
Association of Urinary Dickkopf-3 with Residual Renal Function Decline in Patients Undergoing Peritoneal Dialysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Date and Sample Collection
2.2. Measurement of Urinary DKK-3
2.3. Statistical Analysis
3. Results
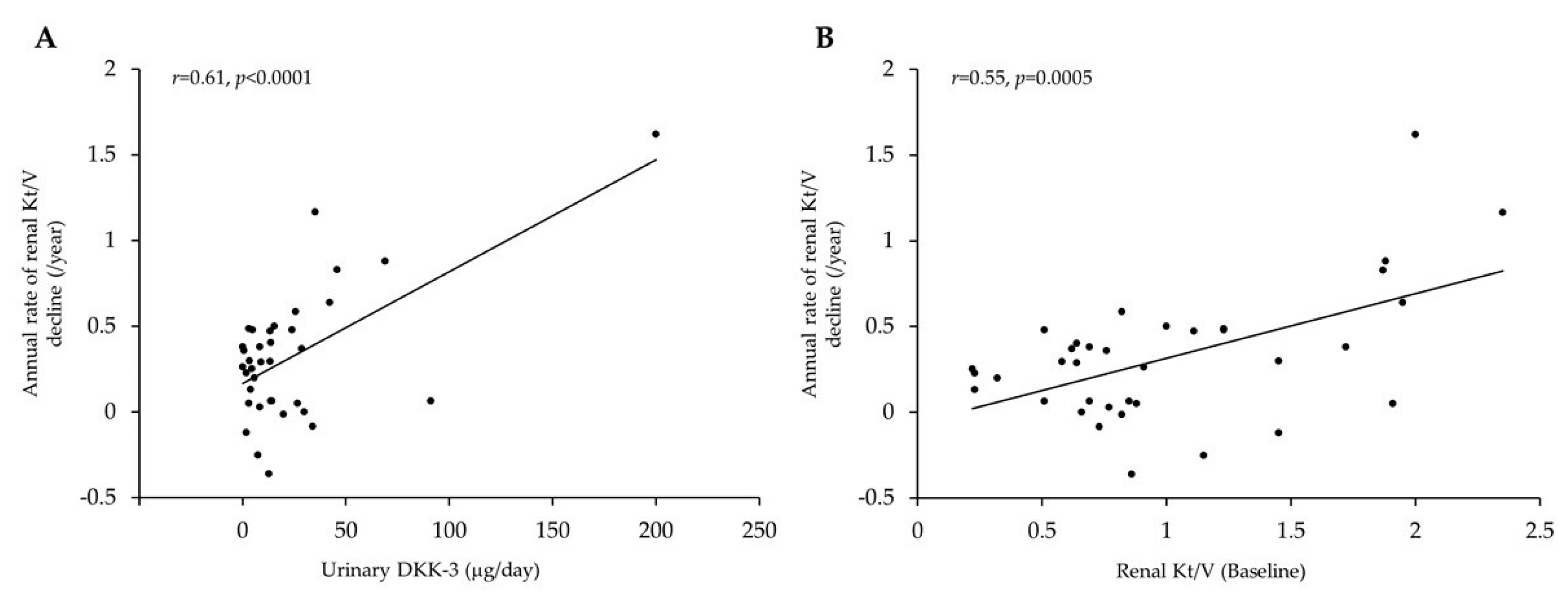
Factors Associated with RRF Decline in PD Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coresh, J. Update on the burden of CKD. J. Am. Soc. Nephrol. 2017, 28, 1020–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.Y.; Lai, K.N. The importance of residual renal function in dialysis patients. Kidney Int. 2006, 69, 1726–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Dai, C. Advances in understanding and management of residual renal function in patients with chronic kidney disease. Kidney Dis. 2017, 2, 187–196. [Google Scholar] [CrossRef]
- Liao, C.T.; Chen, Y.M.; Shiao, C.C.; Hu, F.C.; Huang, J.W.; Kao, T.W.; Chuang, H.F.; Hung, K.Y.; Wu, K.D.; Tsia, T. Rate of decline of residual renal function is associated with all-cause mortality and technique failure in patients on long-term peritoneal dialysis. Nephrol. Dial. Transpl. 2009, 24, 2909–2914. [Google Scholar] [CrossRef] [Green Version]
- Lang, S.M.; Bergner, A.; Töpfer, M.; Schiffl, H. Preservation of residual renal function in dialysis patients: Effects of dialysis-technique-related factors. Perit. Dial. Int. 2001, 21, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xie, X.; Yan, X.; Yang, X.; Zhang, X.; Chen, J.; Han, F. A fast decline of residual renal function in the first year is a predictor for early withdrawal from peritoneal dialysis in non-diabetic patients. Kidney Blood Press Res. 2019, 44, 12–21. [Google Scholar] [CrossRef]
- Termorshuizen, F.; Korevaar, J.C.; Dekker, F.W.; van Manen, J.G.; Boeschoten, E.W.; Krediet, R.T.; NECOSAD Study Group. The relative importance of residual renal function compared with peritoneal clearance for patient survival and quality of life: An analysis of the Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD)-2. Am. J. Kidney Dis. 2003, 41, 1293–1302. [Google Scholar] [CrossRef]
- Marrón, B.; Remón, C.; Pérez-Fontán, M.; Quirós, P.; Ortíz, A. Benefits of preserving residual renal function in peritoneal dialysis. Kidney Int. Suppl. 2008, 108, S42–S51. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Cho, K.H.; Park, J.W.; Yoon, K.W.; Do, J.Y. Proteinuria as a risk factor for decline in residual renal function in non-diabetic peritoneal dialysis patients. Kidney Blood Press Res. 2013, 37, 199–210. [Google Scholar] [CrossRef]
- Cho, Y.; Johnson, D.W.; Vesey, D.A.; Hawley, C.M.; Clarke, M.; Topley, N. Utility of urinary biomarkers in predicting loss of residual renal function: The balANZ Trial. Perit. Dial. Int. 2015, 35, 159–171. [Google Scholar] [CrossRef] [Green Version]
- Hidaka, H.; Nakao, T. Preservation of residual renal function and factors affecting its decline in patients on peritoneal dialysis. Nephrology 2003, 8, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.C.; Kwan, B.C.; Chow, K.M.; Chung, S.; Yu, V.; Cheng, P.M.; Leung, C.B.; Law, M.C.; Li, P.K. Predictors of residual renal function decline in patients undergoing continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 2015, 35, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Federico, G.; Meister, M.; Mathow, D.; Heine, G.H.; Moldenhauer, G.; Popovic, Z.V.; Nordström, V.; Kopp-Schneider, A.; Hielscher, T.; Nelson, P.J.; et al. Tubular Dickkopf-3 promotes the development of renal atrophy and fibrosis. JCI Insight 2016, 1, e84916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zewinger, S.; Rauen, T.; Rudnicki, M.; Federico, G.; Wagner, M.; Triem, S.; Schunk, S.J.; Petrakis, I.; Schmit, D.; Wagenpfeil, S.; et al. Dickkopf-3 (DKK3) in urine identifies patients with short-term risk of eGFR loss. J. Am. Soc. Nephrol. 2018, 29, 2722–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schunk, S.J.; Zarbock, A.; Meersch, M.; Küllmar, M.; Kellum, J.A.; Schmit, D.; Wagner, M.; Triem, S.; Wagenpfeil, S.; Gröne, H.J.; et al. Association between urinary dickkopf-3, acute kidney injury, and subsequent loss of kidney function in patients undergoing cardiac surgery: An observational cohort study. Lancet 2019, 394, 488–496. [Google Scholar] [CrossRef]
- Schunk, S.J.; Speer, T.; Petrakis, I.; Fliser, D. Dickkopf 3-a novel biomarker of the ‘kidney injury continuum’. Nephrol. Dial. Transpl. 2021, 36, 761–767. [Google Scholar] [CrossRef]
- Fang, X.; Hu, J.; Chen, Y.; Shen, W.; Ke, B. Dickkopf-3: Current knowledge in kidney diseases. Front. Physiol. 2020, 11, 533344. [Google Scholar] [CrossRef]
- Uchiyama, K.; Yanai, A.; Maeda, K.; Ono, K.; Honda, K.; Tsujimoto, R.; Kamijo, Y.; Yanagi, M.; Ishibashi, Y. Baseline and time-averaged values predicting residual renal function decline rate in Japanese peritoneal dialysis patients. Ther. Apher. Dial. 2017, 21, 599–605. [Google Scholar] [CrossRef]
- Seibert, F.S.; Heringhaus, A.; Pagonas, N.; Rohn, B.; Bauer, F.; Trappe, H.J.; Landmesser, U.; Babel, N.; Westhoff, T.H. Dickkopf-3 in the prediction of contrast media induced acute kidney injury. J. Nephrol. 2021, 34, 821–828. [Google Scholar] [CrossRef]
- MacDonald, B.T.; Tamai, K.; He, X. Wnt/beta-catenin signaling: Components, mechanisms, and diseases. Dev. Cell 2009, 17, 9–26. [Google Scholar] [CrossRef] [Green Version]
- Tan, R.J.; Zhou, D.; Zhou, L.; Liu, Y. Wnt/β-catenin signaling and kidney fibrosis. Kidney Int. Suppl. 2014, 4, 84–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, M.; Muragaki, Y.; Saika, S.; Roberts, A.B.; Ooshima, A. Targeted disruption of TGF-beta1/Smad3 signaling protects against renal tubulointerstitial fibrosis induced by unilateral ureteral obstruction. J. Clin. Investig. 2003, 112, 1486–1494. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Iturbe, B.; Johnson, R.J.; Herrera-Acosta, J. Tubulointerstitial damage and progression of renal failure. Kidney Int. Suppl. 2005, 99, S82–S86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nath, K.A. Tubulointerstitial changes as a major determinant in the progression of renal damage. Am. J. Kidney Dis. 1992, 20, 1–17. [Google Scholar] [CrossRef]
- Johnson, D.W.; Mudge, D.W.; Sturtevant, J.M.; Hawley, C.M.; Campbell, S.B.; Isbel, N.M.; Hollett, P. Predictors of decline of residual renal function in new peritoneal dialysis patients. Perit. Dial. Int. 2003, 23, 276–283. [Google Scholar] [CrossRef]
- Yang, C.; Ma, X.; Zhao, W.; Chen, Y.; Lin, H.; Luo, D.; Zhang, J.; Lou, T.; Peng, Y.; Peng, H. A longitudinal analysis of the relationship between serum uric acid and residual renal function loss in peritoneal dialysis patients. Ren. Fail. 2020, 42, 447–454. [Google Scholar] [CrossRef]
- Liu, X.Y.; Gao, X.M.; Zhang, N.; Chen, R.; Wu, F.; Tao, X.C.; Li, C.J.; Zhang, P.; Yu, P. Oral bicarbonate slows decline of residual renal function in peritoneal dialysis patients. Kidney Blood Press Res. 2017, 42, 565–574. [Google Scholar] [CrossRef]
- Tian, N.; Guo, Q.; Zhou, Q.; Cao, P.; Hong, L.; Chen, M.; Yang, X.; Yu, X. The impact of fluid overload and variation on residual renal function in peritoneal dialysis patient. PLoS ONE 2016, 11, e0153115. [Google Scholar]


{kind=link}
| Characteristic | Value | Characteristic | Value |
|---|---|---|---|
| Age (years) | 61.1 ± 12.8 | Alb (g/dL) | 3.3 ± 0.3 |
| Duration of PD (months) | 13 (11–24) | Corrected Ca (mg/dL) | 9.2 ± 0.6 |
| Male: Female | 21:15 | P (mg/dL) | 5.2 (4.4–5.6) |
| BMI (kg/m2) | 22.6 (20.3–25.3) | Intact-PTH (pg/mL) | 167.8 (90.1–255.3) |
| MAP (mmHg) | 92.9 ± 16.2 | Total-cholesterol (mg/dL) | 189.7 ± 34.2 |
| History of peritonitis (%) | 13.9% | HbA1c (%) | 5.4 (5.1–5.7) |
| Primary disease of ESRD | CRP (mg/dL) | 0.06 (0.03–0.21) | |
| Chronic glomerulonephritis (%) | 25.0 | Urinary volume (mL/day) | 1500 (1140–1700) |
| Diabetic kidney disease (%) | 13.9 | Effluent volume (mL/day) | 248.0 ± 368.6 |
| Nephrosclerosis (%) | 33.3 | Residual GFR (mL/min) | 4.17 (2.60–6.51) |
| Other (%) | 27.8 | Peritoneal Kt/V | 1.03 ± 0.37 |
| Comorbidity | Renal Kt/V | 0.84 (0.64–1.40) | |
| Diabetes mellitus (%) | 25.0 | Total Kt/V | 1.95 (1.63–2.48) |
| Charlson Comorbidity Index | 3 (2–3) | 4 h-D/P cr | 0.61 (0.56–0.68) |
| ACE-I/ARB (%) | 66.7 | nPCR | 0.88 ± 0.18 |
| CCB (%) | 63.9 | Urinary protein (g/day) | 0.50 (0.27–0.76) |
| Diuretic (%) | 83.3 | Urinary DKK-3 (μg/day) | 13.4 (4.1–28.2) |
| Statin (%) | 27.8 | Renal Kt/V decline rate (/year) | 0.29 (0.05–0.48) |
| CAPD: APD | 24: 12 | Duration of follow-up (month) | 11.5 (11.0–12.0) |
| Hb (g/dL) | 11.6 ± 1.4 |
| Pearson’s Correlation Analyses | Multiple Regression Analyses | |||||
|---|---|---|---|---|---|---|
| r | p-Value | B | 95% CI | β | p-Value | |
| MAP (mmHg) | 0.05 | 0.77 | - | |||
| Alb (g/dL) | 0.23 | 0.18 | - | |||
| Total-cholesterol (mg/dL) | −0.05 | 0.78 | - | |||
| Renal Kt/V | 0.55 | 0.0005 | 0.259 | 0.080–0.437 | 0.38 | 0.0059 |
| Total Kt/V | 0.32 | 0.06 | - | |||
| 4 h-D/P cr | −0.19 | 0.27 | - | |||
| Urinary protein (g/day) | 0.28 | 0.1 | 0.164 | −0.011–0.338 | 0.23 | 0.0652 |
| Urinary DKK-3 (μg/day) | 0.61 | <0.0001 | 0.005 | 0.002–0.008 | 0.44 | 0.0015 |
| Diabetes mellitus | - | |||||
| ACE-I/ARB | - | |||||
| Diuretics | - | |||||
| History of peritonitis | - | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torigoe, K.; Muta, K.; Tsuji, K.; Yamashita, A.; Torigoe, M.; Abe, S.; Ota, Y.; Mukae, H.; Nishino, T. Association of Urinary Dickkopf-3 with Residual Renal Function Decline in Patients Undergoing Peritoneal Dialysis. Medicina 2021, 57, 631. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060631
Torigoe K, Muta K, Tsuji K, Yamashita A, Torigoe M, Abe S, Ota Y, Mukae H, Nishino T. Association of Urinary Dickkopf-3 with Residual Renal Function Decline in Patients Undergoing Peritoneal Dialysis. Medicina. 2021; 57(6):631. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060631
Chicago/Turabian StyleTorigoe, Kenta, Kumiko Muta, Kiyokazu Tsuji, Ayuko Yamashita, Miki Torigoe, Shinichi Abe, Yuki Ota, Hiroshi Mukae, and Tomoya Nishino. 2021. "Association of Urinary Dickkopf-3 with Residual Renal Function Decline in Patients Undergoing Peritoneal Dialysis" Medicina 57, no. 6: 631. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060631