
Evaluation of Mortality and Morbidity According to Initial Symptoms in COVID-19 Patients Using Clinical Epidemiologic Data from the Korea Centers for Disease Control & Prevention


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
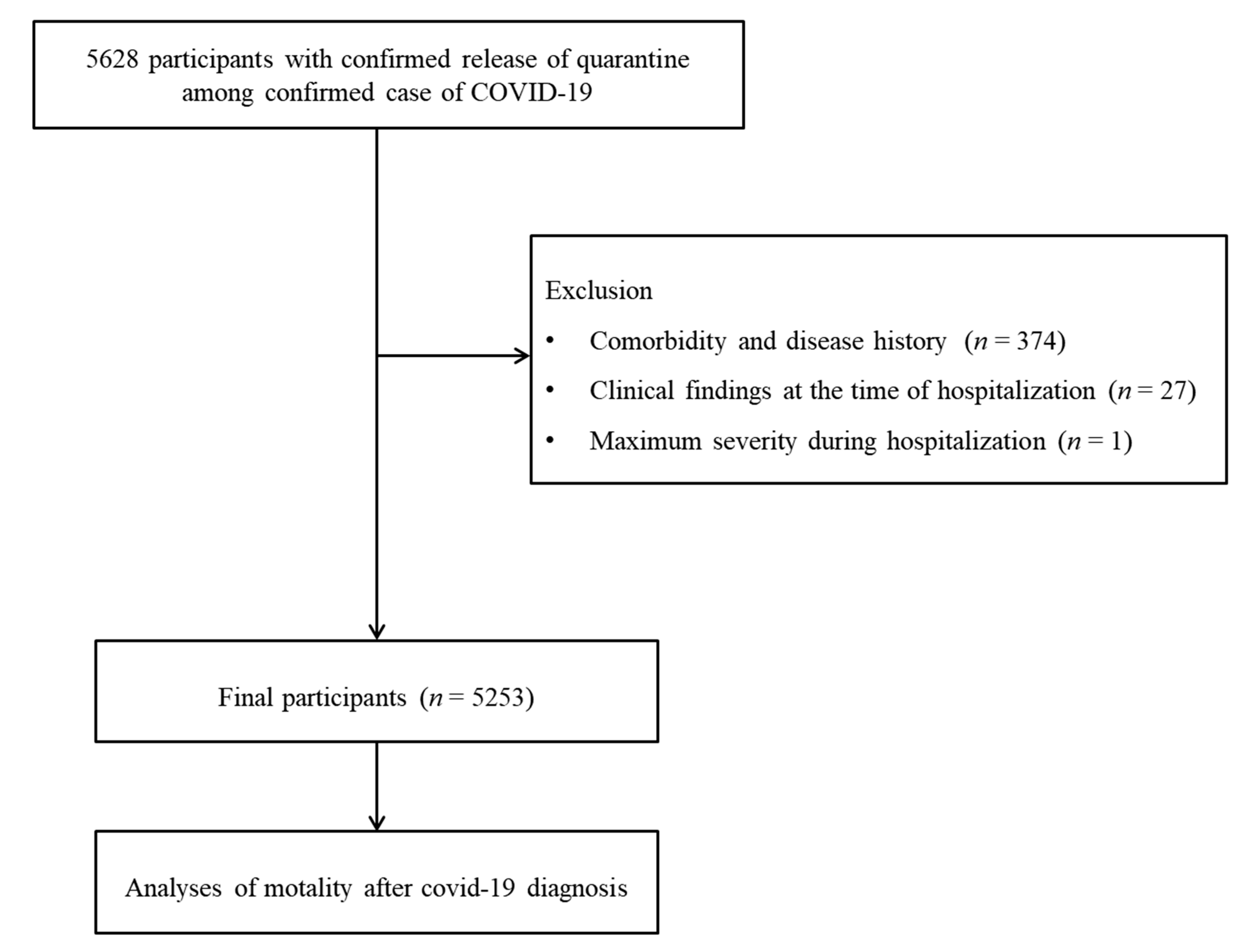
2.2. Study Population and Participant Selection
2.3. Exposure (Clinical Symptoms)
2.4. Outcome (Mortality)
2.5. Outcome (Morbidity)
2.6. Covariates
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Tan, W. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 12 December 2020).
- Chen, G.; Wu, D.I.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Ning, Q. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Lau, E.H.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Leung, G.M. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- To, K.K.W.; Tsang, O.T.Y.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yuen, K.Y. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Wendtner, C. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biguenet, A.; Bouiller, K.; Marty-Quinternet, S.; Brunel, A.S.; Chirouze, C.; Lepiller, Q. SARS-CoV-2 respiratory viral loads and association with clinical and biological features. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Liang, T. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: Retrospective cohort study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [Green Version]
- Fu, F.; Lou, J.; Xi, D.; Bai, Y.; Ma, G.; Zhao, B.; Wang, M. The Clinical Manifestations and Chest Computed Tomography Findings of Coronavirus Disease 2019 (COVID-19) Patients in China: A Proportion Meta-Analysis. Clin. Exp. Otorhinolaryngol. 2020, 13, 95–105. [Google Scholar] [CrossRef]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Wu, J. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Kang, M.K.; Kim, K.O.; Kim, M.C.; Cho, J.H.; Kim, S.B.; Park, J.G.; Kim, T.N. Clinical characteristics of coronavirus disease 2019 patients with diarrhea in Daegu. Korean J. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Koutsoukou, A. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe. 2020, 27, 992–1000.e3. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.I.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ning, Q. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Johnson, K.D.; Harris, C.; Cain, J.K.; Hummer, C.; Goyal, H.; Perisetti, A. Pulmonary and Extra-Pulmonary Clinical Manifestations of COVID-19. Front. Med. 2020, 7, 526. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, D.W. Does the Clinical Spectrum of Coronavirus Disease 2019 (COVID-19) Show Regional Differences? Clin. Exp. Otorhinolaryngol. 2020, 13, 83–84. [Google Scholar] [CrossRef]
- Yeo, C.; Kaushal, S.; Yeo, D. Enteric involvement of coronaviruses: Is faecal-oral transmission of SARS-CoV-2 possible? Lancet Gastroenterol. Hepatol. 2020, 5, 335–337. [Google Scholar] [CrossRef] [Green Version]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Tu, L. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef]
- Leung, W.K.; To, K.F.; Chan, P.K.; Chan, H.L.; Wu, A.K.; Lee, N.; Sung, J.J. Enteric involvement of severe acute respiratory syndrome-associated coronavirus infection. Gastroenterology 2003, 125, 1011–1017. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Lian, J.S.; Hu, J.H.; Gao, J.; Zheng, L.; Zhang, Y.M.; Yang, Y. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | The Participants with COVID-19 | ||
|---|---|---|---|
| Severe | Mild | p-Value | |
| Total participants (n, %) | 808 (100.0) | 4445 (100.0) | |
| Age (years old) (n, %) | <0.001 * | ||
| 0–9 | 0 (0.0) | 66 (1.5) | |
| 10–19 | 2 (0.3) | 192 (4.3) | |
| 20–29 | 21 (2.6) | 976 (22.0) | |
| 30–39 | 16 (2.0) | 503 (11.3) | |
| 40–49 | 36 (4.5) | 643 (14.5) | |
| 50–59 | 136 (16.8) | 932 (21.0) | |
| 60–69 | 191 (23.6) | 675 (15.2) | |
| 70–79 | 214 (26.5) | 327 (7.4) | |
| 80+ | 192 (23.8) | 131 (3.0) | |
| Sex (n, %) | <0.001 * | ||
| Male | 380 (47.0) | 1796 (40.4) | |
| Female | 428 (53.0) | 2649 (59.6) | |
| Obesity ‡ (n, %) | 0.066 | ||
| Underweight | 34 (4.2) | 213 (4.8) | |
| Normal | 430 (53.2) | 2465 (55.5) | |
| Overweight | 137 (17.0) | 815 (18.3) | |
| Obese I | 178 (22.0) | 787 (17.7) | |
| Obese II | 29 (3.6) | 165 (3.7) | |
| Systolic blood pressure (n, %) | <0.001 * | ||
| <120 mmHg | 166 (20.5) | 1077 (24.2) | |
| 120–129 mmHg | 167 (20.7) | 1042 (23.4) | |
| 130–139 mmHg | 141 (17.5) | 871 (19.6) | |
| 140–159 mmHg | 223 (27.6) | 1080 (24.3) | |
| ≥160 mmHg | 111 (13.7) | 375 (8.4) | |
| Diastolic blood pressure (n, %) | 0.024 * | ||
| <80 mmHg | 338 (41.8) | 1615 (36.3) | |
| 80–89 mmHg | 253 (31.3) | 1577 (35.5) | |
| 90–99 mmHg | 146 (18.1) | 850 (19.1) | |
| ≥100 mmHg | 71 (8.8) | 403 (9.1) | |
| Heart rate (mean, SD) | 87.28 (17.1) | 85.29 (14.5) | 0.002 † |
| Temperature (mean, SD) | 36.91 (0.5) | 36.87 (0.5) | 0.564 |
| Past medical history | |||
| Diabetes mellitus (n, %) | 229 (28.3) | 447 (10.1) | <0.001 * |
| Hypertension (n, %) | 382 (47.3) | 783 (17.6) | <0.001 * |
| Heart failure (n, %) | 35 (4.3) | 24 (0.5) | <0.001 * |
| Chronic heart disease (n, %) | 68 (8.4) | 109 (2.5) | <0.001 * |
| Asthma (n, %) | 30 (3.7) | 94 (2.1) | 0.006 * |
| COPD (n, %) | 20 (2.5) | 20 (0.5) | <0.001 * |
| Chronic kidney disease (n, %) | 32 (4.0) | 22 (0.5) | <0.001 * |
| Any cancer (n, %) | 44 (5.5) | 101 (2.3) | <0.001 * |
| Chronic liver disease (n, %) | 22 (2.7) | 59 (1.3) | 0.003 * |
| Rheumatic or autoimmune disease (n, %) | 9 (1.1) | 29 (0.7) | 0.155 |
| Dementia (n, %) | 215 (4.2) | 8 (6.5) | 0.218 |
| Clinical initial symptoms | |||
| Respiratory symptoms | |||
| Cough (n, %) | 383 (47.4) | 1812 (40.8) | <0.001 * |
| Sputum (n, %) | 283 (35.0) | 1222 (27.5) | <0.001 * |
| Sore throat (n, %) | 78 (9.7) | 723 (16.3) | <0.001 * |
| Rhinorrhea (n, %) | 50 (6.2) | 483 (10.9) | <0.001 * |
| Shortness of breath (n, %) | 325 (40.2) | 302 (6.8) | <0.001 * |
| Gastrointestinal symptoms | |||
| Vomiting and nausea (n, %) | 62 (7.7) | 178 (4.0) | <0.001 * |
| Diarrhea (n, %) | 87 (10.8) | 375 (8.4) | 0.031 * |
| General symptoms | |||
| Fever (n, %) | 336 (41.6) | 906 (20.4) | <0.001 * |
| Myalgia (n, %) | 141 (17.5) | 718 (16.2) | 0.359 |
| Fatigue and malaise (n, %) | 59 (7.3) | 170 (3.8) | <0.001 * |
| Neurologic symptoms | |||
| Headache (n, %) | 110 (13.6) | 767 (17.3) | 0.011 * |
| Alteration of confusion (n, %) | 27 (3.3) | 8 (0.2) | <0.001 * |
| Death (n, %) | 241 (29.8) | 0 (0.0) | <0.001 * |
| Characteristics | HRs for Death | |||
|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | |
| Symptom | ||||
| Cough | 0.66 (0.50–0.86) | 0.002 * | 0.90 (0.67–1.20) | 0.466 |
| Sputum | 1.02 (0.77–1.34) | 0.904 | 1.19 (0.88–1.60) | 0.256 |
| Sore throat | 0.31 (0.18–0.55) | <0.001 * | 0.81 (0.46–1.43) | 0.466 |
| Rhinorrhea | 0.22 (0.10–0.50) | <0.001 * | 0.41 (0.18–0.92) | 0.036 * |
| Shortness of breath | 6.39 (4.96–8.25) | <0.001 * | 3.33 (2.52–4.40) | <0.001 * |
| Vomiting and nausea | 1.35 (0.81–2.24) | 0.252 | 1.01 (0.60–1.69) | 0.977 |
| Diarrhea | 0.79 (0.49–1.28) | 0.342 | 0.94 (0.57–1.54) | 0.803 |
| Fever | 1.97 (1.52–2.55) | <0.001 * | 1.50 (1.05–2.15) | 0.024 * |
| Myalgia | 0.46 (0.29–0.72) | <0.001 * | 0.74 (0.47–1.18) | 0.210 |
| Fatigue and malaise | 1.63 (0.99–2.66) | 0.054 | 1.04 (0.61–1.75) | 0.895 |
| Headache | 0.28 (0.16–0.48) | <0.001 * | 0.54 (0.31–0.96) | 0.036 * |
| Alteration of confusion | 20.75 (13.46–31.98) | <0.001 * | 3.89 (2.40–6.31) | <0.001 * |
| Symptom score | ||||
| Respiratory symptom | 1.06 (0.95–1.18) | 0.320 | 1.18 (1.05–1.33) | 0.004 * |
| Gastrointestinal symptom | 0.99 (0.71–1.38) | 0.947 | 0.97 (0.69–1.37) | 0.878 |
| General symptom | 1.19 (1.00–1.43) | 0.049 * | 1.09 (0.87–1.38) | 0.442 |
| Neurologic symptom | 0.82 (0.58–1.17) | 0.275 | 1.26 (0.88–1.80) | 0.217 |
| Full insertion model ‡ | ||||
| Respiratory symptom | 1.05 (0.94–1.18) | 0.393 | 1.17 (1.04–1.32) | 0.008 * |
| Gastrointestinal symptom | 0.96 (0.69–1.35) | 0.830 | 0.92 (0.65–1.31) | 0.652 |
| General symptom | 1.22 (1.01–1.46) | 0.039 * | 1.02 (0.80–1.29) | 0.884 |
| Neurologic symptom | 0.75 (0.52–1.08) | 0.121 | 1.18 (0.81–1.71) | 0.388 |
| Characteristics | Ors For Severe Morbidity | |||
|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | |
| Symptom | ||||
| Cough | 1.31 (1.13–1.52) | <0.001 * | 1.56 (1.30–1.87) | <0.001 * |
| Sputum | 1.42 (1.21–1.67) | <0.001 * | 1.52 (1.26–1.84) | <0.001 * |
| Sore throat | 0.55 (0.43–0.70) | <0.001 * | 0.87 (0.66–1.15) | 0.341 |
| Rhinorrhea | 0.54 (0.40–0.73) | <0.001 * | 0.77 (0.54–1.08) | 0.131 |
| Shortness of breath | 9.23 (7.69–11.08) | <0.001 * | 7.17 (5.75–8.95) | <0.001 * |
| Vomiting and nausea | 1.99 (1.48–2.69) | <0.001 * | 1.56 (1.09–2.22) | 0.015 * |
| Diarrhea | 1.31 (1.02–1.68) | 0.032 * | 1.41 (1.06–1.89) | 0.020 * |
| Fever | 2.78 (2.38–3.26) | <0.001 * | 2.38 (1.87–3.05) | <0.001 * |
| Myalgia | 1.10 (0.90–1.34) | 0.359 | 1.21 (0.96–1.52) | 0.109 |
| Fatigue and malaise | 1.98 (1.46–2.69) | <0.001 * | 1.45 (0.99–2.12) | 0.056 |
| Headache | 0.76 (0.61–0.94) | 0.011 * | 1.00 (0.78–1.28) | 0.997 |
| Alteration of confusion | 19.17 (8.68–42.36) | <0.001 * | 8.02 (3.13–20.53) | <0.001 * |
| Symptom score | ||||
| Respiratory symptom | 1.32 (1.24–1.41) | <0.001 * | 1.45 (1.34–1.57) | <0.001 * |
| Gastrointestinal symptom | 1.46 (1.22–1.75) | <0.001 * | 1.40 (1.13–1.72) | 0.002 * |
| General symptom | 1.71 (1.54–1.90) | <0.001 * | 1.53 (1.32–1.76) | <0.001 * |
| Neurologic symptom | 0.97 (0.79–1.18) | 0.744 | 1.18 (0.94–1.48) | 0.165 |
| Full insertion model ‡ | ||||
| Respiratory symptom | 1.26 (1.18–1.35) | <0.001 * | 1.41 (1.30–1.53) | <0.001 * |
| Gastrointestinal symptom | 1.26 (1.04–1.52) | 0.017 * | 1.22 (0.98–1.52) | 0.069 |
| General symptom | 1.62 (1.45–1.80) | <0.001 * | 1.37 (1.18–1.59) | <0.001 * |
| Neurologic symptom | 0.69 (0.56–0.85) | 0.001 * | 0.87 (0.68–1.11) | 0.274 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Yoo, D.M.; Min, C.; Kim, J.-H.; Choi, H.G. Evaluation of Mortality and Morbidity According to Initial Symptoms in COVID-19 Patients Using Clinical Epidemiologic Data from the Korea Centers for Disease Control & Prevention. Medicina 2021, 57, 688. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070688
Kim SY, Yoo DM, Min C, Kim J-H, Choi HG. Evaluation of Mortality and Morbidity According to Initial Symptoms in COVID-19 Patients Using Clinical Epidemiologic Data from the Korea Centers for Disease Control & Prevention. Medicina. 2021; 57(7):688. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070688
Chicago/Turabian StyleKim, So Young, Dae Myoung Yoo, Chanyang Min, Joo-Hee Kim, and Hyo Geun Choi. 2021. "Evaluation of Mortality and Morbidity According to Initial Symptoms in COVID-19 Patients Using Clinical Epidemiologic Data from the Korea Centers for Disease Control & Prevention" Medicina 57, no. 7: 688. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070688