 6, 297–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; Van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document (VARC-2). Eur. J. Cardiothorac. Surg. 2012, 42, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Poggianti, E.; Venneri, L.; Chubuchny, V.; Jambrik, Z.; Baroncini, L.A.; Picano, E. Aortic valve sclerosis is associated with systemic endothelial dysfunction. J. Am. Coll. Cardiol. 2003, 41, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Mourino-Alvarez, L.; Baldan-Martin, M.; Gonzalez-Calero, L.; Martinez-Laborde, C.; Sastre-Oliva, T.; Moreno-Luna, R.; Lopez-Almodovar, L.F.; Sanchez, P.L.; Fernandez-Aviles, F.; Vivanco, F.; et al. Patients with calcific aortic stenosis exhibit systemic molecular evidence of ischemia, enhanced coagulation, oxidative stress and impaired cholesterol transport. Int. J. Cardiol. 2016, 225, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.; Roques, F.; Michel, P.; Gauducheau, E.; Lemeshow, S.; Salamon, R. European system for cardiac operative risk evaluation (EuroSCORE). Eur. J. Cardiothorac. Surg. 1999, 16, 9–13. [Google Scholar] [CrossRef]
- Wendt, D.; Osswald, B.R.; Kayser, K.; Thielmann, M.; Tossios, P.; Massoudy, P.; Kamler, M.; Jakob, H. Society of thoracic surgeons score is superior to the EuroSCORE determining mortality in high risk patients undergoing isolated aortic valve replacement. Ann. Thorac. Surg. 2009, 88, 468–474. [Google Scholar] [CrossRef]
- Condado, J.F.; Junpaparp, P.; Binongo, J.N.; Lasanajak, Y.; Witzke-Sanz, C.F.; Devireddy, C.; Leshnower, B.; Mavromatis, K.; Stewart, J.; Guyton, R.; et al. Neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) can risk stratify patients in transcatheter aortic-valve replacement (TAVR). Int. J. Cardiol. 2016, 223, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Álvarez, D.; López-Otero, D.; González-Ferreiro, R.; Sanmartín-Pena, X.; Cid-Álvarez, B.; Trillo, R.; Jualnatey, J.R.G. Prognostic Value of hs-CRP after Transcatheter Aortic Valve Implantation. Circ. Cardiovasc. Interv. 2018, 11, e007213. [Google Scholar] [CrossRef] [PubMed]
- Okuno, T.; Koseki, K.; Nakanishi, T.; Sato, K.; Ninomiya, K.; Tomii, D.; Tanaka, T.; Sato, Y.; Horiuchi, Y.; Koike, H.; et al. Evaluation of objective nutritional indexes predictors of one-year outcomes after transcatheter aortic valve implantation. J. Cardiol. 2019, 74, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, M.; Yamada, T.; Morita, T.; Furukawa, Y.; Tamaki, S.; Iwasaki, Y.; Kawasaki, M.; Kikuchi, A.; Kawai, T.; Ikeda, I.; et al. P589Prognostic value of systemic immune-inflammation index in patients with chronic heart failure. Eur. Heart J. 2018, 39. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Population (n = 120) | MACEs (−) (n = 86) | MACEs (+) (n = 34) | p Value | |
|---|---|---|---|---|
| Male gender, n (%) | 68 (56.7) | 47 (54.7) | 21 (61.8) | 0.48 |
| Age, years | 77.5 ± 4.6 | 77.6 ± 4.9 | 77.2 ± 3.7 | 0.70 |
| BMI, kg/m2 | 23.1 ± 2.0 | 23.0 ± 2.0 | 23.2 ± 2.1 | 0.63 |
| Risk factors | ||||
| Hypertension, n (%) | 68 (56.7) | 53 (61.6) | 15 (44.1) | 0.08 |
| Diabetes, n (%) | 72 (60) | 50 (58.1) | 22 (64.7) | 0.51 |
| Smoking, n (%) | 16 (13.3) | 12 (14.0) | 4 (11.8) | 0.75 |
| Hyperlipidemia, n (%) | 53 (44.2) | 39 (45.3) | 14 (41.2) | 0.68 |
| CAD history, n (%) | 47 (39.2) | 35 (40.7) | 12 (35.3) | 0.59 |
| PAD, n (%) | 28 (23.3) | 22 (25.6) | 6 (17.6) | 0.35 |
| CRF history, n (%) | 23 (19.2) | 16 (18.6) | 7 (20.6) | 0.80 |
| COPD, n (%) | 53 (44.2) | 38 (44.2) | 15 (44.1) | 0.99 |
| CVA history, n (%) | 6 (5) | 3 (3.5) | 3 (8.8) | 0.23 |
| NYHA Class III-IV, n (%) | 43 (35.8) | 28 (32.6) | 15 (44.1) | 0.23 |
| Atrial fibrillation, n (%) | 20 (16.7) | 12 (14) | 8 (23.5) | 0.20 |
| Presence of BBB, n (%) | 19 (15.8) | 11 (12.8) | 8 (23.5) | 0.15 |
| Medications | ||||
| Acetylsalicylic acid, n (%) | 33 (27.5) | 26 (30.2) | 7 (20.6) | 0.29 |
| OAC, n (%) | 16 (13.3) | 10 (11.6) | 6 (17.6) | 0.38 |
| Beta-blockers, n (%) | 44 (36.7) | 34 (39.5) | 10 (29.4) | 0.30 |
| RAS blockers, n (%) | 39 (32.5) | 30 (34.9) | 9 (26.5) | 0.38 |
| Statin, n (%) | 18 (15) | 12 (14) | 6 (17.6) | 0.61 |
| Diuretic, n (%) | 34 (28.5) | 25 (29.1) | 9 (26.5) | 0.78 |
| All Population (n = 120) | MACEs (−) (n = 86) | MACEs (+) (n = 34) | p Value | |
|---|---|---|---|---|
| FBG, mg/dL | 125.8 ± 39.8 | 125.7 ± 40.5 | 126 ± 38.7 | 0.98 |
| Creatinine, mg/dL | 1.1 (0.8–1.58) | 1.0 (0.78–1.53) | 1.1 (0.8–1.83) | 0.47 |
| TC, mg/dL | 206.5 ± 39.9 | 207.7 ± 41.9 | 203.4 ± 34.6 | 0.60 |
| LDL-C, mg/dL | 138.9 ± 39.1 | 139.2 ± 41.0 | 138.1 ± 33.6 | 0.89 |
| HDL-C, mg/dL | 41.2 ± 4.0 | 41.4 ± 6.9 | 40.6 ± 6.4 | 0.52 |
| Triglyceride, mg/dL | 175 (146.3–195) | 175 (148.8–195.3) | 174.5 (143–195) | 0.35 |
| CRP, mg/dL | 2.5 (0.9–4.9) | 1.8 (0.8–4.5) | 4.9 (2.3–7.2) | <0.01 |
| Hemoglobin, mg/dL | 15.1 ± 3.5 | 14.9 ± 1.1 | 15.0 ± 3.0 | 0.86 |
| Platelet, µ × 103/µL | 263.7 ± 73.2 | 260.4 ± 70 | 271.9 ± 81.4 | 0.44 |
| WBC, µ × 103/µL | 7.0 (5.5–8.2) | 6.2 (5.2–7.4) | 8.3 (7.5–9.1) | <0.01 |
| SII, 103/µL | 737 (407–1145) | 522 (344–845) | 1283 (1153–1399) | <0.01 |
| All Population (n = 120) | Low SII (n = 82) | High SII (n = 38) | p Value | |
|---|---|---|---|---|
| Aortic valve area, cm2 | 0.81 ± 0.1 | 0.83 ± 0.09 | 0.78 ± 0.1 | 0.01 |
| Mean AVG, mmHg | 47.8 ± 4.1 | 46.9 ± 3.3 | 50.0 ± 5.2 | <0.01 |
| LV ejection fraction, % | 55.5 ± 7.9 | 55.4 ± 7.9 | 55.9 ± 8.2 | 0.77 |
| STS score, median | 9.6 (8.1–11.5) | 10.3 (8.1–11.5) | 9.2 (8.1–12.3) | 0.96 |
| Predilation, n (%) | 19 (15.8) | 15 (18.3) | 4 (10.5) | 0.28 |
| Postdilatation, n (%) | 16 (13.3) | 9 (11) | 7 (18.4) | 0.26 |
| Implantation depth, mm | 5.2 ± 0.8 | 5.3 ± 0.7 | 5.1 ± 0.8 | 0.35 |
| Type of valve, n (%) | ||||
| Balloon-expandable | 37 (30.8) | 28 (34.1) | 9 (23.7) | 0.25 |
| Self-expandable | 83 (69.2) | 54 (65.9) | 29 (76.3) | 0.25 |
| All Population (n = 120) | Low SII (n = 82) | High SII (n = 38) | p Value | |
|---|---|---|---|---|
| Major vascular complications, n (%) | 18 (15) | 1 (1.2) | 17 (44.7) | <0.01 |
| Major bleeding, n (%) | 9 (7.5) | 1 (1.2) | 8 (21.1) | <0.01 |
| Permanent pacemaker, n (%) | 7 (5.8) | 1 (1.2) | 6 (15.8) | <0.01 |
| Re-hospitalization, n (%) | 9 (7.5) | 0 (0) | 9 (23.7) | <0.01 |
| Postprocedural IS or TIA, n (%) | 8 (6.7) | 1 (1.2) | 7 (18.4) | <0.01 |
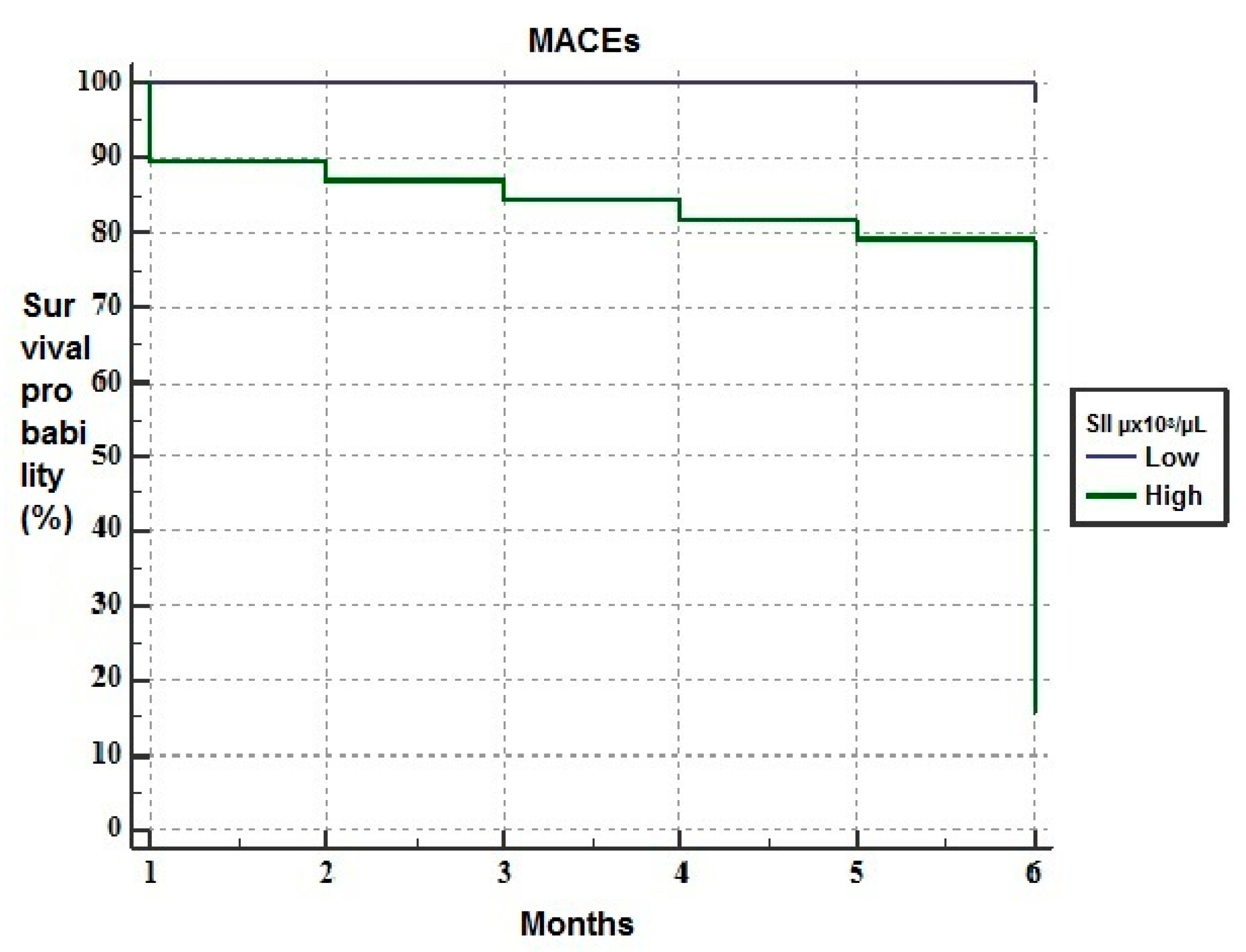
| 6-month mortality, n (%) | 8 (6.7) | 0 (0) | 8 (23.5) | <0.01 |
| MACEs, n (%) | 34 (28.3) | 2 (2.4) | 32 (84.2) | <0.01 |
| Univariable | Multivariable Model-1 | Multivariable Model-2 | ||||
|---|---|---|---|---|---|---|
| HR (95%CI) | p Value | HR (95%CI) | p Value | HR (95%CI) | p Value | |
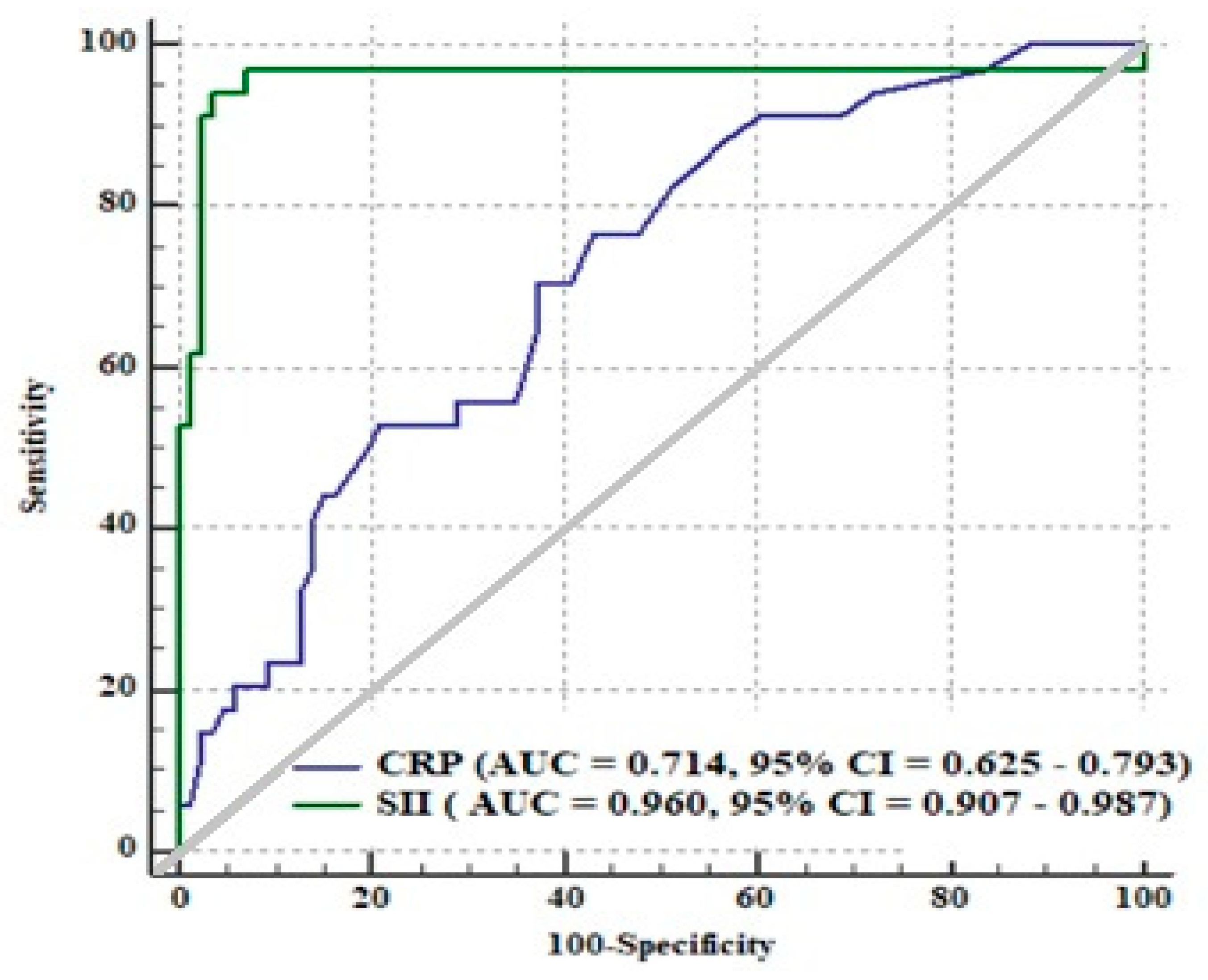
| CRP | 1.107 (1.033–1.186) | <0.01 | 1.050 (0.974–1.132) | 0.20 | − | − |
| AVG | 1.143 (1.056–1.236) | <0.01 | 1.139 (1.052–1.233) | <0.01 | 1.050 (0.964–1.144) | 0.260 |
| STS | 1.158 (1.046–1.281) | <0.01 | 1.178 (1.056–1.313) | <0.01 | 1.127 (1.011–1.256) | 0.03 |
| SII | 1.002 (1.002–1.003) | <0.01 | − | − | 1.002 (1.001–1.003) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tosu, A.R.; Kalyoncuoglu, M.; Biter, H.İ.; Cakal, S.; Selcuk, M.; Çinar, T.; Belen, E.; Can, M.M. Prognostic Value of Systemic Immune-Inflammation Index for Major Adverse Cardiac Events and Mortality in Severe Aortic Stenosis Patients after TAVI. Medicina 2021, 57, 588. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060588
Tosu AR, Kalyoncuoglu M, Biter Hİ, Cakal S, Selcuk M, Çinar T, Belen E, Can MM. Prognostic Value of Systemic Immune-Inflammation Index for Major Adverse Cardiac Events and Mortality in Severe Aortic Stenosis Patients after TAVI. Medicina. 2021; 57(6):588. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060588
Chicago/Turabian StyleTosu, Aydin Rodi, Muhsin Kalyoncuoglu, Halil İbrahim Biter, Sinem Cakal, Murat Selcuk, Tufan Çinar, Erdal Belen, and Mehmet Mustafa Can. 2021. "Prognostic Value of Systemic Immune-Inflammation Index for Major Adverse Cardiac Events and Mortality in Severe Aortic Stenosis Patients after TAVI" Medicina 57, no. 6: 588. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060588