
Advancements in Transcatheter Aortic Valve Implantation: A Focused Update

 , ,
, ,
Abstract
:1. Introduction. Extended Indications: A Powerful Stimulus to Reduce All Complications
2. Novelties in Femoral Approach: From US Guided Micro-Puncture to Iliac Intravascular Lithotripsy
3. Cerebral Protection Devices for Stroke Prevention
3.1. SENTINEL™ Cerebral Protection System
3.2. Embol-X
3.3. TriGuard™ Device
3.4. Wirion Embolic Protection System
3.5. Embrella Embolic Deflector Device
3.6. Novel Perspectives for Cerebral Protection during TAVI
4. Optimal Valve Positioning to Reduce Pace-Maker Implantation
4.1. Conduction Disturbances
4.1.1. Mechanism
4.1.2. Incidence
New-Onset Persistent Left Bundle Branch Block (NOP-LBBB)
Permanent Pacemaker Implantation
4.1.3. Predictors of Conduction Disturbances
LBBB after TAVI
PPM Implantation after TAVI
4.1.4. Implantation Techniques: Measures to Reduce the Risk of Pacemaker Implantation
4.2. Aortic Regurgitation Post TAVI
4.2.1. Definition
4.2.2. Mechanism
4.2.3. Predictors of Post-Procedural Paravalvular Aortic Regurgitation
Annulus Dimensions and Shape
Valvular and LVOT Calcium
Valve Type
Sizing
4.2.4. Implantation Techniques
Measures to Reduce Aortic Regurgitation
5. Valve-in-Valve and Valve-in-TAVI
5.1. Outcomes of VIV TAVI
5.2. Comparison of VIV versus Re-Do SAVR
5.3. Procedural Considerations for VIV-TAVI
5.4. Limitations and New Techniques
5.5. Coronary Occlusion
5.6. THV Malpositioning
5.7. Patient-Prosthesis Mismatch
5.8. Leaflet Thickening and Thrombosis
5.9. Reintervention after TAVI: TAVI in TAVI
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Otto, C.M. Informed Shared Decisions for Patients with Aortic Stenosis. N. Engl. J. Med. 2019, 380, 1769–1770. [Google Scholar] [CrossRef]
- Siontis, G.C.; Overtchouk, P.; Cahill, T.J.; Modine, T.; Prendergast, B.; Praz, F.; Pilgrim, T.; Petrinic, T.; Nikolakopoulou, A.; Salanti, G.; et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: An updated meta-analysis. Eur. Heart J. 2019, 40, 3143–3153. [Google Scholar] [CrossRef]
- Carroll, J.D.; Mack, M.J.; Vemulapalli, S.; Herrmann, H.C.; Gleason, T.G.; Hanzel, G.; Deeb, G.M.; Thourani, V.H.; Cohen, D.J.; Desai, N.; et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2492–2516. [Google Scholar] [CrossRef]
- El Faquir, N.; De Backer, O.; Bosmans, J.; Rudolph, T.; Buzzatti, N.; Bieliauskas, G.; Collas, V.; Wienemann, H.; Schiavi, D.; Cummins, P.; et al. Patient-Specific Computer Simulation in TAVR with the Self-Expanding Evolut R Valve. Cardiovasc. Interv. 2020, 13, 1803–1812. [Google Scholar]
- Jhand, A.; Apala, D.R.; Dhawan, R.; Katta, N.; Aronow, H.D.; Daniels, M.J.; Porter, T.R.; Altin, E.; Goldsweig, A.M. Meta-analysis Comparing Transradial versus Transfemoral Secondary Access in Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2020, 131, 74–81. [Google Scholar] [CrossRef]
- Leclercq, F.; Robert, P.; Akodad, M.; Macia, J.C.; Gandet, T.; Delseny, D.; Chettouh, M.; Schmutz, L.; Robert, G.; Levy, G.; et al. Prior Balloon Valvuloplasty versus Direct Transcatheter Aortic Valve Replacement: Results from the DIRECTAVI Trial. Cardiovasc. Interv. 2020, 13, 594–602. [Google Scholar]
- Thiele, H.; Kurz, T.; Feistritzer, H.J.; Stachel, G.; Hartung, P.; Lurz, P.; Eitel, I.; Marquetand, C.; Nef, H.; Doerr, O.; et al. General Versus Local Anesthesia with Conscious Sedation in Transcatheter Aortic Valve Implantation: The Randomized SOLVE-TAVI Trial. Circulation 2020, 142, 1437–1447. [Google Scholar] [CrossRef]
- Di Mario, C.; Goodwin, M.; Ristalli, F.; Ravani, M.; Meucci, F.; Stolcova, M.; Sardella, G.; Salvi, N.; Bedogni, F.; Berti, S.; et al. A Prospective Registry of Intravascular Lithotripsy-Enabled Vascular Access for Transfemoral Transcatheter Aortic Valve Replacement. Cardiovasc. Interv. 2019, 12, 502–504. [Google Scholar] [CrossRef]
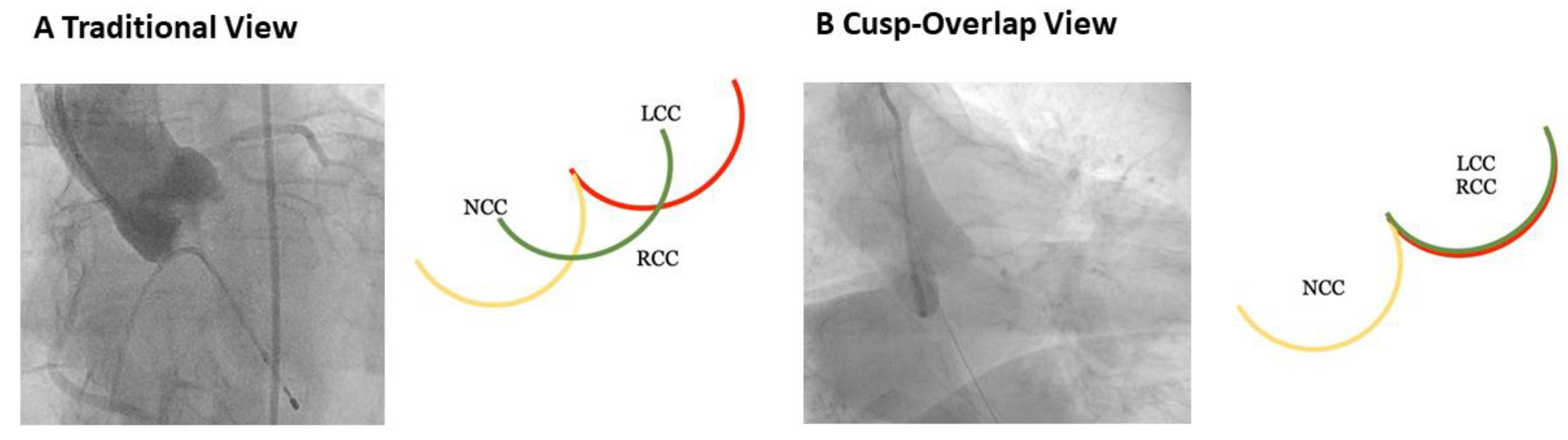
- Tang, G.H.; Zaid, S.; Michev, I.; Ahmad, H.; Kaple, R.; Undemir, C.; Cohen, M.; Lansman, S.L. “Cusp-Overlap” View Simplifies Fluoroscopy-Guided Implantation of Self-Expanding Valve in Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2018, 11, 1663–1665. [Google Scholar] [CrossRef]
- Lilly, S.M.; Deshmukh, A.J.; Epstein, A.E.; Ricciardi, M.J.; Shreenivas, S.; Velagapudi, P.; Wyman, J.F. 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 76, 2391–2411. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Munoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 52, 616–664. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: Executive summary a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J. Am. Coll. Cardiol. 2021, 77, 450–500. [Google Scholar] [CrossRef]
- Velagapudi, P.; Bapat, V.; Kodali, S. When Excluded from Randomized Clinical Trials: To “OR” or “‘TAVR”? J. Am. Coll. Cardiol. 2021, 77, 124–127. [Google Scholar] [CrossRef]
- Cribier, A.; Eltchaninoff, H.; Bash, A.; Borenstein, N.; Tron, C.; Bauer, F.; Derumeaux, G.; Anselme, F.; Laborde, F.; Leon, M.B. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation 2002, 106, 3006–3008. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Romano, M.; Lefèvre, T.; Hovasse, T.; Farge, A.; Le Houerou, D.; Hayashida, K.; Watanabe, Y.; Garot, P.; Benamer, H.; et al. Direct Comparison of Feasibility and Safety of Transfemoral versus Transaortic versus Transapical Transcatheter Aortic Valve Replacement. Cardiovasc. Interv. 2016, 9, 2320–2325. [Google Scholar] [CrossRef]
- Ando, T.; Akintoye, E.; Telila, T.; Briasoulis, A.; Takagi, H.; Grines, C.L.; Afonso, L. Trends in Vascular Complications in High-Risk Patients Following Transcatheter Aortic Valve Replacement in the United States. Am. J. Cardiol. 2017, 119, 1433–1437. [Google Scholar] [CrossRef]
- Toggweiler, S.; Leipsic, J.; Binder, R.K.; Freeman, M.; Barbanti, M.; Heijmen, R.H.; Wood, D.A.; Webb, J.G. Management of vascular access in transcatheter aortic valve replacement: Part 1: Basic anatomy, imaging, sheaths, wires, and access routes. JACC Cardiovasc. Interv. 2013, 6, 643–653. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the bleeding academic research consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, G.J.; Reeves, B.C.; Rogers, C.A.; Rizvi, S.I.; Culliford, L.; Angelini, G.D. Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery. Circulation 2007, 116, 2544–2552. [Google Scholar] [CrossRef] [Green Version]
- Piccolo, R.; Pilgrim, T.; Franzone, A.; Valgimigli, M.; Haynes, A.; Asami, M.; Lanz, J.; Räber, L.; Praz, F.; Langhammer, B.; et al. Frequency, Timing, and Impact of Access-Site and Non–Access-Site Bleeding on Mortality among Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2017, 10, 1436–1446. [Google Scholar] [CrossRef]
- Tchetche, D.; Van der Boon, R.M.; Dumonteil, N.; Chieffo, A.; Van Mieghem, N.M.; Farah, B.; Buchanan, G.L.; Saady, R.; Marcheix, B.; Serruys, P.W.; et al. Adverse impact of bleeding and transfusion on the outcome post-transcatheter aortic valve implantation: Insights from the Pooled-RotterdAm-Milano-Toulouse in Collaboration Plus (PRAGMATIC Plus) initiative. Am. Heart J. 2012, 164, 402–409. [Google Scholar] [CrossRef]
- Vincent, F.; Spillemaeker, H.; Kyheng, M.; Belin-Vincent, C.; Delhaye, C.; Piérache, A.; Denimal, T.; Verdier, B.; Debry, N.; Moussa, M.; et al. Ultrasound guidance to reduce vascular and bleeding complications of percutaneous transfemoral transcatheter aortic valve replacement: A propensity score–matched comparison. J. Am. Heart Assoc. 2020, 9, e014916. [Google Scholar] [CrossRef]
- Ben-Dor, I.; Sharma, A.; Rogers, T.; Yerasi, C.; Case, B.C.; Chezar-Azerrad, C.; Musallam, A.; Forrestal, B.J.; Zhang, C.; Hashim, H.; et al. Micropuncture technique for femoral access is associated with lower vascular complications compared to standard needle. Catheter. Cardiovasc. Interv. 2020, 97, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, J.A.; Lardizabal, J.; Mouanoutoua, M.; Buhari, C.F.; Berg, R.; Joshi, B.; El-Sherief, K.; Wessel, R.; Singh, M.; Kiel, R. Femoral micropuncture or routine introducer study (FEMORIS). Cardiology 2014, 129, 39–43. [Google Scholar] [CrossRef]
- Elbaz-Greener, G.; Zivkovic, N.; Arbel, Y.; Radhakrishnan, S.; Fremes, S.E.; Wijeysundera, H.C. Use of Two-Dimensional Ultrasonographically Guided Access to Reduce Access-Related Complications for Transcatheter Aortic Valve Replacement. Can. J. Cardiol. 2017, 33, 918–924. [Google Scholar] [CrossRef]
- Koshy, L.M.; Aberle, L.H.; Krucoff, M.W.; Hess, C.N.; Mazzaferri, E.; Jolly, S.S.; Jacobs, A.; Gibson, C.M.; Mehran, R.; Gilchrist, I.C.; et al. Comparison of Radial Access, Guided Femoral Access, and Non-Guided Femoral Access among Women Undergoing Percutaneous Coronary Intervention. J. Invasive Cardiol. 2018, 30, 18–22. [Google Scholar]
- Seto, A.H.; Abu-Fadel, M.S.; Sparling, J.M.; Zacharias, S.J.; Daly, T.S.; Harrison, A.T.; Suh, W.M.; Vera, J.A.; Aston, C.E.; Winters, R.J.; et al. Real-time ultrasound guidance facilitates femoral arterial access and reduces vascular complications: FAUST (Femoral Arterial Access with Ultrasound Trial). JACC Cardiovasc. Interv. 2010, 3, 751–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soverow, J.; Oyama, J.; Lee, M.S. Adoption of routine ultrasound guidance for femoral arterial access for cardiac catheterization. J. Invasive Cardiol. 2016, 28, 311–314. [Google Scholar]
- Kurra, V.; Schoenhagen, P.; Roselli, E.E.; Kapadia, S.R.; Tuzcu, E.M.; Greenberg, R.; Akhtar, M.; Desai, M.Y.; Flamm, S.D.; Halliburton, S.S.; et al. Prevalence of significant peripheral artery disease in patients evaluated for percutaneous aortic valve insertion: Preprocedural assessment with multidetector computed tomography. J. Thorac. Cardiovasc. Surg. 2009, 137, 1258–1264. [Google Scholar] [CrossRef] [Green Version]
- Kussmaul, W.G.; Buchbinder, M.; Whitlow, P.L.; Aker, U.T.; Heuser, R.R.; King, S.B.; Kent, K.M.; Leon, M.B.; Kolansky, D.M.; Sandza, J.G. Rapid arterial hemostasis and decreased access site complications after cardiac catheterization and angioplasty: Results of a randomized trial of a novel hemostatic device. J. Am. Coll. Cardiol. 1995, 25, 1685–1692. [Google Scholar] [CrossRef] [Green Version]
- Ramlawi, B.; Anaya-Ayala, J.E.; Reardon, M.J. Transcatheter aortic valve replacement (TAVR): Access planning and strategies. Methodist DeBakey Cardiovasc. J. 2012, 8, 22–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAteer, J.A.; Bailey, M.R.; Williams, J.C.; Cleveland, R.O.; Evan, A.P. Strategies for improved shock wave lithotripsy. Minerva Urol. Nefrol. 2005, 57, 271–287. [Google Scholar] [PubMed]
- Davros, W.J.; Garra, B.S.; Zeman, R.K. Gallstone lithotripsy: Relevant physical principles and technical issues. Radiology 1991, 178, 397–408. [Google Scholar] [CrossRef]
- Brinton, T.J.; Ali, Z.A.; Hill, J.M.; Meredith, I.T.; Maehara, A.; Illindala, U.; Lansky, A.; Götberg, M.; Van Mieghem, N.M.; Whitbourn, R.; et al. Feasibility of shockwave coronary intravascular lithotripsy for the treatment of calcified coronary stenoses first description. Circulation 2019, 139, 834–836. [Google Scholar] [CrossRef]
- Ali, Z.A.; Nef, H.; Escaned, J.; Werner, N.; Banning, A.P.; Hill, J.M.; De Bruyne, B.; Montorfano, M.; Lefevre, T.; Stone, G.W.; et al. Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Stenoses: The Disrupt CAD II Study. Circ. Cardiovasc. Interv. 2019, 12, e008434. [Google Scholar] [CrossRef]
- Hill, J.M.; Kereiakes, D.J.; Shlofmitz, R.A.; Klein, A.J.; Riley, R.F.; Price, M.J.; Herrmann, H.C.; Bachinsky, W.; Waksman, R.; Stone, G.W. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 2635–2646. [Google Scholar] [CrossRef]
- Adams, G.; Shammas, N.; Mangalmurti, S.; Bernardo, N.L.; Miller, W.E.; Soukas, P.A.; Parikh, S.A.; Armstrong, E.J.; Tepe, G.; Lansky, A.; et al. Intravascular Lithotripsy for Treatment of Calcified Lower Extremity Arterial Stenosis: Initial Analysis of the Disrupt PAD III Study. J. Endovasc. Ther. 2020, 27, 473–480. [Google Scholar] [CrossRef]
- Ristalli, F.; Dini, C.S.; Stolcova, M.; Nardi, G.; Valente, S.; Meucci, F.; Di Mario, C. Role of Lithotripsy for Small Calcified Iliacs in the Era of Big Devices. Curr. Cardiol. Rep. 2019, 21, 143. [Google Scholar] [CrossRef]
- Ali, Z.A.; Brinton, T.J.; Hill, J.M.; Maehara, A.; Matsumura, M.; Karimi Galougahi, K.; Illindala, U.; Götberg, M.; Whitbourn, R.; Van Mieghem, N.; et al. Optical Coherence Tomography Characterization of Coronary Lithoplasty for Treatment of Calcified Lesions: First Description. JACC Cardiovasc. Imaging 2017, 10, 897–906. [Google Scholar] [CrossRef]
- Di Mario, C.; Chiriatti, N.; Stolcova, M.; Meucci, F.; Squillantini, G. Lithotripsy-assisted transfemoral aortic valve implantation. Eur. Heart J. 2018, 39, 2655. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, S.; Agarwal, S.; Miller, D.C.; Webb, J.G.; Mack, M.; Ellis, S.; Herrmann, H.C.; Pichard, A.D.; Tuzcu, E.M.; Svensson, L.G.; et al. Insights into Timing, Risk Factors, and Outcomes of Stroke and Transient Ischemic Attack after Transcatheter Aortic Valve Replacement in the PARTNER Trial (Placement of Aortic Transcatheter Valves). Circ. Cardiovasc. Interv. 2016, 9, e002981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nombela-Franco, L.; Webb, J.G.; de Jaegere, P.P.; Toggweiler, S.; Nuis, R.J.; Dager, A.E.; Amat-Santos, I.J.; Cheung, A.; Ye, J.; Binder, R.K.; et al. Timing, predictive factors, and prognostic value of cerebrovascular events in a large cohort of patients undergoing transcatheter aortic valve implantation. Circulation 2012, 126, 3041–3053. [Google Scholar] [CrossRef]
- Gasior, T.; Mangner, N.; Bijoch, J.; Wojakowski, W. Cerebral embolic protection systems for transcatheter aortic valve replacement. J. Interv. Cardiol. 2018, 31, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nombela-Franco, L.; Armijo, G.; Tirado-Conte, G. Cerebral embolic protection devices during transcatheter aortic valve implantation: Clinical versus silent embolism. J. Thorac. Dis. 2018, 10, S3604. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Nijenhuis, V.J.; Brouwer, J.; Delewi, R.; Hermanides, R.S.; Holvoet, W.; Dubois, C.L.; Frambach, P.; De Bruyne, B.; van Houwelingen, G.K.; Van Der Heyden, J.A.; et al. Anticoagulation with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N. Engl. J. Med. 2020, 382, 1696–1707. [Google Scholar] [CrossRef]
- Makkar, R.R.; Yoon, S.H.; Leon, M.B.; Chakravarty, T.; Rinaldi, M.; Shah, P.B.; Skipper, E.R.; Thourani, V.H.; Babaliaros, V.; Cheng, W.; et al. Association between transcatheter aortic valve replacement for bicuspid vs tricuspid aortic stenosis and mortality or stroke. J. Am. Med. Assoc. 2019, 321, 2193–2202. [Google Scholar] [CrossRef] [PubMed]
- Kahlert, P.; Knipp, S.C.; Schlamann, M.; Thielmann, M.; Al-Rashid, F.; Weber, M.; Johansson, U.; Wendt, D.; Jakob, H.G.; Forsting, M.; et al. Silent and apparent cerebral ischemia after percutaneous transfemoral aortic valve implantation: A diffusion-weighted magnetic resonance imaging study. Circulation 2010, 121, 870–878. [Google Scholar] [CrossRef] [Green Version]
- Makkar, R.R.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Kapadia, S.; Webb, J.G.; Yoon, S.H.; Trento, A.; Svensson, L.G.; Herrmann, H.C.; et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 799–809. [Google Scholar] [CrossRef]
- Dahle, T.G.; Kaneko, T.; McCabe, J.M. Outcomes Following Subclavian and Axillary Artery Access for Transcatheter Aortic Valve Replacement: Society of the Thoracic Surgeons/American College of Cardiology TVT Registry Report. JACC Cardiovasc. Interv. 2019, 12, 662–669. [Google Scholar] [CrossRef]
- Thiele, H.; Kurz, T.; Feistritzer, H.J.; Stachel, G.; Hartung, P.; Eitel, I.; Marquetand, C.; Nef, H.; Doerr, O.; Lauten, A.; et al. Comparison of newer generation self-expandable vs. balloon-expandable valves in transcatheter aortic valve implantation: The randomized SOLVE-TAVI trial. Eur. Heart J. 2020, 41, 1890–1899. [Google Scholar] [CrossRef]
- Tay, E.L.; Gurvitch, R.; Wijesinghe, N.; Nielispach, F.; Wood, D.; Cheung, A.; Ye, J.; Lichtenstein, S.V.; Carere, R.; Thompson, C.; et al. A high-risk period for cerebrovascular events exists after transcatheter aortic valve implantation. JACC Cardiovasc. Interv. 2011, 4, 1290–1297. [Google Scholar] [CrossRef] [Green Version]
- Dangas, G.D.; Tijssen, J.G.; Wöhrle, J.; Søndergaard, L.; Gilard, M.; Möllmann, H.; Makkar, R.R.; Herrmann, H.C.; Giustino, G.; Baldus, S.; et al. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 120–129. [Google Scholar] [CrossRef]
- Demir, O.M.; Iannopollo, G.; Mangieri, A.; Ancona, M.B.; Regazzoli, D.; Mitomo, S.; Colombo, A.; Weisz, G.; Latib, A. The Role of Cerebral Embolic Protection Devices during Transcatheter Aortic Valve Replacement. Front. Cardiovasc. Med. 2018, 5, 150. [Google Scholar] [CrossRef] [Green Version]
- Van Gils, L.; Kroon, H.; Daemen, J.; Ren, C.; Maugenest, A.M.; Schipper, M.; De Jaegere, P.P.; Van Mieghem, N.M. Complete filter-based cerebral embolic protection with transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2018, 91, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Van Mieghem, N.M.; van Gils, L.; Ahmad, H.; Van Kesteren, F.; Van Der Werf, H.W.; Brueren, G.; Storm, M.; Lenzen, M.; Daemen, J.; van den Heuvel, A.F.; et al. Filter-based cerebral embolic protection with transcatheter aortic valve implantation: The randomised MISTRAL-C trial. EuroIntervention 2016, 12, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Haussig, S.; Mangner, N.; Dwyer, M.G.; Lehmkuhl, L.; Lücke, C.; Woitek, F.; Holzhey, D.M.; Mohr, F.W.; Gutberlet, M.; Zivadinov, R.; et al. Effect of a cerebral protection device on brain lesions following transcatheter aortic valve implantation in patients with severe aortic stenosis: The CLEAN-TAVI randomized clinical trial. J. Am. Med. Assoc. 2016, 316, 592–601. [Google Scholar] [CrossRef]
- Kapadia, S.R.; Kodali, S.; Makkar, R.; Mehran, R.; Lazar, R.M.; Zivadinov, R.; Dwyer, M.G.; Jilaihawi, H.; Virmani, R.; Anwaruddin, S.; et al. Protection against Cerebral Embolism during Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2017, 69, 367–377. [Google Scholar] [CrossRef]
- Wendt, D.; Kleinbongard, P.; Knipp, S.; Al-Rashid, F.; Gedik, N.; El Chilali, K.; Schweter, S.; Schlamann, M.; Kahlert, P.; Neuhäuser, M.; et al. Intraaortic Protection from Embolization in Patients Undergoing Transaortic Transcatheter Aortic Valve Implantation. Ann. Thorac. Surg. 2015, 100, 686–691. [Google Scholar] [CrossRef]
- Baumbach, A.; Mullen, M.; Brickman, A.M.; Aggarwal, S.K.; Pietras, C.G.; Forrest, J.K.; Hildick-Smith, D.; Meller, S.M.; Gambone, L.; den Heijer, P.; et al. Safety and performance of a novel embolic deflection device in patients undergoing transcatheter aortic valve replacement: Results from the DEFLECT I study. EuroIntervention 2015, 11, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Samim, M.; Hendrikse, J.; Agostoni, P.; Van Der Worp, B.; Budde, R.P.; Nijhoff, F.; Ramjankhan, F.; Doevendans, P.A.; Stella, P.R. CRT-809 TriGuardTM HD Embolic Deflection Device for Cerebral Protection during Transcatheter Aortic Valve Replacement: Results: Of the Deflect II Trial. JACC Cardiovasc. Interv. 2015, 8, S51. [Google Scholar] [CrossRef] [Green Version]
- Lansky, A.J.; Schofer, J.; Tchetche, D.; Stella, P.; Pietras, C.G.; Parise, H.; Abrams, K.; Forrest, J.K.; Cleman, M.; Reinöhl, J.; et al. A prospective randomized evaluation of the TriGuardTM HDH embolic DEFLECTion device during transcatheter aortic valve implantation: Results from the DEFLECT III trial. Eur. Heart J. 2015, 36, 2070–2078. [Google Scholar] [CrossRef] [PubMed]
- Scheinert, D.; Reimers, B.; Cremonesi, A.; Schmidt, A.; Sievert, H.; Rohde, S.; Schofer, J.; Mudra, H.G.; Bosiers, M.; Zeller, T.; et al. Independent Modular Filter for Embolic Protection in Carotid Stenting. Circ. Cardiovasc. Interv. 2017, 10, e004244. [Google Scholar] [CrossRef]
- Rodés-Cabau, J.; Kahlert, P.; Neumann, F.J.; Schymik, G.; Webb, J.G.; Amarenco, P.; Brott, T.; Garami, Z.; Gerosa, G.; Lefèvre, T.; et al. Feasibility and exploratory efficacy evaluation of the embrella embolic deflector system for the prevention of cerebral emboli in patients undergoing transcatheter aortic valve replacement: The PROTAVI-C pilot study. JACC Cardiovasc. Interv. 2014, 7, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Haussig, S.; Linke, A.; Mangner, N. Cerebral Protection Devices during Transcatheter Interventions: Indications, Benefits, and Limitations. Curr. Cardiol. Rep. 2020, 22, 96. [Google Scholar] [CrossRef] [PubMed]
- Latib, A.; Mangieri, A.; Vezzulli, P.; Spagnolo, P.; Sardanelli, F.; Fellegara, G.; Pagnesi, M.; Giannini, F.; Falini, A.; Gorla, R.; et al. First-in-Man Study Evaluating the Emblok Embolic Protection System during Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Pasupati, S. TCT CONNECT-458 Clinical Performance of a Total Embolic Protection Device: Results of the Emboliner SafePass 2 Study. J. Am. Coll. Cardiol. 2020, 76, B196. [Google Scholar] [CrossRef]
- Chen, S.; Chau, K.H.; Nazif, T.M. The incidence and impact of cardiac conduction disturbances after transcatheter aortic valve replacement. Ann. Cardiothorac. Surg. 2020, 9, 452–467. [Google Scholar] [CrossRef]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J., Jr.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef] [Green Version]
- Kaneko, H.; Hoelschermann, F.; Seifert, M.; Tambor, G.; Okamoto, M.; Moeller, V.; Neuss, M.; Butter, C. Predictors of permanent pacemaker implantation after transcatheter aortic valve implantation for aortic stenosis using Medtronic new generation self-expanding CoreValve Evolut, R. Heart Vessels 2019, 34, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.I.; Miura, M.; Tagliari, A.P.; Lee, Y.H.; Shirai, S.; Puri, R.; Maisano, F.; Taramasso, M. Intraventricular conduction disturbances after transcatheter aortic valve implantation. Interv. Cardiol. Rev. 2020, 15, e11. [Google Scholar] [CrossRef]
- Chamandi, C.; Barbanti, M.; Munoz-Garcia, A.; Latib, A.; Nombela-Franco, L.; Gutiérrez-Ibanez, E.; Veiga-Fernandez, G.; Cheema, A.N.; Cruz-Gonzalez, I.; Serra, V.; et al. Long-Term Outcomes in Patients with New-Onset Persistent Left Bundle Branch Block Following TAVR. JACC Cardiovasc. Interv. 2019, 12, 1175–1184. [Google Scholar] [CrossRef]
- Testa, L.; Latib, A.; De Marco, F.; De Carlo, M.; Agnifili, M.; Latini, R.A.; Petronio, A.S.; Ettori, F.; Poli, A.; De Servi, S.; et al. Clinical impact of persistent left bundle-branch block after transcatheter aortic valve implantation with CoreValve revalving system. Circulation 2013, 127, 1300–1307. [Google Scholar] [CrossRef] [Green Version]
- Urena, M.; Webb, J.G.; Cheema, A.; Serra, V.; Toggweiler, S.; Barbanti, M.; Cheung, A.; Ye, J.; Dumont, E.; DeLarochellière, R.; et al. Impact of new-onset persistent left bundle branch block on late clinical outcomes in patients undergoing transcatheter aortic valve implantation with a balloon-expandable valve. JACC Cardiovasc. Interv. 2014, 7, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Franzoni, I.; Latib, A.; Maisano, F.; Costopoulos, C.; Testa, L.; Figini, F.; Giannini, F.; Basavarajaiah, S.; Mussardo, M.; Slavich, M.; et al. Comparison of incidence and predictors of left bundle branch block after transcatheter aortic valve implantation using the corevalve versus the edwards valve. Am. J. Cardiol. 2013, 112, 554–559. [Google Scholar] [CrossRef]
- Faroux, L.; Chen, S.; Muntané-Carol, G.; Regueiro, A.; Philippon, F.; Sondergaard, L.; Jørgensen, T.H.; Lopez-Aguilera, J.; Kodali, S.; Leon, M.; et al. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: A systematic review and meta-analysis. Eur. Heart J. 2020, 41, 2771–2781. [Google Scholar] [CrossRef]
- Ferreira, N.D.; Caeiro, D.; Adão, L.; Oliveira, M.; Gonçalves, H.; Ribeiro, J.; Teixeira, M.; Albuquerque, A.; Primo, J.; Braga, P.; et al. Incidence and predictors of permanent pacemaker requirement after transcatheter aortic valve implantation with a self-expanding bioprosthesis. Pacing Clin. Electrophysiol. 2010, 33, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Van Rosendael, P.J.; Delgado, V.; Bax, J.J. Pacemaker implantation rate after transcatheter aortic valve implantation with early and new-generation devices: A systematic review. Eur. Heart J. 2018, 39, 2003–2013. [Google Scholar] [CrossRef] [PubMed]
- Rheude, T.; Pellegrini, C.; Lutz, J.; Alvarez-Covarrubias, H.A.; Lahmann, A.L.; Mayr, N.P.; Michel, J.; Kasel, M.A.; Joner, M.; Xhepa, E. Transcatheter Aortic Valve Replacement with Balloon-Expandable Valves: Comparison of SAPIEN 3 Ultra versus SAPIEN 3. JACC Cardiovasc. Interv. 2020, 13, 2631–2638. [Google Scholar] [CrossRef]
- Kalogeras, K.; Ruparelia, N.; Kabir, T.; Jabbour, R.; Naganuma, T.; Vavuranakis, M.; Nakamura, S.; Wang, B.; Sen, S.; Hadjiloizou, N.; et al. Comparison of the self-expanding Evolut-PRO transcatheter aortic valve to its predecessor Evolut-R in the real world multicenter ATLAS registry. Int. J. Cardiol. 2020, 310, 120–125. [Google Scholar] [CrossRef]
- Jilaihawi, H.; Zhao, Z.; Du, R.; Staniloae, C.; Saric, M.; Neuburger, P.J.; Querijero, M.; Vainrib, A.; Hisamoto, K.; Ibrahim, H.; et al. Minimizing Permanent Pacemaker Following Repositionable Self-Expanding Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 1796–1807. [Google Scholar] [CrossRef]
- Sammour, Y.; Krishnaswamy, A.; Kumar, A.; Puri, R.; Tarakji, K.G.; Bazarbashi, N.; Harb, S.; Griffin, B.; Svensson, L.; Wazni, O.; et al. Incidence, Predictors, and Implications of Permanent Pacemaker Requirement After Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2021, 14, 115–134. [Google Scholar] [CrossRef]
- Auffret, V.; Puri, R.; Urena, M.; Chamandi, C.; Rodriguez-Gabella, T.; Philippon, F.; Rodés-Cabau, J. Conduction disturbances after transcatheter aortic valve replacement: Current status and future perspectives. Circulation 2017, 136, 1049–1069. [Google Scholar] [CrossRef]
- Zaid, S.; Sengupta, A.; Okoli, K.; Tsoi, M.; Khan, A.; Ahmad, H.; Goldberg, J.B.; Undemir, C.; Rozenshtein, A.; Patel, N.; et al. Novel Anatomic Predictors of New Persistent Left Bundle Branch Block after Evolut Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2020, 125, 1222–1229. [Google Scholar] [CrossRef]
- Siontis, G.C.; Jüni, P.; Pilgrim, T.; Stortecky, S.; Büllesfeld, L.; Meier, B.; Wenaweser, P.; Windecker, S. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: A meta-analysis. J. Am. Coll. Cardiol. 2014, 64, 129–140. [Google Scholar] [CrossRef] [Green Version]
- Nazif, T.M.; Dizon, J.M.; Hahn, R.T.; Xu, K.E.; Babaliaros, V.; Douglas, P.S.; El-Chami, M.F.; Herrmann, H.C.; Mack, M.; Makkar, R.R.; et al. Predictors and clinical outcomes of permanent pacemaker implantation after transcatheter aortic valve replacement: The PARTNER (Placement of AoRtic TraNscathetER Valves) trial and registry. JACC Cardiovasc. Interv. 2015, 8, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Hamdan, A.; Guetta, V.; Klempfner, R.; Konen, E.; Raanani, E.; Glikson, M.; Goitein, O.; Segev, A.; Barbash, I.; Fefer, P.; et al. Inverse Relationship between Membranous Septal Length and the Risk of Atrioventricular Block in Patients Undergoing Transcatheter Aortic Valve Implantation. JACC Cardiovasc. Interv. 2015, 8, 1218–1228. [Google Scholar] [CrossRef]
- Rodés-Cabau, J. Optimizing Valve Implantation Depth to Win the Battle against Conduction Disturbances Post-TAVR. JACC Cardiovasc. Interv. 2019, 12, 1808–1810. [Google Scholar] [CrossRef]
- Gada, B.H.; Vora, A.N. Procedural Optimization to Minimize Interaction with the Left Ventricular Conduction System during Self-Expanding TAVR. Card. Interv. Today 2021, 15, 3–8. [Google Scholar]
- Hagar, A.; Li, Y.; Wei, X.; Peng, Y.; Xu, Y.; Ou, Y.; Wang, Z.; Wang, X.; Shah, J.P.; Sihag, V.; et al. Incidence, Predictors, and Outcome of Paravalvular Leak after Transcatheter Aortic Valve Implantation. J. Interv. Cardiol. 2020, 2020, 8249497. [Google Scholar] [CrossRef]
- Bettinger, N.; Khalique, O.K.; Krepp, J.M.; Hamid, N.B.; Bae, D.J.; Pulerwitz, T.C.; Liao, M.; Hahn, R.T.; Vahl, T.P.; Nazif, T.M.; et al. Practical determination of aortic valve calcium volume score on contrast-enhanced computed tomography prior to transcatheter aortic valve replacement and impact on paravalvular regurgitation: Elucidating optimal threshold cutoffs. J. Cardiovasc. Comput. Tomogr. 2017, 11, 302–308. [Google Scholar] [CrossRef]
- Rao, G.; Sheth, S.; Donnelly, J.; Scatola, A.; Tariq, U.; Laighold, S.; Grines, C.; Rutkin, B. Early Real-World Experience with CoreValve Evolut PRO and R Systems for Transcatheter Aortic Valve Replacement. J. Interv. Cardiol. 2019, 2019, 1906814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriyama, N.; Lehtola, H.; Miyashita, H.; Piuhola, J.; Niemelä, M.; Laine, M. Hemodynamic comparison of transcatheter aortic valve replacement with the SAPIEN 3 Ultra versus SAPIEN 3: The HomoSAPIEN registry. Catheter. Cardiovasc. Interv. 2020, 97, E982–E991. [Google Scholar]
- He, C.; Xiao, L.; Liu, J. Safety and efficacy of self-expandable Evolut R vs. balloon-expandable Sapien 3 valves for transcatheter aortic valve implantation: A systematic review and meta-analysis. Exp. Ther. Med. 2019, 18, 3893–3904. [Google Scholar] [CrossRef]
- Li, Y.M.; Tsauo, J.Y.; Liao, Y.B.; Zhao, Z.G.; Chen, M. Comparison of third generation balloon-expandable Edwards Sapien 3 versus self-expandable Evolut R in transcatheter aortic valve implantation: A meta-analysis. Ann. Cardiothorac. Surg. 2020, 9, 700–708. [Google Scholar]
- Mylotte, D.; Dorfmeister, M.; Elhmidi, Y.; Mazzitelli, D.; Bleiziffer, S.; Wagner, A.; Noterdaeme, T.; Lange, R.; Piazza, N. Erroneous measurement of the aortic annular diameter using 2-dimensional echocardiography resulting in inappropriate corevalve size selection: A retrospective comparison with multislice computed tomography. JACC Cardiovasc. Interv. 2014, 7, 652–661. [Google Scholar] [CrossRef] [Green Version]
- Masri, A.; Schoenhagen, P.; Svensson, L.; Kapadia, S.R.; Griffin, B.P.; Tuzcu, E.M.; Desai, M.Y. Dynamic characterization of aortic annulus geometry and morphology with multimodality imaging: Predictive value for aortic regurgitation after transcatheter aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2014, 147, 1847–1854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piayda, K.; Hellhammer, K.; Veulemans, V.; Sievert, H.; Gafoor, S.; Afzal, S.; Hennig, I.; Makosch, M.; Polzin, A.; Jung, C.; et al. Navigating the “Optimal Implantation Depth” with a Self-Expandable TAVR Device in Daily Clinical Practice. JACC Cardiovasc. Interv. 2020, 13, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Jilaihawi, H.; Chin, D.; Spyt, T.; Jeilan, M.; Vasa-Nicotera, M.; Bence, J.; Logtens, E.; Kovac, J. Prosthesis-patient mismatch after transcatheter aortic valve implantation with the Medtronic-Corevalve bioprosthesis. Eur. Heart J. 2010, 31, 857–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takagi, K.; Latib, A.; Al-Lamee, R.; Mussardo, M.; Montorfano, M.; Maisano, F.; Godino, C.; Chieffo, A.; Alfieri, O.; Colombo, A. Predictors of moderate-to-severe paravalvular aortic regurgitation immediately after CoreValve implantation and the impact of postdilatation. Catheter. Cardiovasc. Interv. 2011, 78, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Sherif, M.A.; Abdel-Wahab, M.; Stöcker, B.; Geist, V.; Richardt, D.; Tölg, R.; Richardt, G. Anatomic and procedural predictors of paravalvular aortic regurgitation after implantation of the medtronic CoreValve bioprosthesis. J. Am. Coll. Cardiol. 2010, 56, 1623–1629. [Google Scholar] [CrossRef] [Green Version]
- Dvir, D.; Webb, J.G.; Bleiziffer, S.; Pasic, M.; Waksman, R.; Kodali, S.; Barbanti, M.; Latib, A.; Schaefer, U.; Rodés-Cabau, J.; et al. Transcatheter Aortic Valve Implantation in Failed Bioprosthetic Surgical Valves. JAMA 2014, 312, 162–170. [Google Scholar] [CrossRef]
- Chen, H.L.; Liu, K. Clinical outcomes for transcatheter valve-in-valve in treating surgical bioprosthetic dysfunction: A meta-analysis. Int. J. Cardiol. 2016, 212, 138–141. [Google Scholar] [CrossRef]
- Ferrari, E.; Stortecky, S.; Heg, D.; Muller, O.; Nietlispach, F.; Tueller, D.; Toggweiler, S.; Noble, S.; Maisano, F.; Roffi, M.; et al. The hospital results and 1-year outcomes of transcatheter aortic valve-in-valve procedures and transcatheter aortic valve implantations in the native valves: The results from the Swiss-TAVI Registry. Eur. J. Cardio-Thorac. Surg. 2019, 56, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Webb, J.G.; Murdoch, D.J.; Alu, M.C.; Cheung, A.; Crowley, A.; Dvir, D.; Herrmann, H.C.; Kodali, S.K.; Leipsic, J.; Miller, D.C.; et al. 3-Year Outcomes after Valve-in-Valve Transcatheter Aortic Valve Replacement for Degenerated Bioprostheses: The PARTNER 2 Registry. J. Am. Coll. Cardiol. 2019, 73, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Hirji, S.A.; Percy, E.D.; Zogg, C.K.; Malarczyk, A.; Harloff, M.T.; Yazdchi, F.; Kaneko, T. Comparison of in-hospital outcomes and readmissions for valve-in-valve transcatheter aortic valve replacement vs. reoperative surgical aortic valve replacement: A contemporary assessment of real-world outcomes. Eur. Heart J. 2020, 41, 2747–2755. [Google Scholar] [CrossRef]
- Nalluri, N.; Atti, V.; Munir, A.B.; Karam, B.; Patel, N.J.; Kumar, V.; Vemula, P.; Edla, S.; Asti, D.; Paturu, A.; et al. Valve in valve transcatheter aortic valve implantation (ViV-TAVI) versus redo-Surgical aortic valve replacement (redo-SAVR): A systematic review and meta-analysis. J. Interv. Cardiol. 2018, 31, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Vrachatis, D.A.; Vavuranakis, M.; Tsoukala, S.; Giotaki, S.; Papaioannou, T.G.; Siasos, G.; Deftereos, G.; Giannopoulos, G.; Raisakis, K.; Tousoulis, D.; et al. TAVI: Valve in valve. A new field for structuralists? Literature review. Hell. J. Cardiol. 2020, 61, 148–153. [Google Scholar] [CrossRef]
- Bapat, V.; Attia, R.; Thomas, M. Effect of Valve Design on the Stent Internal Diameter of a Bioprosthetic Valve A Concept of True Internal Diameter and Its Implications for the Valve-in-Valve Procedure. JACC Cardiovasc. Interv. 2014, 7, 115–127. [Google Scholar] [CrossRef] [Green Version]
- Bapat, V. Valve-in-valve apps: Why and how they were developed and how to use them. EuroIntervention 2014, 10, U44–U51. [Google Scholar] [CrossRef] [Green Version]
- Bapat, V. Technical pitfalls and tips for the valve-in-valve procedure. Ann. Cardiothorac. Surg. 2017, 6, 541–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bapat, V.; Attia, R.; Redwood, S.; Hancock, J.; Wilson, K.; Young, C.; Thomas, M. Use of transcatheter heart valves for a valve-in-valve implantation in patients with degenerated aortic bioprosthesis: Technical considerations and results. J. Thorac. Cardiovasc. Surg. 2012, 144, 1372–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fede, A.; Romano, M.; Buffoli, F.; Camurri, N.; Lettieri, C. Combination of Double Chimney Technique and Prosthesis Post-Dilation after Valve-in-Valve Implantation. Case Rep. 2020, 2, 2173–2175. [Google Scholar] [CrossRef]
- Mercanti, F.; Rosseel, L.; Neylon, A.; Bagur, R.; Sinning, J.M.; Nickenig, G.; Grube, E.; Hildick-Smith, D.; Tavano, D.; Wolf, A.; et al. Chimney Stenting for Coronary Occlusion during TAVR: Insights from the Chimney Registry. JACC Cardiovasc. Interv. 2020, 13, 751–761. [Google Scholar] [CrossRef]
- Palmerini, T.; Chakravarty, T.; Saia, F.; Bruno, A.G.; Bacchi-Reggiani, M.L.; Marrozzini, C.; Patel, C.; Patel, V.; Testa, L.; Bedogni, F.; et al. Coronary Protection to Prevent Coronary Obstruction during TAVR: A Multicenter International Registry. JACC Cardiovasc. Interv. 2020, 13, 739–747. [Google Scholar] [CrossRef]
- Lederman, R.J.; Babaliaros, V.C.; Rogers, T.; Khan, J.M.; Kamioka, N.; Dvir, D.; Greenbaum, A.B. Preventing Coronary Obstruction during Transcatheter Aortic Valve Replacement: From Computed Tomography to BASILICA. JACC Cardiovasc. Interv. 2019, 12, 1197–1216. [Google Scholar] [CrossRef]
- Noorani, A.; Radia, R.; Bapat, V. Challenges in valve-in-valve therapy. J. Thorac. Dis. 2015, 7, 1501–1508. [Google Scholar]
- Nielsen-Kudsk, J.E.; Christiansen, E.H.; Terkelsen, C.J.; Nørgaard, B.L.; Jensen, K.T.; Krusell, L.R.; Tang, M.; Terp, K.; Klaaborg, K.E.; Andersen, H.R. Fracturing the Ring of Small Mitroflow Bioprostheses by High-Pressure Balloon Predilatation in Transcatheter Aortic Valve-in-Valve Implantation. Circ. Cardiovasc. Interv. 2015, 8, e002667. [Google Scholar] [CrossRef] [Green Version]
- Dvir, D.; Khan, J.; Kornowski, R.; Komatsu, I.; Chatriwalla, A.; Mackenson, G.B.; Simonato, M.; Ribeiro, H.; Wood, D.; Leipsic, J.; et al. Novel strategies in aortic valve-in-valve therapy including bioprosthetic valve fracture and BASILICA. EuroIntervention 2018, 14, AB74–AB82. [Google Scholar] [CrossRef]
- Vahidkhah, K.; Javani, S.; Abbasi, M.; Azadani, P.N.; Tandar, A.; Dvir, D.; Azadani, A.N. Blood Stasis on Transcatheter Valve Leaflets and Implications for Valve-in-Valve Leaflet Thrombosis. Ann. Thorac. Surg. 2017, 104, 751–759. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, D.C.; Okutucu, S.; Russo, G.; Martins, E.C. The Issue of Subclinical Leaflet Thrombosis after Transcatheter Aortic Valve Implantation. Cardiol. Res. 2020, 11, 269–273. [Google Scholar] [CrossRef]
- Makkar, R.R.; Blanke, P.; Leipsic, J.; Thourani, V.; Chakravarty, T.; Brown, D.; Trento, A.; Guyton, R.; Babaliaros, V.; Williams, M.; et al. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves. J. Am. Coll. Cardiol. 2020, 75, 3003–3015. [Google Scholar] [CrossRef]
- Ruiz, C.E.; Laborde, J.C.; Condado, J.F.; Chiam, P.T.; Condado, J.A. First percutaneous transcatheter aortic valve-in-valve implant with three year follow-up. Catheter. Cardiovasc. Interv. 2008, 72, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, A.; Jastrzebski, J.; Dabrowski, M.; Chmielak, Z. Second Transcatheter Aortic Valve Implantation for Treatment of Suboptimal Function of Previously Implanted Prosthesis: Review of the Literature. J. Interv. Cardiol. 2014, 27, 300–307. [Google Scholar] [CrossRef]
- Eftychiou, C.; Kokkinos, C.; Evangelakis, E.; Houri, S.; Simamonian, K.; Yiannikourides, V.; Maimaris, M.; Cassese, M. Repeated transapical TAVI for the treatment of a degenerated bioprosthetic valve. Hell. J. Cardiol. 2018, 59, 40–42. [Google Scholar] [CrossRef] [PubMed]
- De Backer, O.; Landes, U.; Fuchs, A.; Yoon, S.H.; Mathiassen, O.N.; Sedaghat, A.; Kim, W.K.; Pilgrim, T.; Buzzatti, N.; Ruile, P.; et al. Coronary Access after TAVR-in-TAVR as Evaluated by Multidetector Computed Tomography. JACC Cardiovasc. Interv. 2020, 13, 2528–2538. [Google Scholar] [CrossRef]
- Tang, G.H.; Zaid, S.; Fuchs, A.; Yamabe, T.; Yazdchi, F.; Gupta, E.; Ahmad, H.; Kofoed, K.F.; Goldberg, J.B.; Undemir, C.; et al. Alignment of Transcatheter Aortic-Valve Neo-Commissures (ALIGN TAVR): Impact on Final Valve Orientation and Coronary Artery Overlap. JACC Cardiovasc. Interv. 2020, 13, 1030–1042. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SENTINEL™ Cerebral Protection System | TriGuard™ | Embrella Embolic Deflector Device | Wirion Embolic Protection System | Embol-X | Point-Guard™ Dynamic Cerebral Embolic Protection | ProtEmbo® Cerebral Protection System | Emblok Embolic Protection System with Modified Pigtail Catheter | Emboliner™ Total Embolic Protection Catheter | Captis™ Embolic Protection System | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mechanism | Capture | Deflection | Deflection | Capture | Capture | Deflection | Deflection | Capture | Capture | Capture |
| Access site and delivery approach | Radial artery–6 Fr | Femoral artery–9 Fr | Radial/brachial artery–6 Fr | Radial/brachial artery–6 Fr | Direct aortic–14 Fr | Unclear | Left radial–6 Fr | Femoral artery–11 Fr | Femoral artery | Femoral artery |
| Coverage | Partial protection * | Full protection ** | Partial protection * | Partial protection * | Full protection ** | Full protection ** | Full protection ** | Full protection ** | Full protection (cerebral and peripheral vessels) | Full protection (cerebral and peripheral vessels) |
| Mesh pore size (µm) | 140 | 140 | 100 | 120 | 120 | - | 60 | 125 | - | - |
| Main evidence | MISTRAL-C; CLEAN-TAVI; SENTINEL | DEFLECT I-III | PROTAVI-C | WISE | Wendt D, Ann Thorac Surg 2015 | - | - | Latib A, JACC Cardiovasc Interv. 2020 | Pasupati S, J Am Coll Cardiol. 2020 | - |
| Ongoing trial | PROTECTED- TAVR | REFLECT | - | - | - | - | PROTEMBO SF Trial | - | - | CAPTIS® Study |
| Manufacturer | Boston Scientific, Marlborough, MA, USA | Keystone Heart Ltd., Caesarea, Israel | Edwards Lifesciences, Irvine, CA, United States | Cardiovascular Systems Inc., St. Paul, MN, USA | Edwards Lifesciences Corp., Irvine, CA, USA | Transverse Medical Inc., Denver, CO, USA | Protembis, Aachen, Germany | Innovative Cardiovascular Solutions, Grand Rapids, MI, USA | Emboline Inc., Santa Cruz, CA, USA | Filterlex Medical Ltd., Yokneam, Israel |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciardetti, N.; Ciatti, F.; Nardi, G.; Di Muro, F.M.; Demola, P.; Sottili, E.; Stolcova, M.; Ristalli, F.; Mattesini, A.; Meucci, F.; et al. Advancements in Transcatheter Aortic Valve Implantation: A Focused Update. Medicina 2021, 57, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070711
Ciardetti N, Ciatti F, Nardi G, Di Muro FM, Demola P, Sottili E, Stolcova M, Ristalli F, Mattesini A, Meucci F, et al. Advancements in Transcatheter Aortic Valve Implantation: A Focused Update. Medicina. 2021; 57(7):711. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070711
Chicago/Turabian StyleCiardetti, Niccolò, Francesca Ciatti, Giulia Nardi, Francesca Maria Di Muro, Pierluigi Demola, Edoardo Sottili, Miroslava Stolcova, Francesca Ristalli, Alessio Mattesini, Francesco Meucci, and et al. 2021. "Advancements in Transcatheter Aortic Valve Implantation: A Focused Update" Medicina 57, no. 7: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070711