
Recognition in Emergency Department of Septic Patients at Higher Risk of Death: Beware of Patients without Fever

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Data Collection
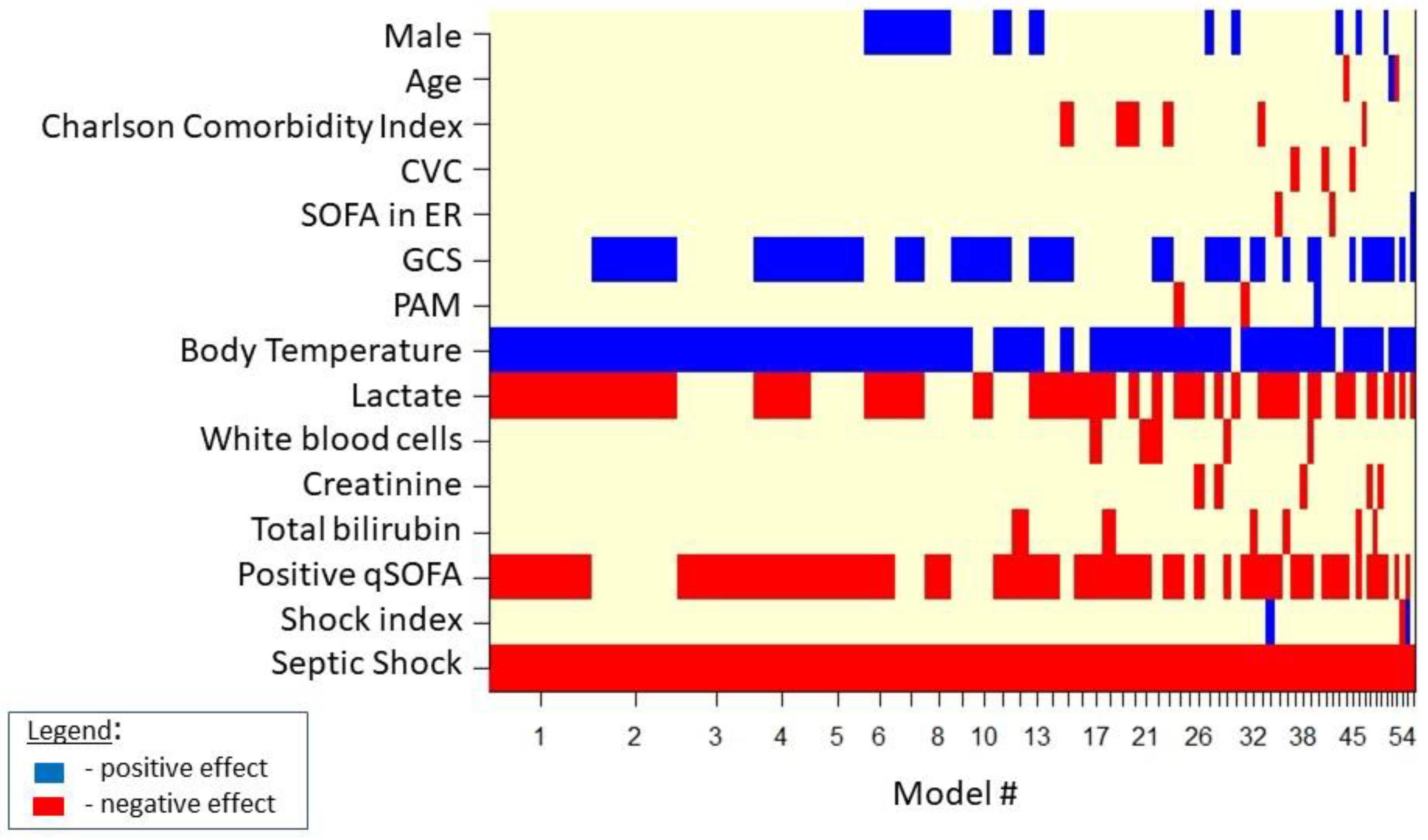
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleischmann, M.C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- Tusgul, S.; Carron, P.-N.; Yersin, B.; Calandra, T.; Dami, F. Low sensitivity of qSOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bone, R.; Balk, R.; Cerra, F.; Dellinger, R.; Fein, A.; Knaus, W.; Schein, R.; Sibbald, W. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The accp/sccm consensus conference committee. american college of chest physicians/society of crit care med. Chest 1992, 101 (Suppl. S5), 1644–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G.; et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003, 29, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Developing a new definition and assessing new clinical criteria for septic shock: For the third international consensus Definitions for sepsis and septic shock (sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]
- Jacob, J.A. New sepsis diagnostic guidelines shift focus to organ dysfunction. JAMA 2016, 315, 739–740. [Google Scholar] [CrossRef]
- Dellinger, R.P.; The Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup*; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef]
- Hayden, G.E.; Tuuri, R.E.; Scott, R.; Losek, J.D.; Blackshaw, A.M.; Schoenling, A.J.; Nietert, P.J.; Hall, G.A. Triage sepsis alert and sepsis protocol lower times to fluids and antibiotics in the ed. Am. J. Emerg. Med. 2016, 34, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Giorgi-Pierfranceschi, M. Sepsis and septic shock: A practical management according to Sepsis-3 diagnostic criteria. Ital. J. Med. 2016, 10, 376. [Google Scholar] [CrossRef] [Green Version]
- Singer, A.J.; Ng, J.; Thode, H.C., Jr.; Spiegel, R.; Weingart, S. Quick sofa scores predict mortality in adult emergency department patients with and without suspected infection. Ann. Emerg. Med. 2017, 69, 475–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khwannimit, B.; Bhurayanontachai, R.; Vattanavanit, V. Comparison of the performance of SOFA, qSOFA and SIRS for predicting mortality and organ failure among sepsis patients admitted to the intensive care unit in a middle-income country. J. Crit. Care 2018, 44, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Finkelsztein, E.J.; Jones, D.S.; Ma, K.C.; Pabón, M.A.; Delgado, T.; Nakahira, K.; Arbo, J.E.; Berlin, D.A.; Schenck, E.J.; Choi, A.M.K.; et al. Comparison of qSOFA and SIRS for predicting adverse outcomes of patients with suspicion of sepsis outside the intensive care unit. Crit. Care 2017, 21, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freund, Y.; Lemachatti, N.; Krastinova, E.; Van Laer, M.; Claessens, Y.-E.; Avondo, A.; Occelli, C.; Feral-Pierssens, A.-L.; Truchot, J.; Ortega, M.; et al. Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients With Suspected Infection Presenting to the Emergency Department. JAMA 2017, 317, 301–308. [Google Scholar] [CrossRef]
- Raith, E.; Udy, A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqui, S.; Chua, M.; Kumaresh, V.; Choo, R. A comparison of pre icu admission sirs, ews and q sofa scores for predictingmortality and length of stay in icu. J. Crit. Care 2017, 41, 191–193. [Google Scholar] [CrossRef]
- Serafim, R.; Gomes, J.A.; Salluh, J.; Povoa, P. A comparison of the quick-sofa and systemic inflammatory response syndrome criteria for the diagnosis of sepsis and prediction of mortality: A systematic review and meta-analysis. Chest 2018, 153, 646–655. [Google Scholar] [CrossRef]
- Gaieski, D.F.; Edwards, J.M.; Kallan, M.J.; Carr, B.G. Benchmarking the Incidence and Mortality of Severe Sepsis in the United States*. Crit. Care Med. 2013, 41, 1167–1174. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef]
- Rhodes, A.A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zhang, W.; Bakhai, A. Comparison of Bayesian model averaging and stepwise methods for model selection in logistic regression. Stat. Med. 2004, 23, 3451–3467. [Google Scholar] [CrossRef] [PubMed]
- Rivers, E.; Nguyen, B.; Havstad, S.; Ressler, J.; Muzzin, A.; Knoblich, B.; Peterson, E.; Tomlanovich, M. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. New Engl. J. Med. 2001, 345, 1368–1377. [Google Scholar] [CrossRef] [Green Version]
- Osborn, T.M.; Nguyen, H.B.; Rivers, E.P. Emergency Medicine and the Surviving Sepsis Campaign: An International Approach to Managing Severe Sepsis and Septic Shock. Ann. Emerg. Med. 2005, 46, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Prescott, H.C.; Langa, K.M.; Iwashyna, T. Readmission Diagnoses After Hospitalization for Severe Sepsis and Other Acute Medical Conditions. JAMA 2015, 313, 1055–1057. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of clinical criteria for sepsis: For the third international consensus Definitions for sepsis and septic shock (sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Daniels, R.; Nutbeam, T.; McNamara, G.; Galvin, C. The sepsis six and the severe sepsis resuscitation bundle: A prospective observational cohort study. Emerg. Med. J. 2010, 28, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef]
- Kluger, M.J.; Kozak, W.; Conn, C.A.; Leon, L.R.; Soszynski, D. THE ADAPTIVE VALUE OF FEVER. Infect. Dis. Clin. North Am. 1996, 10, 1–20. [Google Scholar] [CrossRef]
- Mackowiak, P.A. Fever: Blessing or curse? a unify-ing hypothesis. Ann. Intern. Med. 1994, 120, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Rumbus, Z.; Matics, R.; Hegyi, P.; Zsiboras, C.; Szabo, I.; Illes, A.; Petervari, E.; Balasko, M.; Marta, K.; Miko, A.; et al. Fever Is Associated with Reduced, Hypothermia with Increased Mortality in Septic Patients: A Meta-Analysis of Clinical Trials. PLoS ONE 2017, 12, e0170152. [Google Scholar] [CrossRef] [Green Version]
- Kushimoto, S.; Gando, S.; Saitoh, D.; Mayumi, T.; Ogura, H.; Fujishima, S.; Araki, T.; Ikeda, H.; Kotani, J.; Miki, Y.; et al. The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: An analysis from a multicenter, prospective survey of severe sepsis. Crit. Care 2013, 17, R271. [Google Scholar] [CrossRef] [Green Version]
- Henning, D.J.; Carey, J.R.; Oedorf, K.; Day, D.E.; Redfield, C.S.; Huguenel, C.J.; Roberts, J.C.; Sanchez, L.D.; Wolfe, R.E.; Shapiro, N.I. The absence of fever is associated with higher mortality and decreased antibiotic and iv fluid administration in emergency department patients with suspected septic shock. Crit. Care Med. 2017, 45, e575–e582. [Google Scholar] [CrossRef]
- Drewry, A.; Ablordeppey, E.; Murray, E.; Fuller, B.; Kollef, M.; Hotchkiss, R. 1483: Monocyte function and clinical outcomes in febrile and afebrile patients with severe sepsis. Crit. Care Med. 2018, 46, 725. [Google Scholar] [CrossRef]


{kind=link}
| Over All (n 1014) | Controls (n 363) | Sepsis (n 651) | p | |
|---|---|---|---|---|
| Gender (male) | 537 (53.0%) | 180 (49.6%) | 357 (54.8%) | 0.123 |
| Age (years) | 77.7 ± 13.5 | 77.6 ± 13.4 | 77.8 ± 13.5 | 0.857 |
| Hospital admission | 926 (91.3%) | 311 (85.7%) | 615 (94.5%) | <0.001 |
| ICU admission | 68 (6.7%) | 19 (5.2%) | 49 (7.5%) | 0.205 |
| ED discharge | 65 (6.4%) | 50 (13.8%) | 15 (2.3%) | <0.001 |
| Death in ED | 23 (2.3%) | 2 (0.56%) | 21 (3.2%) | 0.012 |
| Death during hospitalization | 161 (15.9%) | 30 (9.7%) | 131 (20.1%) | 0.001 |
| Charlson Comorbidity Index | 2 (1.0–4.0) | 2 (1–4) | 2 (1–4) | 0.239 |
| Cardiovascular disease | 550 (54.2%) | 208 (57.3%) | 342 (52.5%) | 0.163 |
| Renal insufficiency | 23 (2.3%) | 9 (2.5%) | 14 (2.2%) | 0.907 |
| Diabetes | 250 (24.7%) | 105 (28.9%) | 145 (22.3%) | 0.023 |
| COPD | 176 (17.4%) | 104 (28.7%) | 72 (11.1%) | <0.001 |
| Prosthetic device | 157 (15.5%) | 73 (20.1%) | 84 (12.9%) | 0.003 |
| Chronic hepatopathy | 46 (4.5%) | 18 (5.0%) | 28 (4.3%) | 0.745 |
| Immunosuppression | 88 (8.7%) | 33 (9.1%) | 55 (8.5%) | 0.817 |
| Cancer | 145 (14.3%) | 66 (18.2%) | 79 (12.1%) | 0.011 |
| Steroid therapy (in 30 days) | 154 (15.2%) | 77 (21.2%) | 77 (11.8%) | <0.001 |
| Trauma (in 30 days) | 51 (5.0%) | 11 (3.0%) | 40 (6.1%) | 0.043 |
| Surgery (in 30 days) | 37 (3.7%) | 3 (0.8%) | 34 (5.2%) | 0.001 |
| Presence of CVC | 62 (6.1%) | 7 (1.9%) | 55 (8.5%) | <0.001 |
| Presence of urinary catheter | 112 (11.1%) | 12 (3.3%) | 100 (15.7%) | <0.001 |
| Body temperature (°C) | 37.6 ± 1.2 | 36.9 ± 1.0 | 37.8 ± 1.2 | <0.001 |
| MAP | 119.2 ± 41.8 | 152.8 ± 33.8 | 101.0 ± 33.7 | <0.001 |
| GCS | 13.7 ± 3.0 | 14.2 ± 2.5 | 13.3 ± 3.2 | <0.001 |
| Septic shock | 96 (9.5%) | 0 (0.0%) | 96 (14.8%) | <0.001 |
| Shock index | 0.8 ± 0.3 | 0.7 ± 0.2 | 0.9 ± 0.3 | <0.001 |
| Positive qSOFA | 277 (27.3%) | 24 (8.1%) | 253 (38.9%) | <0.001 |
| SOFA score | 3 (2.0–5.0) | 2 (2–4) | 4 (3–6) | <0.001 |
| Lactate (mmol/L) | 1.6 (1.0–2.9) | 1.2 (0.8–1.9) | 2.1 (1.2–3.8) | <0.001 |
| WBC (/mmc) | 11.9 (8.4–16.9) | 10.0 (7.3–13.3) | 13.4 (9.3–19.6) | <0.001 |
| PCT (ng/mL) | 1.4 (0.3–7.8) | 0.1 (0.1–0.2) | 2.9 (0.9–13.1) | <0.001 |
| Creatinine (mg/dl) | 1.2 (0.8–1.8) | 1.0 (0.8–1.4) | 1.3 (0.9–2.1) | <0.001 |
| Bilirubin (mg/dl) | 0.8 (0.5–1.2) | 0.5 (0.3–0.9) | 0.9 (0.6–1.3) | <0.001 |
| Platelet count (/mmc) | 213 (153–293) | 226.5 (178–291) | 200 (142–293) | <0.001 |
| Variable | OR | 95% CI OR | p (B! = 0) |
|---|---|---|---|
| Male | 0.902 | 0.874–0.931 | 17 |
| Age | 1.000 | 0.999–1.001 | 1.8 |
| Charlson Comorbidity Index | 1.008 | 1.004–1.013 | 6.9 |
| CVC | 1.009 | 0.997–1.021 | 2.3 |
| SOFA score | 1.001 | 0.999–1.002 | 2.2 |
| GCS | 0.936 | 0.928–0.944 | 51.6 |
| PAM | 1.000 | 0.999–1.000 | 2.8 |
| Body Temperature | 0.687 | 0.673–0.701 | 92.5 |
| Lactate | 1.107 | 1.095–1.120 | 63.7 |
| White blood cells | 1.001 | 1.000–1.002 | 5.7 |
| Creatinine | 1.004 | 1.001–1.007 | 4.1 |
| Total bilirubin | 1.011 | 1.004–1.017 | 6.4 |
| Positive qSOFA | 2.144 | 2.002–2.297 | 71.7 |
| Shock index | 0.995 | 0.985–1.005 | 2 |
| Septic Shock | 6.582 | 6.289–6.88 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sozio, E.; Bertini, A.; Bertolino, G.; Sbrana, F.; Ripoli, A.; Carfagna, F.; Giacinta, A.; Viaggi, B.; Meini, S.; Ghiadoni, L.; et al. Recognition in Emergency Department of Septic Patients at Higher Risk of Death: Beware of Patients without Fever. Medicina 2021, 57, 612. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060612
Sozio E, Bertini A, Bertolino G, Sbrana F, Ripoli A, Carfagna F, Giacinta A, Viaggi B, Meini S, Ghiadoni L, et al. Recognition in Emergency Department of Septic Patients at Higher Risk of Death: Beware of Patients without Fever. Medicina. 2021; 57(6):612. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060612
Chicago/Turabian StyleSozio, Emanuela, Alessio Bertini, Giacomo Bertolino, Francesco Sbrana, Andrea Ripoli, Fabio Carfagna, Alessandro Giacinta, Bruno Viaggi, Simone Meini, Lorenzo Ghiadoni, and et al. 2021. "Recognition in Emergency Department of Septic Patients at Higher Risk of Death: Beware of Patients without Fever" Medicina 57, no. 6: 612. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060612