
Evaluation of Patients with Syncope in the Emergency Department: How to Adjust Pharmacological Therapy


Syncope Unit, Geriatric and Intensive Care Unit, University of Florence and Azienda Ospedaliero-Universitaria Careggi, Largo Brambilla 3, 50134 Florence, Italy
*
Author to whom correspondence should be addressed.
†
Contributed equally to the paper.
Medicina 2021, 57(6), 603; https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060603
Submission received: 3 May 2021
/
Revised: 5 June 2021
/
Accepted: 8 June 2021
/
Published: 11 June 2021
(This article belongs to the Special Issue Syncope in the Emergency Department)
Abstract
:The rate of syncope in the Emergency Department ranges between 0.9 and 1.7%. Syncope is mostly related to a underlying reflex or orthostatic mechanism. A bradycardic or a hypotensive phenotype, may be identified. The latter is the most common and could be constitutional or drug induced. Consequently, obtaining an accurate drug history is an important step of the initial assessment of syncope. As anti-hypertensive medication might be responsible for orthostatic hypotension, managing hypertension in patients with syncope requires finding an ideal balance between hypotensive and cardiovascular risks. The choice of anti-hypertensive molecule as well as the therapeutic regimen and dosage, influences the risk of syncope. Not only could anti-hypertensive drugs have a hypotensive effect but opioids and psychoactive medications may also be involved in the mechanism of syncope. Proper drug management could reduce syncope recurrences and their consequences.
1. Introduction
Syncope is defined as a “transient loss of consciousness (TLoC) due to cerebral hypoperfusion, characterized by rapid onset, short duration, and spontaneous complete recovery” [1]. Syncope is usually classified as reflex, orthostatic or cardiac. The principal causes of syncope, which need to be addressed in the differential diagnostic process, are listed in Table 1. The prognosis varies with the type of syncope, with cardiac syncope being the most likely to lead to an increased risk of negative events [2]. Although the prognosis largely depends on the underlying cause of syncope, a syncope-related fall could be a relevant prognostic factor in all types of syncope [3,4,5,6].
Despite its frequency in the general population [2], the accurate estimation of the incidence of syncope is challenging due to the fact that different definitions have been used and because most of the patients with syncopal episodes do not seek medical assistance. However, studies conducted up to now report a frequency of syncope in Emergency Departments (ED) between 0.9 and 1.7% [7,8,9] with a hospital admission rate of up to 38% in some countries resulting in remarkable healthcare costs [10,11,12]. In addition, considering the economic burden of syncope, the readmission rate must also be taken into consideration. In one study, syncope was the most common cause of readmission, with a median cost of all-cause 30-day readmission of $26,127 [13].
In view of the above, the first medical contact, for instance in an ED, must be placed at the centre of all the strategies in order to minimize negative outcomes and to provide substantial cost savings. This proves to be particularly important when considering that the only initial evaluation may guide the diagnosis in up to 50% of the cases [14]. Indeed, the current European Society of Cardiology (ESC) guidelines on syncope [1] recommend a careful and standardized approach, which is easy to use at any age and in any clinical situation. Even if there is no independent reference standard for diagnosing, there is widespread agreement that the initial evaluation may help in distinguishing between high and low risk syncope.
Careful therapeutic recognition is the key to the initial evaluation of syncope, and should address classes of drugs, duration of treatment, relationship between drug consumption and induction of possible adverse effects. Antihypertensive drugs, diuretics, vasodilators, or pro-arrhythmic drugs can be involved in the pathophysiology of syncope [15]. This is mostly true in older adults who are usually on multiple medications.
2. When Should the Pharmacological Therapy Be Adjusted?
A proper risk stratification of syncope in the ED enables discrimination between discharge and admission for urgent investigation. Careful history taking, physical examination, including supine and standing blood pressure (BP) measurements, and electrocardiograms (ECG) represent the core assessment [1].
Forty to forty-five percent of non-cardiovascular and some cardiovascular life-threatening underlying conditions can be detected during ED evaluation [16]. In fact, about half of the cases of cardiac syncope are diagnosed in ED. In the other cases, a cardiac diagnosis may first be suspected and then confirmed by prolonged ECG monitoring or, less frequently, by electrophysiological study or stress test. Patients with low-risk features do not need further diagnostic tests in the ED, as they are likely to have reflex or orthostatic syncope.
Reflex/vasovagal syncope and orthostatic hypotension (OH) are the most frequent causes of transient loss of consciousness and are considered as the cardiovascular cause of orthostatic intolerance [17]. OH is defined as a fall in systolic blood pressure from a baseline value ≥20 mmHg or diastolic blood pressure ≥10 mmHg or a sustained decrease in Systolic Blood Pressure (SBP) to an absolute value <90 mmHg within 3 min of orthostatic position. When the loss of consciousness occurs on assuming the standing position, and there is concomitant significant orthostatic hypotension, orthostatic syncope is confirmed [1].
A bradycardic and a hypotensive phenotype of syncope may also be identified [18].
A “low blood pressure phenotype” identifies patients in whom a chronic low BP plays a role in causing orthostatic reflex syncope and orthostatic intolerance [1]. The hypotensive phenotype is the most common mechanism of syncope and could be constitutional [19,20] or drug-related, when BP is constantly below the target range in patients on antihypertensive treatment.
Hypotensive drugs may exacerbate hypotensive susceptibility, especially as vulnerability to vertical posture stress [21]. In addition, orthostatic vasovagal syncope, situational reflex syncope, vaso-depressive and mixed carotid sinus syndrome, OH-related syncope, postprandial hypotension, reflex syncope triggered by tachyarrhythmia and recurrent severe hypotensive episodes during ambulatory BP monitoring (daytime SBP <90 mmHg), may all be related to hypotensive susceptibility [1].
Patients prone to reflex syncope may thus be more sensitive to antihypertensive medication, resulting in a greater BP drop. Moreover, orthostatic hypotension is most commonly drug-related, particularly in older hypertensive patients on three or more hypotensive medications [22,23,24], in whom a systolic BP <100 mm Hg is considered inappropriately low [25,26].
The bradycardic phenotype is likely when syncope occurs during a spontaneous or induced asystole lasting more than 3 s [27]. However, syncope due to cardiac arrhythmias or to structural heart disease, syncope occurring in the supine position, vasovagal syncope triggered by emotional distress (blood phobia, instrumentation, visceral or somatic pain), or cardio-inhibitory reflex syncope are less likely to be related to hypotensive medications.
In view of the above, drug adjustment is a crucial step in the evaluation of patients with hypotensive syncope.
3. How to Adjust Medication?
Vaso-active and cardio-active drugs may hinder the compensatory reflex responses to standing (e.g., sympathetic-mediated vasoconstriction and increased heart rate response), increase venous pooling (e.g., vasodilators) and/or induce volume depletion (e.g., diuretics), thus favouring OH, which can trigger a reflex bradycardia, when delayed.
In hypertensive patients with drug-related hypotension, the physician should tailor the pharmacological therapy so as to balance between the risk of cardiovascular events and the risk of syncope recurrence.
In patients with recurrent and severe episodes of syncope, especially when older and frail, blood pressure lowering medication should be prescribed with caution. Previous studies have demonstrated a decrease in syncopal recurrences after the reduction or discontinuation of anti-hypertensive medications in adults and older patients, with no safety concerns [28,29,30,31]. Thus, tailoring prescriptions of blood pressure drugs to age, frailty, disability, risk of cardiovascular events and syncope relapses has been proposed (Table 2).
Not only could anti-hypertensive drugs have a hypotensive effect, but also drugs that might increase hypotensive susceptibility, as listed in Table 3.
4. Vaso-Active and Cardio-Active Drugs
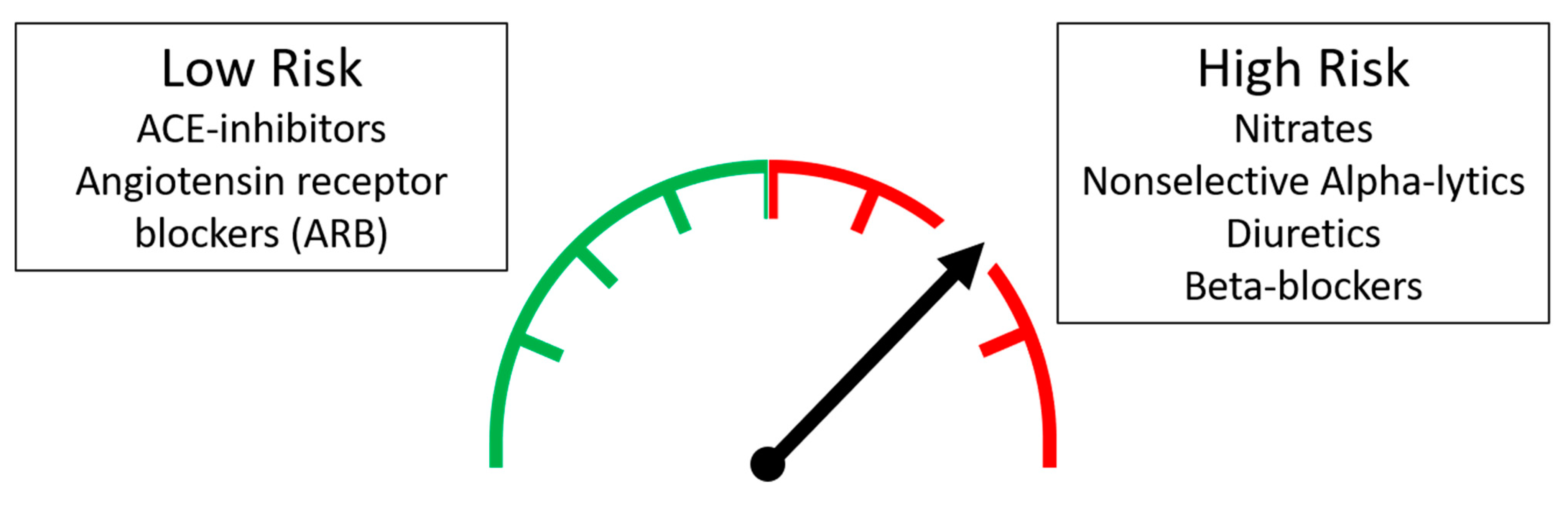
Anti-hypertensive medications are known predisposing factors for OH, through the above-mentioned mechanisms. However, in the light of the available scientific evidence, some “higher risk” classes of drugs have been identified (Figure 1):
Nitrates. Nitrates stimulate nitric oxide release, inducing smooth muscle vascular wall relaxation, venous vasodilation, and therefore reduction in preload. Nitrates significantly increase the risk of orthostatic syncope, regardless of dosage and comorbidities [33,34,35,36].
Nonselective alpha-receptor adrenergic antagonists (or alpha-lytic). Alpha-receptor adrenergic antagonists inhibit the vasoconstrictor effect mediated by catecholamines through the selective blockade of α1-adrenergic receptors and thus induce arterial and venous vasodilation, with the consequent reduction of peripheral resistance and increased venous capacitance (mediated by binding to 1B receptors).
Alpha-lytics facilitate bladder emptying by binding 1A receptors in the prostate and bladder, and thus are widely used in the treatment of urinary tract obstruction. Numerous studies conducted in different clinical settings have demonstrated the role of alpha-lytics as determinants of OH in the elderly [37,38,39]. Alpha1-receptor blockage counteracts the vasoconstriction that occurs upon standing [40]. Highly selective molecules such as silodosine and tamsulosine reduce the risk of hypotension, which is greater for less selective molecules such as alfuzosin, terazosin and doxazosin [41].
Diuretics. Diuretic therapy can increase the risk of orthostatic hypotension by inducing volume depletion, which may be sufficient to alter the BP response to standing, especially in the elderly [35]. In addition, loop diuretics have been significantly associated with orthostatic hypotension in patients with syncope [42].
Beta-blockers. Beta-blockers interfere with BP response when standing, counteracting heart rate, cardiac output increase, and sympatho-mediated vasoconstriction upon standing. Therapy with beta-blockers was associated with an increased risk of initial orthostatic hypotension [43].
“Low risk” classes of drugs can be identified as the following:
ACE-inhibitors and angiotensin II receptor blockers (ARB). ACE-inhibitors reduce angiotensin II and increase kinin levels, both inducing vasodilation.
ARBs are competitive antagonists of angiotensin II, type 1 receptors. Studies that investigated the effect of these two classes of drugs on BP pressure response upon standing have not identified a close association with orthostatic hypotension [43,44,45]. On the contrary, some data seem to suggest a protective effect of both ACE-inhibitors [44,46] and ARBs [47].
Areas of Uncertainty:
Calcium channel blockers. Data are conflicting. A protective effect of dihydropyridine calcium channel blockers on OH has been reported [48], while other studies suggest increased risk factors [47,49]. Non-dihydropyridine calcium channel blockers have negative chronotropic and inotropic effects, which may impede heart rate compensatory responses to standing [23].
Clonidine. Little is known about the impact of clonidine on BP response upon standing. It is not clear whether clonidine is a protective or a risk element for OH [50].
Other Medications
In addition to cardiovascular medications, other drugs may have a hypotensive effect and may interfere with reflex responses to standing.
Orthostatic hypotension is a potential side effect of tricyclic antidepressants, trazodone and antipsychotics due to alpha-adrenergic receptor blockade [47,49,51].
Selective serotonin reuptake inhibitors and benzodiazepines have been associated with abnormal upright BP responses [52,53].
5. Specifically, What Procedures Should Be Carried Out in the ED?
According to ESC guidelines of syncope [1], the ED physician must first rule out arrhythmic or structural cardiac causes of syncope.
After having excluded cardiac syncope, the physician should define whether the syncope is likely OH-related or neurally-mediated. In both cases, patients need to be instructed on appropriate hydration, physical countermeasures, physical conditioning and the use of compressive stockings in OH. This is the core management.
In the case of drug-related hypotension and/or orthostatic hypotension, it is reasonable to consider the withdrawal or reduction of hypotensive medications after evaluating cardiovascular risks. Considering changing molecules or therapy regimen should be an alternative when it is not possible to withdraw a medication.
Practical details are shown in Table 4
6. Conclusions
Reflex syncope and orthostatic hypotension are the most frequent causes of transient loss of consciousness, considered as a cardiovascular cause of orthostatic intolerance.
Anti-hypertensive, psychoactive medications, opioids and other classes of drugs have vaso-active effects and might predispose a patient to orthostatic hypotension and syncope.
Accurate therapeutic recognition is an important step in the assessment of syncope. Proper management of the pharmacological therapy could reduce syncope recurrences and their consequences.
Author Contributions
Each author has contributed to the draft and revision of the manuscript. Each author has approved the submitted version and version substantially edited by journal staff that involves the author’s contribution to the study. Each author agrees to be personally accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Soteriades, E.S.; Evans, J.C.; Larson, M.G.; Chen, M.H.; Chen, L.; Benjamin, E.J.; Levy, D. Incidence and prognosis of syncope. N. Engl. J. Med. 2002, 347, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Costantino, G.; Perego, F.; Dipaola, F.; Borella, M.; Galli, A.; Cantoni, G.; Dell’Orto, S.; Dessi, S.; Filardo, N.; Duca, P.G.; et al. Short- and long-term prognosis of syncope; risk factors; and role of hospital admission: Results from the STePS (Short-Term Prognosis of Syncope) study. J. Am. Coll. Cardiol. 2008, 51, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Ungar, A.; Del Rosso, A.; Giada, F.; Bartoletti, A.; Furlan, R.; Quartieri, F.; Lagi, A.; Morrione, A.; Mussi, C.; Lunati, M.; et al. Early and late outcome of treated patients referred for syncope to emergency department: The EGSYS 2 follow-up study. Eur. Heart J. 2010, 31, 2021–2026. [Google Scholar] [CrossRef] [Green Version]
- Nume’, A.K.; Carlson, N.; Gerds, T.A.; Holm, E.; Pallisgaard, J.; Søndergaard, K.B.; Hansen, M.L.; Vinther, M.; Hansen, J.; Gislason, G.; et al. Risk of postdischarge fall-related injuries among adult patients with syncope: A nationwide cohort study. PLoS ONE 2018, 13, e0206936. [Google Scholar] [CrossRef]
- Furtan, S.; Pochciał, P.; Timler, D.; Ricci, F.; Sutton, R.; Fedorowski, A.; Zyśko, D. Prognosis of Syncope With Head Injury: A Tertiary Center Perspective. Front. Cardiovasc. Med. 2020, 7, 125. [Google Scholar] [CrossRef]
- Thiruganasambandamoorthy, V.; Stiell, I.; Wells, G. Frequency and outcomes of syncope in the emergency department. Can. J. Emerg. Med. Care 2008, 10, 255–295. [Google Scholar]
- Task Force for the Diagnosis and Management of Syncope; European Society of Cardiology (ESC); European Heart Rhythm Association (EHRA); Heart Failure Association (HFA); Heart Rhythm Society (HRS); Moya, A.; Sutton, R.; Ammirati, F.; Blanc, J.J.; Brignole, M.; et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur. Heart J. 2009, 30, 2631–2671. [Google Scholar] [CrossRef] [Green Version]
- Probst, M.A.; Kanzaria, H.K.; Gbedemah, M.; Richardson, L.D.; Sun, B.C. National trends in resource utilization associated with ED visits for syncope. Am. J. Emerg. Med. 2015, 33, 998–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brignole, M.; Menozzi, C.; Bartoletti, A.; Giada, F.; Lagi, A.; Ungar, A.; Ponassi, I.; Mussi, C.; Maggi, R.; Re, G.; et al. A new management of syncope: Prospective systematic guideline-based evaluation of patients referred urgently to general hospitals. Eur. Heart J. 2006, 27, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.C.; Emond, J.A.; Camargo, C.A., Jr. Direct medical costs of syncope-related hospitalizations in the United States. Am. J. Cardiol. 2005, 95, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Ungar, A.; Tesi, F.; Chisciotti, V.M.; Pepe, G.; Vanni, S.; Grifoni, S.; Balzi, D.; Rafanelli, M.; Marchionni, N.; Brignole, M. Assessment of a structured management pathway for patients referred to the Emergency Department for syncope: Results in a tertiary hospital. Europace 2016, 18, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Kadri, A.N.; Abuamsha, H.; Nusairat, L.; Kadri, N.; Abuissa, H.; Masri, A.; Hernandez, A.V. Causes and Predictors of 30-Day Readmission in Patients With Syncope/Collapse: A Nationwide Cohort Study. J. Am. Heart Assoc. 2018, 7, e009746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brignole, M.; Ungar, A.; Bartoletti, A.; Ponassi, I.; Lagi, A.; Mussi, C.; Ribani, M.A.; Tava, G.; Disertori, M.; Quartieri, F.; et al. Standardized-care pathway vs. usual management of syncope patients presenting as emergencies at general hospitals. Evaluation of Guidelines in Syncope Study 2 (EGSYS-2) GROUP. Europace 2006, 8, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Davidson, E.; Fuchs, J.; Rotenberg, Z.; Weinberger, I.; Agmon, J. Drug-related syncope. Clin. Cardiol. 1989, 12, 577–580. [Google Scholar] [CrossRef]
- Reed, M.J.; Newby, D.E.; Coull, A.J.; Prescott, R.J.; Jacques, K.G.; Gray, A.J. The ROSE (Risk Stratification of Syncope in the Emergency department) study. J. Am. Coll. Cardiol. 2010, 55, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, D. The epidemic of orthostatic tachycardia and orthostatic intolerance. Am. J. Med. Sci. 1999, 317, 75–77. [Google Scholar] [CrossRef]
- Brignole, M.; Rivasi, G. New insights in diagnostics and therapies in syncope: A novel approach to non-cardiac syncope. Heart 2021. [Google Scholar] [CrossRef]
- Duschek, S.; Schandry, R. Reduced brain perfusion and cognitive performance due to constitutional hypotension. Clin. Auton. Res. 2007, 17, 69–76. [Google Scholar] [CrossRef] [Green Version]
- WHO Expert Committee. Arterial Hypertension: Report of a WHO Expert Committee; World Health Organization technical report series; WHO: Geneva, Switzerland, 1978; pp. 7–56. [Google Scholar]
- Sutton, R.; Brignole, M. Twenty-eight years of research permit reinterpretation of tilt-testing: Hypotensive susceptibility rather than diagnosis. Eur. Heart J. 2014, 35, 2211–2212. [Google Scholar] [CrossRef] [Green Version]
- Kamaruzzaman, S.; Watt, H.; Carson, C.; Ebrahim, S. The association between orthostatic hypotension and medication use in the British Women’s Heart and Health Study. Age Ageing 2010, 39, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Stefano, C.; Milazzo, V.; Totaro, S.; Sobrero, G.; Ravera, A.; Milan, A.; Maule, S.; Veglio, F. Orthostatic hypotension in a cohort of hypertensive patients referring to a hypertension clinic. J. Hum. Hypertens. 2015, 29, 599–603. [Google Scholar] [CrossRef]
- Ceccofiglio, A.; Mussi, C.; Rafanelli, M.; Rivasi, G.; Bo, M.; Mossello, E.; Martone, A.M.; Abete, P.; Ungar, A. Increasing Prevalence of Orthostatic Hypotension as a Cause of Syncope With Advancing Age and Multimorbidity. J. Am. Med. Dir. Assoc. 2019, 20, 586–588. [Google Scholar] [CrossRef]
- Scuteri, A.; Modestino, A.; Frattari, A.; Di Daniele, N.; Tesauro, M. Occurrence of hypotension in older participants. Which 24-hour ABPM parameter better correlate with? J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 804–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrissey, Y.; Bedford, M.; Irving, J.; Farmer, C.K. Older people remain on blood pressure agents despite being hypotensive resulting in increased mortality and hospital admission. Age Ageing 2016, 45, 783–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brignole, M.; Russo, V.; Arabia, F.; Oliveira, M.; Pedrote, A.; Aerts, A.; Rapacciuolo, A.; Boveda, S.; Deharo, J.C.; Maglia, G.; et al. Cardiac pacing in severe recurrent reflex syncope and tilt-induced asystole. Eur. Heart J. 2021, 42, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Moonen, J.E.F.; Foster-Dingley, J.C.; de Ruijter, W.; van der Grond, J.; de Craen, A.J.; van der Mast, R.C. Effect of discontinuation of antihypertensive medication on orthostatic hypotension in older persons with mild cognitive impairment: The DANTE Study Leiden. Age Ageing 2016, 45, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solari, D.; Tesi, F.; Unterhuber, M.; Gaggioli, G.; Ungar, A.; Tomaino, M.; Brignole, M. Stop vasodepressor drugs in reflex syncope: A randomised controlled trial. Heart 2017, 103, 449–455. [Google Scholar] [CrossRef]
- Van der Wardt, V.; Harrison, J.K.; Welsh, T.; Conroy, S.; Gladman, J. Withdrawal of antihypertensive medication: A systematic review. J. Hypertens. 2017, 35, 1742–1749. [Google Scholar] [CrossRef] [Green Version]
- Rivasi, G.; Brignole, M.; Rafanelli, M.; Bilo, G.; Pengo, M.F.; Ungar, A.; Parati, G. Blood pressure management in hypertensive patients with syncope: How to balance hypotensive and cardiovascular risk. J Hypertens. 2020, 38, 2356–2362. [Google Scholar] [CrossRef]
- Gibbons, C.H.; Schmidt, P.; Biaggioni, I.; Frazier-Mills, C.; Freeman, R.; Isaacson, S.; Karabin, B.; Kuritzky, L.; Lew, M.; Low, P.; et al. The recommendations of a consensus panel for the screening, diagnosis, and treatment of neurogenic orthostatic hypotension and associated supine hypertension. J. Neurol. 2017, 264, 1567–1582. [Google Scholar] [CrossRef] [Green Version]
- Verhaeverbeke, I.; Mets, T. Drug-induced orthostatic hypotension in the elderly: Avoiding its onset. Drug Saf. 1997, 17, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Ylitalo, R.; Kähönen, M.; Nieminen, T.; Kööbi, T.; Ylitalo, P.; Turjanmaa, V. Effects of a mononitrate; a beta1-blocker and a dihydropyridine calcium channel blocker on cardiovascular responsiveness to passive orthostasis: A placebo-controlled doubleblind study in normotensive volunteers. Arzneimittelforschung 2005, 55, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Mussi, C.; Ungar, A.; Salvioli, G.; Menozzi, C.; Bartoletti, A.; Giada, F.; Lagi, A.; Ponassi, I.; Re, G.; Furlan, R.; et al. Orthostatic hypotension as cause of syncope in patients older than 65 years admitted to emergency departments for transient loss of consciousness. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 801–806. [Google Scholar] [CrossRef] [Green Version]
- Milazzo, V.; Di Stefano, C.; Servo, S.; Crudo, V.; Fulcheri, C.; Maule, S.; Veglio, F. Drugs and Orthostatic Hypotension: Evidence from Literature. J. Hypertens. 2012, 1, 104. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.K.; Lord, S.R.; Sturnieks, D.L.; Delbaere, K.; Trollor, J.N.; Close, J.C. Angiotensin system-blocking medications are associated with fewer falls over 12 months in community-dwelling older people. J. Am. Geriatr. Soc. 2013, 61, 776–781. [Google Scholar] [CrossRef]
- Press, Y.; Punchik, B.; Freud, T. Orthostatic hypotension and drug therapy in patients at an outpatient comprehensive geriatric assessment unit. J. Hypertens. 2016, 34, 351–358. [Google Scholar] [CrossRef]
- Wojszel, Z.B.; Kasiukiewicz, A.; Magnuszewski, L. Health and Functional Determinants of Orthostatic Hypotension in Geriatric Ward Patients: A Retrospective Cross Sectional Cohort Study. J. Nutr. Health Aging 2019, 23, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Sica, D.A. Alpha1-adrenergic blockers: Current usage considerations. J. Clin. Hypertens. 2005, 7, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Chapple, C.R.; Montorsi, F.; Tammela, T.L.; Wirth, M.; Koldewijn, E.; Fernández, E.; European Silodosin Study Group. Silodosin therapy for lower urinary tract symptoms in men with suspected benign prostatic hyperplasia: Results of an international, randomized, double-blind, placebo- and active-controlled clinical trial performed in Europe. Eur. Urol. 2011, 59, 342–352. [Google Scholar] [CrossRef]
- Fedorowski, A.; Burri, P.; Juul-Möller, S.; Melander, O. A dedicated investigation unit improves management of syncopal attacks (Syncope Study of Unselected Population in Malmo—SYSTEMA I). Europace 2010, 12, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Canney, M.; O’Connell, M.D.; Murphy, C.M.; O’Leary, N.; Little, M.A.; O’Seaghdha, C.M.; Kenny, R.A. Single Agent Antihypertensive Therapy and Orthostatic Blood Pressure Behaviour in Older Adults Using Beat-to-Beat Measurements: The Irish Longitudinal Study on Ageing. PLoS ONE 2016, 11, e0146156. [Google Scholar] [CrossRef] [PubMed]
- Valbusa, F.; Labat, C.; Salvi, P.; Vivian, M.E.; Hanon, O.; Benetos, A.; PARTAGE investigators. Orthostatic hypotension in very old individuals living in nursing homes: The PARTAGE study. J. Hypertens. 2012, 30, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Juraschek, S.P.; Appel, L.J.; Miller, E.R.; Mukamal, K.J.; Lipsitz, L.A. Hypertension Treatment Effects on Orthostatic Hypotension and Its Relationship With Cardiovascular Disease. Hypertension 2018, 72, 986–993. [Google Scholar] [CrossRef]
- Fedorowski, A.; Burri, P.; Melander, O. Orthostatic hypotension in genetically related hypertensive and normotensive individuals. J. Hypertens. 2009, 27, 976–982. [Google Scholar] [CrossRef]
- Gaxatte, C.; Faraj, E.; Lathuillerie, O.; Salleron, J.; Deramecourt, V.; Pardessus, V.; Destailleur, M.H.; Boulanger, E.; Puisieux, F. Alcohol and psychotropic drugs: Risk factors for orthostatic hypotension in elderly fallers. J. Hum. Hypertens. 2017, 31, 299–304. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; O’Connell, M.D.; Finucane, C.; Soraghan, C.; Fan, C.W.; Kenny, R.A. Insights into the clinical management of the syndrome of supine hypertension–orthostatic hypotension (SH-OH): The Irish Longitudinal Study on Ageing (TILDA). BMC Geriatr. 2013, 13, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poon, I.O.; Braun, U. High prevalence of orthostatic hypotension and its correlation with potentially causative medications among elderly veterans. J. Clin. Pharm. Ther. 2005, 30, 173–178. [Google Scholar] [CrossRef]
- Oster, J.R.; Epstein, M. Use of centrally acting sympatholytic agents in the management of hypertension. Arch. Intern Med. 1991, 151, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Brunton, L.L.; Parker, K.L.; Blumenthal, D.K.; Buxton, I.L.O. Goodman and Gilman’s Manual of Pharmacology and Therapeutics, 12th ed.; The Mac Graw Hill Company: New York, NY, USA, 2011. [Google Scholar]
- Briggs, R.; Carey, D.; McNicholas, T.; Claffey, P.; Nolan, H.; Kennelly, S.P.; Kenny, R.A. The association between antidepressant use and orthostatic hypotension in older people: A matched cohort study. J. Am. Soc. Hypertens. 2018, 12, 597–604.e1. [Google Scholar] [CrossRef]
- Rivasi, G.; Kenny, R.A.; Ungar, A.; Romero-Ortuno, R. Effects of benzodiazepines on orthostatic blood pressure in older people. Eur. J. Intern. Med. 2020, 72, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.D. Clinical review and treatment of select adverse effects of dopamine receptor agonists in Parkinson’s disease. Drugs Aging 2010, 27, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Churchyard, A.; Mathias, C.J.; Lees, A.J. Selegiline-induced postural hypotension in Parkinson’s disease: A longitudinal study on the effects of drug withdrawal. Mov. Disord. 1999, 14, 246–251. [Google Scholar] [CrossRef]
- Chen, A.; Ashburn, M.A. Cardiac Effects of Opioid Therapy. Pain Med. 2015, 16, S27–S31. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Antihypertensive medications that may increase the risk of orthostatic hypotension.


{kind=link}
Table 1.
Causes of syncope, adapted from Moya A. et al. [1].
Table 1.
Causes of syncope, adapted from Moya A. et al. [1].
| Reflex syncope |
| Vasovagal (VVS) orthostatic VVS: standing, or less common sitting emotional: fear, pain, instrumentation, blood phobia pain triggers: peripheral or visceral |
| Situational micturition gastrointestinal stimulation cough, sneeze others (e.g., laughing, brass instrument playing, weight lifting, post-exercise) |
| Carotid sinus syncope |
| Orthostatic Syncope |
| Drug-induced orthostatic hypotension |
| Volume depletion Primary autonomic failure (pure autonomic failure, multiple system atrophy, Parkinson’s disease, dementia with Lewy bodies) |
| Secondary autonomic failure (diabetes, amyloidosis, spinal cord injuries, auto-immune autonomic neuropathy, paraneoplastic autonomic neuropathy, kidney failure) |
| Cardiac syncope |
| Arrhythmia as primary cause: Bradycardia:
|
| Structural disease: cardiac valvular disease, acute myocardial infarction/ischaemia, hypertrophic cardiomyopathy, cardiac masses (atrial myxoma) pericardial disease/tamponade, congenital anomalies of coronary arteries, prosthetic valves dysfunction. |
| Cardiopulmonary and great vessels |
| Pulmonary embolus, acute aortic dissection, pulmonary hypertension |
Table 2.
BP targets in patients with hypertension and treatment-related syncope, adapted from Rivasi et al. [31].
Table 2.
BP targets in patients with hypertension and treatment-related syncope, adapted from Rivasi et al. [31].
| Age < 70 | Age > 70 or Frailty | Disability | |
|---|---|---|---|
| Low syncope risk and high CV risk | 120–130 mmHg | 130–140 mmHg | <160 mmHg |
| High syncope risk and low CV risk | 130–140 mmHg |
Table 3.
Vaso-active drugs, adapted from Gibbons C.H. et al., 2017 [32].
Table 3.
Vaso-active drugs, adapted from Gibbons C.H. et al., 2017 [32].
| Classes of Drugs | Drugs |
|---|---|
| Dopaminergic agents | levodopa, dopamine agonists |
| Antidepressant | amytriptiline, nortryptiline, imipramine, desipramine |
| Anticholinergics | atropine, glycopyrrolate, hyoscyamine |
| Antihypertensives | |
| Diuretics | furosemide, torsemide, acetazolamide, spironolactone, hydrochlorothiazide |
| Nitrates | nitroprusside, isosorbide dinitrate, nitroglycerin |
| Phosphodiesterase E5 inhibitors | sildenafil, vardenafil, tadalafil |
| Alpha-1 adrenergic antagonists | alfuzosin, doxazosin, tamsulosin |
| Dihydropyridine calcium channel blockers | amlodipine, nifedipine, nicardipin |
| Other direct vasodilators | hydralazine, medoxidil |
| Negative inotropic/chronotropic agents | |
| Beta-adrenergic blockers | metroprolol, propranolo, atenolol, bisoprolol, etc. |
| Non dihydropyridine calcium channel blockers | verapamil, diltiazem |
| Central sympatolytic agents | |
| Centrally acting alpha-2 agonists | clonidine |
| False neurotransmitters | alpha-methyldopa |
| Renine-angiotensin system (RAS) antagonists | |
| ACE inhibitors | captopril, enalapril, perindopril |
| ARB | losartan, telmisartan, candesartan |
Table 4.
Key points for the management of hypotensive medications in syncope.
| Key Points |
|---|
| 1. Considering the reduction or withdrawal of hypotensive medication. |
| 2. Considering changing molecules or therapy regimen (preferring bedtime administration, except for diuretics) when it is not possible to withdraw a hypotensive medication. |
| 3. Preferring selective beta-blockers instead of alpha- and beta-receptor blockers, when indicated. |
| 4. Preferring uro-selective alpha-lytics in patients with BPH-associated LUTS (e.g., silodosin), when indicated. |
| 5. Avoiding diuretics, unless specifically indicated as essential. |
| 6. Considering renal and hepatic impairment in order to avoid drug accumulation. |
BPH: benign prostatic hyperplasia; LUTS: low urinary tract symptoms.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rafanelli, M.; Testa, G.D.; Rivasi, G.; Ungar, A. Evaluation of Patients with Syncope in the Emergency Department: How to Adjust Pharmacological Therapy. Medicina 2021, 57, 603. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060603
AMA Style
Rafanelli M, Testa GD, Rivasi G, Ungar A. Evaluation of Patients with Syncope in the Emergency Department: How to Adjust Pharmacological Therapy. Medicina. 2021; 57(6):603. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060603
Chicago/Turabian StyleRafanelli, Martina, Giuseppe Dario Testa, Giulia Rivasi, and Andrea Ungar. 2021. "Evaluation of Patients with Syncope in the Emergency Department: How to Adjust Pharmacological Therapy" Medicina 57, no. 6: 603. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060603