
The Relationship between Affect Integration and Psychopathology in Patients with Personality Disorder: A Cross-Sectional Study

 , ,
, ,
Abstract
:1. Introduction
1.1. The Relationship between Emotional Dysfunction and Severity of Psychopathology in Individuals with Personality Disorders
1.2. The Present Study
- (1)
- Problems with AI are associated with symptom distress and overall relational difficulties.
- (2)
- Problems with AI for discrete affects are systematically and predictably associated with specific types of interpersonal problems (see the statistical section for further elaboration of the expected relations on page 5).
- (3)
- Problems with AI are associated with the severity of personality dysfunction.
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Affect Integration Inventory
2.3.2. The Symptom Checklist-90, Revised (SCL-90-R)
2.3.3. Inventory of Interpersonal Problems 64 Circumplex Version (IIP-64)
2.3.4. The Severity Indices of Personality Problems
2.4. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of the Sample
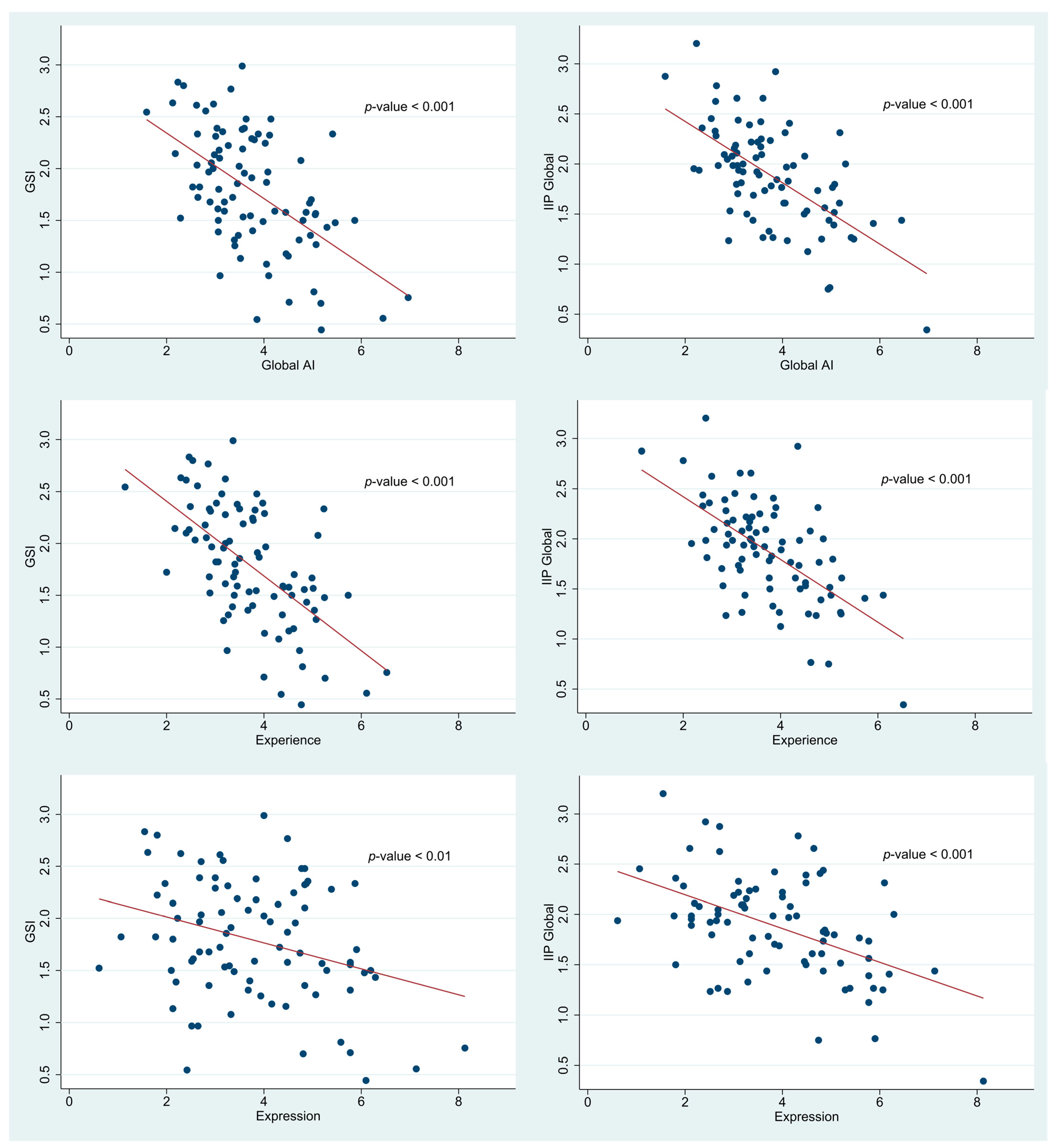
3.2. Relationships between Affect Integration, Symptom Distress, and Relational Difficulties
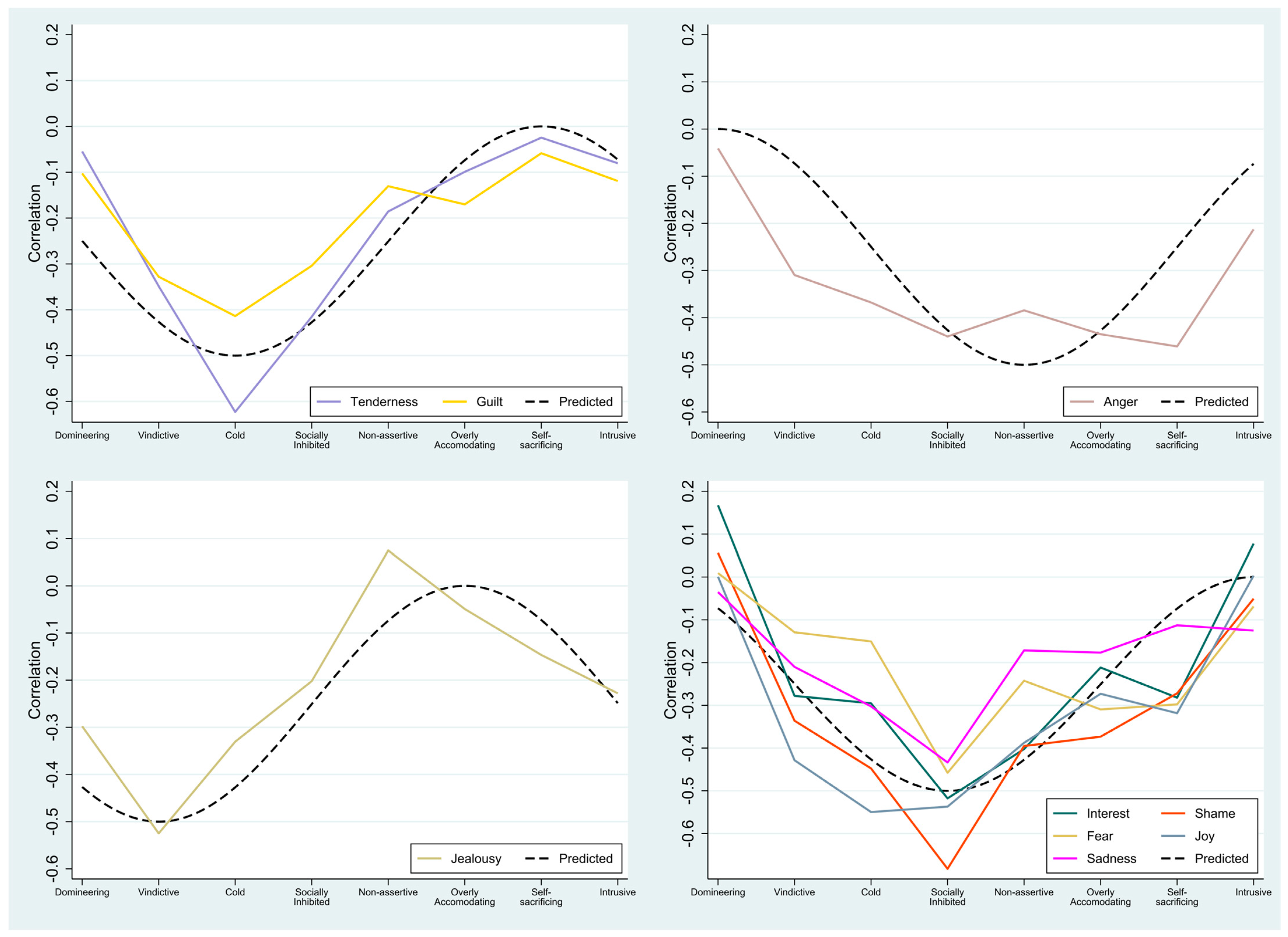
3.3. Patterns of Relationships between AI for Discrete Affects and Specific Types of Interpersonal Problems
3.4. Relationship between AI and Personality Functioning
4. Discussion
4.1. AI and Symptom Distress
4.2. AI and General Interpersonal Problems
4.3. AI and Specific Types of Interpersonal Problems
4.4. AI and Personality Functioning
4.5. AI as a Core Mechanism in the Development of Symptoms, Personality Pathology and Interpersonal Problems
4.6. AI as a Mechanism of Change in Psychotherapy
4.7. Implications for the Field of Knowledge—Generalizing between AI and Related Constructs of Emotional Dysfunction
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; 171p. [Google Scholar]
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics; 11th Revision. 2018. Available online: https://icd.who.int/browse11/l-m/en (accessed on 1 May 2021).
- Bach, B.; First, M.B. Application of the ICD-11 classification of personality disorders. BMC Psychiatry 2018, 18, 351. [Google Scholar] [CrossRef] [Green Version]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The twenty-item Toronto Alexithymia scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Lesser, I.M. A Review of the Alexithymia Concept. Psychosom. Med. 1981, 43, 531–543. [Google Scholar] [CrossRef]
- Monsen Eilertsen, D.E.; Melgård, T.; Ødegård, P. Affects and affect consciousness: Initial experiences with the assessment of affect integration. J. Psychother. Pract. Res 1996, 5, 238–249. [Google Scholar]
- Stolorow, R.D.; Atwood, G.E.; Brandchaft, B. Psychoanalytic Treatment: An Intersubjective Approach; Psychoanalytic Inquiry Book Series; Analytic Press: Hillsdale, NJ, USA, 1987. [Google Scholar]
- Gross, J.J. Emotion regulation: Conceptual foundations. In Handbook of Emotion Regulation; Gross, J.J., Ed.; Guilford: New York, NY, USA, 2007; pp. 3–24. [Google Scholar]
- Lane, R.D.; Quinlan, D.M.; Schwartz, G.E.; Walker, P.A.; Zeitlin, S.B. The Levels of Emotional Awareness Scale: A Cognitive-Developmental Measure of Emotion. J. Pers. Assess. 1990, 55, 124–134. [Google Scholar] [CrossRef]
- Fonagy, P.; Gergely, G.; Target, M.; Jurist, E.L. Affect. Regulation, Mentalization, and the Development of the Self; Other Press: New York, NY, USA, 2002; Available online: https://books.google.dk/books?id=EDHi3N-ebykC (accessed on 1 May 2021).
- Jurist, E.L. Mentalized affectivity. Psychoanal. Psychol. 2005, 22, 426–444. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D. Emotional Intelligence. Imagin Cogn. Pers 1990, 9, 185–211. [Google Scholar] [CrossRef]
- Monsen Monsen, K. Affects an affect consciousness: A psychotherapy model integrating Silvan Tomkins’ affect- and script theory witin the framework of self psychology. In Pluralism in Self Psychology: Progress in Self Psychology; Goldberg, A., Ed.; Analytic Press: Hillsdale, NJ, USA, 1999; Volume 15, pp. 287–307. [Google Scholar]
- Krystal, H. The genetic development of affects and affect regression. Annu. Psychoanal. 1974, 2, 98–126. [Google Scholar]
- Solbakken, O.A.; Hansen, R.S.; Monsen, J.T. Affect integration and reflective function: Clarification of central conceptual issues. Psychother. Res. 2011, 21, 482–496. [Google Scholar] [CrossRef]
- Tomkins, S.S. Affect. Imagery Consciousness: The Complete Edition; Volumes I and II, Springer Publishing Company: New York, NY, USA, 2008. [Google Scholar]
- Tomkins, S.S. Affect. Imagery Consciousness: The Complete Edition; Volumes III and IV, Springer Publishing Company: New York, NY, USA, 2008. [Google Scholar]
- Monsen Monsen, K.; Solbakken, O.A.; Hansen, R.S. Affect Consciousness Interview (ACI) and the Affect Consciusness Scale (ACS): Instructions for the interview and rating; Department of Psychology, University of Oslo: Oslo, Norway, 2008. [Google Scholar]
- Solbakken, O.A.; Rauk, M.; Solem, A.; Lødrup, W.; Monsen, J.T. Tell me how you feel and I will tell you who you are: First validation of the affect integration inventory. Scand. Psychol. 2017, 4, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Taarvig, E.; Solbakken, O.A.; Grova, B.; Monsen, J.T. Affect Consciousness in children with internalizing problems: Assessment of affect integration. Clin. Child. Psychol. Psychiatry 2015, 20, 591–610. [Google Scholar] [CrossRef]
- Solbakken, O.A.; Hansen, R.S.; Havik, O.E.; Monsen, J.T. Affect integration as a predictor of change: Affect consciousness and treatment response in open-ended psychotherapy. Psychother. Res. 2012, 22, 656–672. [Google Scholar] [CrossRef] [PubMed]
- Solbakken, O.A.; Hansen, R.S.; Havik, O.E.; Monsen, J.T. Assessment of affect integration: Validation of the affect consciousness construct. J. Pers. Assess. 2011, 93, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Normann-Eide, E.; Johansen, M.S.; Normann-Eide, T.; Egeland, J.; Wilberg, T. Is low affect consciousness related to the severity of psychopathology? A cross-sectional study of patients with avoidant and borderline personality disorder. Compr. Psychiatry 2013, 54, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Lech, B.; Andersson, G.; Holmqvist, R. Consciousness about own and others’ affects: A study of the validity of a revised version of the Affect Consciousness Interview. Scand. J. Psychol 2008, 49, 515–521. [Google Scholar] [CrossRef]
- Lech, B.; Andersson, G.; Holmqvist, R. Affect Consciousness and Adult Attachment. Psychology 2012, 03, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Johansen, M.S.; Normann-Eide, E.; Normann-Eide, T.; Klungsøyr, O.; Kvarstein, E.H.; Wilberg, T. Relationship Between Affect Consciousness and Personality Functioning in Patients With Personality Disorders: A Prospective Study. J. Pers. Disord. 2016, 30, 633–652. [Google Scholar] [CrossRef]
- Frederiksen, C.; Solbakken, O.A.; Licht, R.W.; Christensen, A.-E.; Jørgensen, C.R.; Kjaersdam, G.T. Validation of the Affect Integration Inventory in a sample of patients with personality disorders: A cross sectional study. Manuscr Submitt Publ. 2021. [Google Scholar]
- Solbakken, O.A.; Monsen, J. Validation of a short form of the Affect Integration Inventory. Int J. Psychol. Psychol. Ther. 2021, 21, 107–122. [Google Scholar]
- First, M.B. User’s Guide for the Structured Clinical Interview for DSM—IV Axis II Personality Disorders—SCID II; American Psychiatric Press: Washington, DC, USA, 1997; 91 sider. [Google Scholar]
- Lech, B.; Holmqvist, R.; Andersson, G. Affect consciousness and eating disorders. Short term stability and subgroup characteristics. Eur. Eat. Disord. Rev. 2012, 20, e50–e55. [Google Scholar] [CrossRef]
- Bach, M.; de Zwaan, M.; Ackard, D.; Nutzinger, D.O.; Mitchell, J.E. Alexithymia: Relationship to personality disorders. Compr. Psychiatry 1994, 35, 239–243. [Google Scholar] [CrossRef]
- Derks, Y.P.M.J.; Westerhof, G.J.; Bohlmeijer, E.T. A Meta-analysis on the Association Between Emotional Awareness and Borderline Personality Pathology. J. Pers. Disord. 2016, 31, 362–384. [Google Scholar] [CrossRef]
- Fonagy, P.; Luyten, P.; Moulton-Perkins, A.; Lee, Y.W.; Warren, F.; Howard, S.; Ghinai, R.; Fearon, P.; Lowyck, B. Development and Validation of a Self-Report Measure of Mentalizing: The Reflective Functioning Questionnaire. PLoS ONE 2016, 11, e0158678. [Google Scholar] [CrossRef] [PubMed]
- Wupperman, P.; Neumann, C.S.; Whitman, J.B.; Axelrod, S.R. The Role of Mindfulness in Borderline Personality Disorder Features. J. Nerv. Ment. Dis. 2009, 197, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Kröger, C.; Vonau, M.; Kliem, S.; Kosfelder, J. Emotion Dysregulation as a Core Feature of Borderline Personality Disorder: Comparison of the Discriminatory Ability of Two Self-Rating Measures. Psychopathology 2011, 44, 253–260. [Google Scholar] [CrossRef]
- Leible, T.L.; Snell, W.E. Borderline personality disorder and multiple aspects of emotional intelligence. Pers. Individ. Dif. 2004, 37, 393–404. [Google Scholar] [CrossRef]
- Andrea, H.; Verheul, R.; Berghout, C.C.; Dolan, C.; van der Kroft, P.J.A.; Bateman, A.W.; Fonagy, P.; van Busschbach, J.J. Measuring the Core Components of Maladaptive Personality: Severity Indices of Personality Problems (SIPP-118); Report of the Viersprong Institute for Studies on Personality Disorders (VISPD) in Cooperation with the Department of Medical Psychology & Psychotherapy; Erasmus University Rotterdam: Burgemeester Oudlaan, The Netherlands, 2007. [Google Scholar]
- Committee, S.A. GlaxoSmithKlin. Present State Examination: Kort Version til Klinisk Brug, 3rd ed.; GlaxoSmithKline: Ballerup, Denmark, 2002; 128 sider. [Google Scholar]
- Derogatis, L.R. SCL-90-R: Symptom Checklist-90-R: Administration, Scoring and Procedures Manual; National Computer System: Minneapolis, MN, USA, 1994. [Google Scholar]
- Horowitz, L.M.; Alden, L.E.; Wiggins, J.S.; Pincus, A.L. Inventory of Interpersonal Problems Manual; The Psychological Corporation: Odessa, Ukraine, 2000. [Google Scholar]
- Tracey, T.; Rounds, J.; Gurtman, M. Examination of the General Factor with the Interpersonal Circumplex Structure: Application to the Inventory of Interpersonal Problems. Multivar. Behav. Res. 1996, 31, 441–466. [Google Scholar] [CrossRef]
- Monsen, J.T.; Hagtvet, K.A.; Havik, O.E.; Eilertsen, D.E. Circumplex structure and personality disorder correlates of the Interpersonal Problems model (IIP-C): Construct validity and clinical implications. Psychol. Assess. 2006, 18, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Bender, D.S.; Morey, L.C.; Skodol, A.E. Toward a Model for Assessing Level of Personality Functioning in DSM–5, Part I: A Review of Theory and Methods. J. Pers. Assess. 2011, 93, 332–346. Available online: http://www.tandfonline.com/doi/abs/10.1080/00223891.2011.583808 (accessed on 1 May 2021). [CrossRef]
- Bastiaansen, L.; De Fruyt, F.; Rossi, G.; Schotte, C.; Hofmans, J. Personality disorder dysfunction versus traits: Structural and conceptual issues. Pers. Disord. 2013, 4, 293–303. [Google Scholar] [CrossRef]
- Feenstra, D.J.; Hutsebaut, J.; Verheul, R.; Busschbach, J.J.V. Severity Indices of Personality Problems (SIPP-118) in adolescents: Reliability and validity. Psychol. Assess. 2011, 23, 646–655. [Google Scholar] [CrossRef] [Green Version]
- Verheul, R.; Andrea, H.; Berghout, C.C.; Dolan, C.; Busschbach, J.J.V.; van der Kroft, P.J.; Bateman, A.W.; Fonagy, P. Severity Indices of Personality Problems (SIPP-118): Development, Factor Structure, Reliability, and Validity. Psychol. Assess. 2008, 20, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnevik, E.; Wilberg, T.; Monsen, J.T.; Andrea, H.; Karterud, S. A cross-national validity study of the Severity Indices of Personality Problems (SIPP-118). Personal Ment. Health 2009, 3, 41–55. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Bateman, A.W.; Fonagy, P.; Luyten, P. Handbook of Mentalizing in Mental Health Practice; Bateman, A.W., Fonagy, P., Eds.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2012; p. xxiii, 593. [Google Scholar]
- Izard, C.E. The Psychology of Emotions; Plenum Press: New York, NY, USA, 1991. [Google Scholar]
- Krystal, H. Integration and Self Healing: Affect, Trauma, Alexithymia; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Monsen, J.; Odland, T.; Faugli, A.; Daae, E.; Eilertsen, D.E. Personality Disorders: Changes and Stability after Intensive Psychotherapy Focusing on Affect Consciousness. Psychother. Res. 1995, 5, 33–48. [Google Scholar] [CrossRef]
- Monsen, K.; Monsen, J.T. Chronic pain and psychodynamic body therapy: A controlled outcome study. Psychother. Theory Res. Pract. Train. 2000, 37, 257–269. [Google Scholar] [CrossRef]
- Gude, T.; Monsen, J.T.; Hoffart, A. Schemas, Affect Consciousness, and Cluster C Personality Pathology: A Prospective One-Year Follow-Up Study of Patients in a Schema-Focused Short-Term Treatment Program. Psychother. Res. 2001, 11, 85–98. [Google Scholar] [CrossRef]
- Nordmo, M.; Sønderland, N.M.; Havik, O.E.; Eilertsen, D.-E.; Monsen, J.T.; Solbakken, O.A. Effectiveness of Open-Ended Psychotherapy Under Clinically Representative Conditions. Front. Psychiatry 2020, 11, 384. [Google Scholar] [CrossRef] [PubMed]
- Doss, B.D. Changing the Way We Study Change in Psychotherapy. Clin. Psychol. Sci. Pract. 2006, 11, 368–386. [Google Scholar] [CrossRef]
- Choi-Kain, L.W.; Gunderson, J.G. Mentalization: Ontogeny, Assessment, and Application in the Treatment of Borderline Personality Disorder. Am. J. Psychiatry 2008, 165, 1127–1135. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, D.M.; Kolasi, J.; Hegsted, C.P.; Berkowitz, Y.; Jurist, E.L. Mentalized affectivity: A new model and assessment of emotion regulation. PLoS ONE 2017, 12, e0185264. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age *,a | 31.7 (9.5) |
| Sex, female + | 74 (85.1%) |
| Married/cohabiting +,b | 49 (57.6%) |
| Completed high school +,b | 31 (36.5%) |
| Self-harm within the last three months +,b | 22 (25.9%) |
| Suicide attempt within the last three months +,c | <4% |
| Mood disorder +,b | 27 (31.0%) |
| Anxiety disorder +,b | 21 (24.1%) |
| Substance abuse +,b | 4 (4.6%) |
| Eating disorder +,b | 3 (3.4%) |
| Behavioural disorder +,b | 4 (4.6%) |
| Primary PD diagnosis + | |
| Borderline | 30 (34.5%) |
| Avoidant | 36 (41.4%) |
| Mixed | 15 (17.2%) |
| Other e | 6 (6.9%) |
| No. of PD-diagnoses * | 1.4 (0.6) |
| GSI *,a | 1.8 (0.6) |
| IIP-Global *,d | 1.9 (0.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frederiksen, C.; Solbakken, O.A.; Licht, R.W.; Jørgensen, C.R.; Rodrigo-Domingo, M.; Kjaersdam Telléus, G. The Relationship between Affect Integration and Psychopathology in Patients with Personality Disorder: A Cross-Sectional Study. Medicina 2021, 57, 627. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060627
Frederiksen C, Solbakken OA, Licht RW, Jørgensen CR, Rodrigo-Domingo M, Kjaersdam Telléus G. The Relationship between Affect Integration and Psychopathology in Patients with Personality Disorder: A Cross-Sectional Study. Medicina. 2021; 57(6):627. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060627
Chicago/Turabian StyleFrederiksen, Christina, Ole André Solbakken, Rasmus Wentzer Licht, Carsten René Jørgensen, Maria Rodrigo-Domingo, and Gry Kjaersdam Telléus. 2021. "The Relationship between Affect Integration and Psychopathology in Patients with Personality Disorder: A Cross-Sectional Study" Medicina 57, no. 6: 627. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060627