
The Dilemma of Falls in Older Persons: Never Forget to Investigate the Syncope

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solbiati, M.; Sheldon, R.; Seifer, C. Managing Syncope in the Elderly: The Not so Simple Faint in Aging Patients. Can. J. Cardiol. 2016, 32, 1124–1131. [Google Scholar] [CrossRef]
- Bhangu, J.; Hall, P.; Devaney, N.; Bennett, K.; Carroll, L.; Kenny, R.A.; McMahon, C.G. The Prevalence of Unexplained Falls and Syncope in Older Adults Presenting to an Irish Urban Emergency Department. Eur. J. Emerg. Med. 2019, 26, 100–104. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Josephson, K.R. The Epidemiology of Falls and Syncope. Clin. Geriatr. Med. 2002, 18, 141–158. [Google Scholar] [CrossRef]
- Ungar, A.; Mussi, C.; Ceccofiglio, A.; Bellelli, G.; Nicosia, F.; Bo, M.; Riccio, D.; Martone, A.M.; Guadagno, L.; Noro, G.; et al. Etiology of Syncope and Unexplained Falls in Elderly Adults with Dementia: Syncope and Dementia (SYD) Study. J. Am. Geriatr. Soc. 2016, 64, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Galizia, G.; Abete, P.; Mussi, C.; Noro, G.; Morrione, A.; Langellotto, A.; Landi, A.; Cacciatore, F.; Masotti, G.; Rengo, F.; et al. Role of Early Symptoms in Assessment of Syncope in Elderly People: Results from the Italian Group for the Study of Syncope in the Elderly. J. Am. Geriatr. Soc. 2009, 57, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Rafanelli, M.; Ruffolo, E.; Chisciotti, V.M.; Brunetti, M.A.; Ceccofiglio, A.; Tesi, F.; Morrione, A.; Marchionni, N.; Ungar, A. Clinical Aspects and Diagnostic Relevance of Neuroautonomic Evaluation in Patients with Unexplained Falls. Aging Clin. Exp. Res. 2014, 26, 33–37. [Google Scholar]
- Kenny, R.A. Syncope in the Elderly: Diagnosis, Evaluation, and Treatment. J. Cardiovasc. Electrophysiol. 2003, 14, S74–S77. [Google Scholar] [CrossRef]
- Shaw, F.E.; Kenny, R.A. The Overlap between Syncope and Falls in the Elderly. Postgrad. Med. J. 1997, 73, 635–639. [Google Scholar]
- Faul, M.; Stevens, J.A.; Sasser, S.M.; Alee, L.; Deokar, A.J.; Kuhls, D.A.; Burke, P.A. Older Adult Falls seen by Emergency Medical Service Providers: A Prevention Opportunity. Am. J. Prev. Med. 2016, 50, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-Based Injury Statistics Query and Reporting System (WISQARS). Available online: http://www.cdc.gov/injury/wisqars/ (accessed on 1 July 2020).
- Roudsari, B.S.; Ebel, B.E.; Corso, P.S.; Molinari, N.A.; Koepsell, T.D. The acute medical care costs of fall-related injuries among the U.S. older adults. Injury 2005, 36, 1316–1322. [Google Scholar] [CrossRef]
- De Ruiter, S.C.; Biesheuvel, S.S.; van Haelst, I.M.M.; van Marum, R.J.; Jansen, R.W.M.M. To STOPP or to START? Potentially Inappropriate Prescribing in Older Patients with Falls and Syncope. Maturitas 2020, 131, 65–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberger, Z.D.; Petek, B.J.; Brignole, M.; Shen, W.K.; Sheldon, R.S.; Solbiati, M.; Deharo, J.C.; Moya, A.; Hamdan, M.H. ACC/AHA/HRS Versus ESC Guidelines for the Diagnosis and Management of Syncope: JACC Guideline Comparison. J. Am. Coll. Cardiol. 2019, 74, 2410–2423. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. G2018 ESC Guidelines for the Diagnosis and Management of Syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D.; Grubb, B.P.; Hamdan, M.H.; Krahn, A.D.; Link, M.S.; et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients with Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2017, 136, e60–e122. [Google Scholar] [PubMed]
- Reed, M.J. Approach to Syncope in the Emergency Department. Emerg. Med. J. 2019, 36, 108–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perego, F.; Costantino, G.; Dipaola, F.; Scannella, E.; Borella, M.; Galli, A.; Barbic, F.; Casella, F.; Solbiati, M.; Angaroni, L.; et al. Predictors of Hospital Admission After Syncope: Relationships with Clinical Risk Scores. Int. J. Cardiol. 2012, 161, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Costantino, G.; Perego, F.; Dipaola, F.; Borella, M.; Galli, A.; Cantoni, G.; Dell’Orto, S.; Dassi, S.; Filardo, N.; Duca, P.G.; et al. Short- and Long-Term Prognosis of Syncope, Risk Factors, and Role of Hospital Admission: Results from the STePS (Short-Term Prognosis of Syncope) Study. J. Am. Coll. Cardiol. 2008, 51, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Galizia, G.; Balestrieri, G.; De Maria, B.; Lastoria, C.; Monelli, M.; Salvaderi, S.; Romanelli, G.; Dalla Vecchia, L.A. Role of Rehabilitation in the Elderly After an Acute Event: Insights from a Real-Life Prospective Study in the Subacute Care Setting. Eur. J. Phys. Rehabil. Med. 2018, 54, 934–938. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Conwell, Y.; Forbes, N.T.; Cox, C.; Caine, E.D. Validation of a measure of physical illness burden at autopsy: The Cumulative Illness Rating Scale. J. Am. Geriatr. Soc. 1993, 41, 38–41. [Google Scholar] [CrossRef]
- Carpenter, C.R.; Cameron, A.; Ganz, D.A.; Liu, S. Older Adult Falls in Emergency Medicine: 2019 Update. Clin. Geriatr. Med. 2019, 35, 205–219. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | T-LOC | UF | AF | |
|---|---|---|---|---|
| n = 100 | n = 36 | n = 37 | n = 27 | |
| Age, yrs | 78.4 ± 4.5 | 83.0 ± 1.4 ** | 77.0 ± 3.2 | 74.2 ± 3.1 |
| Sex (women), n (%) | 61 (61) | 24 (67) | 20 (54) | 17 (62) |
| Witness, n (%) | 21 (21) | 8 (22) | 0 (0) * | 13 (48) |
| Previous syncope, n (%) | 12 (12) | 10 (28) * | 2 (5) | 0 (0) |
| Medical Dept, n (%) | 30 (30) | 13 (36) * | 12 (32) * | 5 (18) |
| Surgical Dept, n (%) | 70 (70) | 23 (63) | 24 (64) | 23 (85) |
| Fracture, n (%) | 46 (46) | 18 (50) | 10 (27) * | 18 (67) |
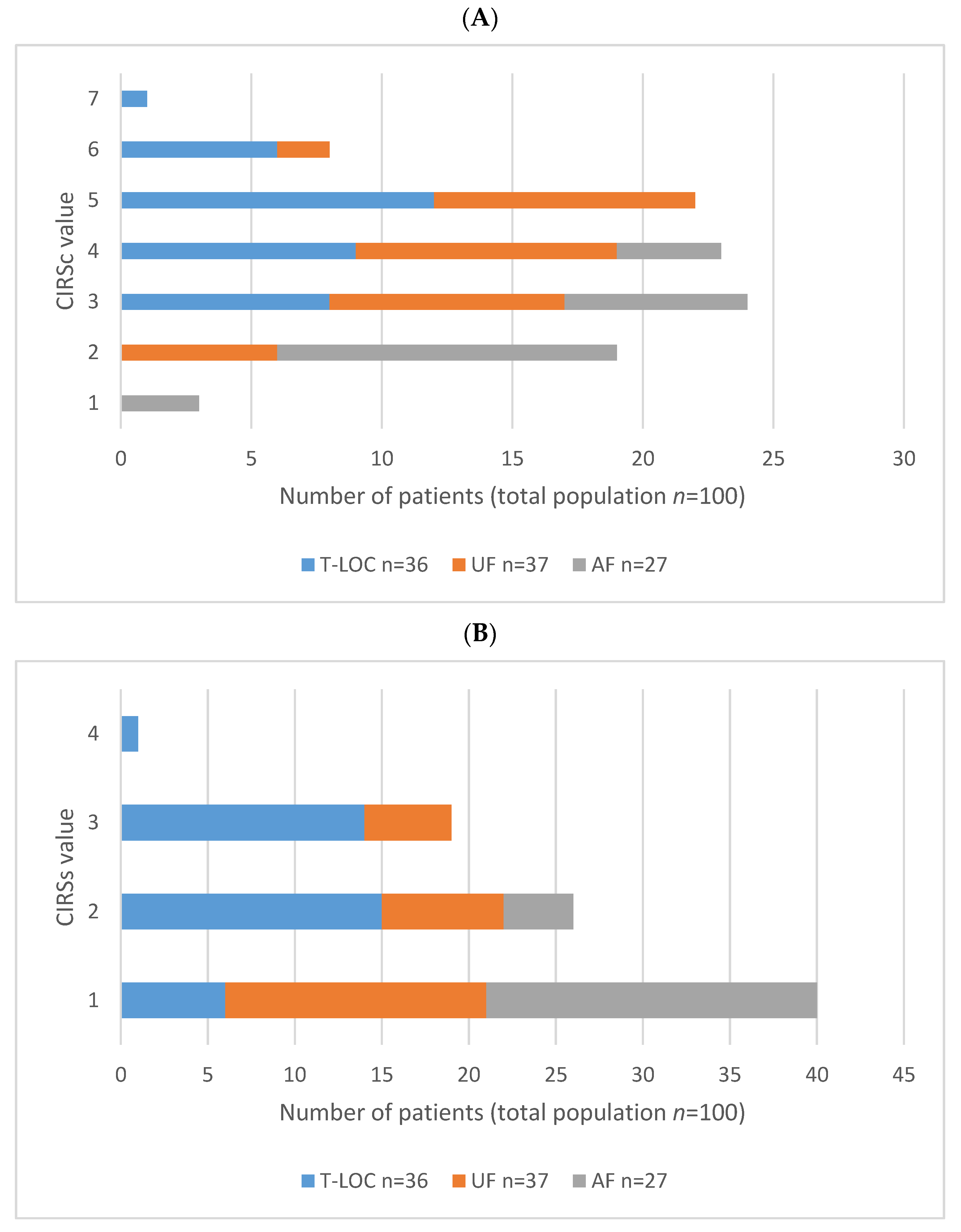
| CIRSc ≥ 4, n (%) | 58 (58) | 28 (78) ** | 26 (70) ** | 4 (15) |
| CIRSs ≥ 2, n (%) | 20 (20) | 15 (42) ** | 5 (14) | 0 (0) |
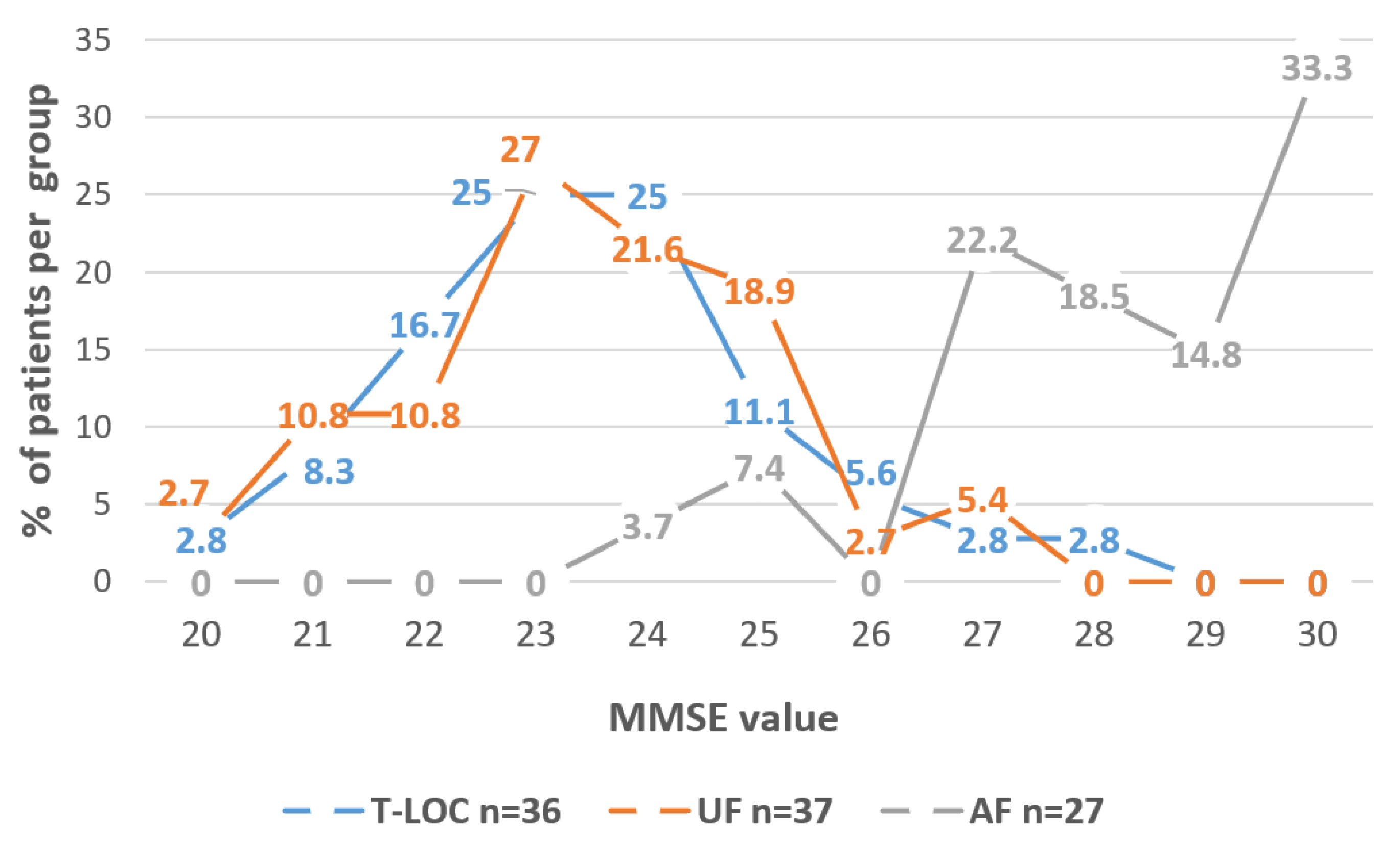
| MMSE, score | 24.8 ± 2.7 | 23.5 ± 1.7 ** | 23.5 ± 1.6 ** | 28.2 ± 1.7 |
| Heart Rate, bpm | 73 ± 11 | 74 ± 15 | 74 ± 8 | 70 ± 8 |
| Abnormal ECG, n (%) | 55 (55) | 27 (75) ** | 24 (65) ** | 4 (15) |
| OH, n (%) | 69 (69) | 29 (81) ** | 31 (84) ** | 9 (33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perego, F.; De Maria, B.; Bagnara, L.; De Grazia, V.; Monelli, M.; Cesari, M.; Dalla Vecchia, L.A. The Dilemma of Falls in Older Persons: Never Forget to Investigate the Syncope. Medicina 2021, 57, 623. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060623
Perego F, De Maria B, Bagnara L, De Grazia V, Monelli M, Cesari M, Dalla Vecchia LA. The Dilemma of Falls in Older Persons: Never Forget to Investigate the Syncope. Medicina. 2021; 57(6):623. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060623
Chicago/Turabian StylePerego, Francesca, Beatrice De Maria, Laura Bagnara, Valeria De Grazia, Mauro Monelli, Matteo Cesari, and Laura Adelaide Dalla Vecchia. 2021. "The Dilemma of Falls in Older Persons: Never Forget to Investigate the Syncope" Medicina 57, no. 6: 623. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060623