
Previous Catheter Ablation Predicts In-Hospital Restoration of Sinus Rhythm in Patients Presenting with Recent-Onset Atrial Fibrillation—The Retrospective HAMBURG-AF Study


 and
and
Abstract
:1. Introduction
2. Materials and Methods
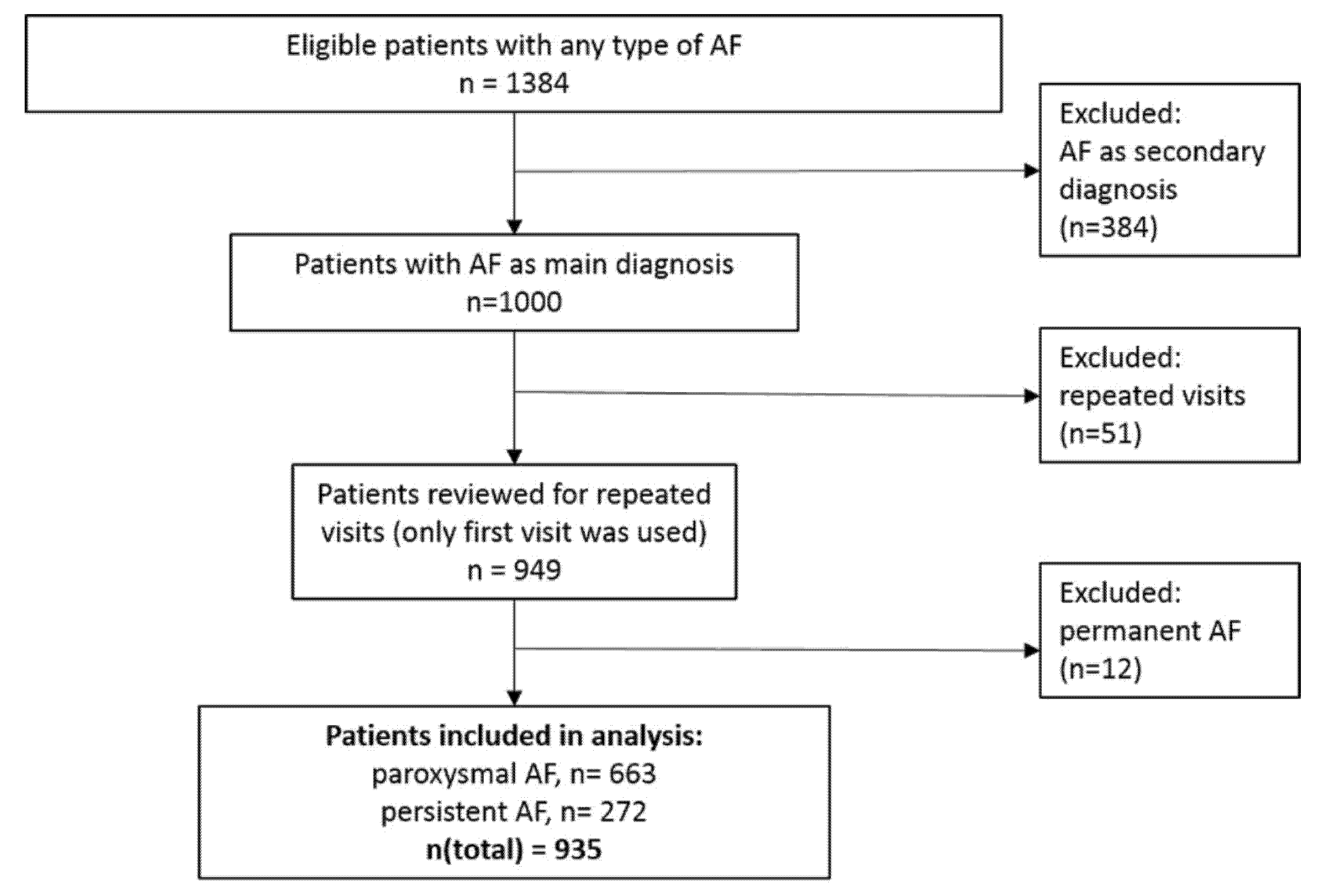
2.1. Patients and Study Variables
2.2. Statistical Analyses
3. Results
4. Discussion
4.1. Pathophysiological Insights
4.2. Translational Perspective
4.3. Strengths and Limitations
5. Conclusions and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, B.A.; Honushefsky, A.M.; Berger, P.B. Temporal Trends in the Incidence, Prevalence, and Survival of Patients With Atrial Fibrillation From 2004 to 2016. Am. J. Cardiol. 2017, 120, 1961–1965. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.F.; Liu, C.-J.; Tuan, T.-C.; Chen, T.-J.; Hsieh, M.-H.; Lip, G.Y.H.; Chen, S.-A. Lifetime Risks, Projected Numbers, and Adverse Outcomes in Asian Patients with Atrial Fibrillation: A Report from the Taiwan Nationwide AF Cohort Study. Chest 2018, 153, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnabel, R.B.; Wilde, S.; Wild, P.S.; Munzel, T.; Blankenberg, S. Atrial fibrillation: Its prevalence and risk factor profile in the German general population. Dtsch. Arztebl. Int. 2012, 109, 293–299. [Google Scholar]
- Conen, D.; Chae, C.U.; Glynn, R.J.; Tedrow, U.B.; Everett, B.M.; Buring, J.E.; Albert, C.M. Risk of death and cardiovascular events in initially healthy women with new-onset atrial fibrillation. JAMA 2011, 305, 2080–2087. [Google Scholar] [CrossRef] [Green Version]
- Vermond, R.A.; Geelhoed, B.; Verweij, N.; Tieleman, R.G.; Van der Harst, P.; Hillege, H.L.; Van Gilst, W.H.; Van Gelder, I.C.; Rienstra, M. Incidence of Atrial Fibrillation and Relationship With Cardiovascular Events, Heart Failure, and Mortality: A Community-Based Study From the Netherlands. J. Am. Coll. Cardiol. 2015, 66, 1000–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krijthe, B.P.; Kunst, A.; Benjamin, E.J.; Lip, G.Y.H.; Franco, O.H.; Hofman, A.; Witteman, J.C.M.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef] [Green Version]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Freedman, B.; Camm, J.; Calkins, H.; Healey, J.S.; Rosenqvist, M.; Wang, J.; Albert, C.M.; Anderson, C.S.; Antoniou, S.; Benjamin, E.J.; et al. Screening for Atrial Fibrillation: A Report of the AF-SCREEN International Collaboration. Circulation 2017, 135, 1851–1867. [Google Scholar] [CrossRef]
- Gu, Y.; Doughty, R.N.; Freedman, B.; Kennelly, J.; Warren, J.; Harwood, M.; Hulme, R.; Paltridge, C.; Teh, R.; Rolleston, A.; et al. Burden of Atrial Fibrillation in Māori and Pacific People in New Zealand: A Cohort Study. Intern. Med. J. 2017, 48, 301–309. [Google Scholar] [CrossRef]
- Healey, J.S. What do implanted cardiac monitors reveal about atrial fibrillation? JAMA Cardiol. 2017, 2, 1128–1129. [Google Scholar] [CrossRef]
- Magnussen, C.; Niiranen, T.J.; Ojeda, F.M.; Gianfagna, F.; Blankenberg, S.; Njolstad, I.; Vartiainen, E.; Sans, S.; Pasterkamp, G.; Hughes, M.; et al. Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results from the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe). Circulation 2017, 136, 1588–1597. [Google Scholar] [CrossRef] [Green Version]
- Ganesan, A.N.; Shipp, N.J.; Brooks, A.G.; Kuklik, P.; Lau, D.H.; Lim, H.S.; Sullivan, T.; Roberts-Thomson, K.C.; Sanders, P. Long-term outcomes of catheter ablation of atrial fibrillation: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.M.; Webster, L.; Qiu, F.; Austin, P.C.; Ko, D.T.; Tu, J.V.; Wijeysundera, H.C. Effect of Electrophysiology Assessment on Mortality and Hospitalizations in Patients With New-Onset Atrial Fibrillation. Am. J. Cardiol. 2018, 121, 830–835. [Google Scholar] [CrossRef]
- Steinberg, J.S.; Palekar, R.; Sichrovsky, T.; Arshad, A.; Preminger, M.; Musat, D.; Shaw, R.E.; Mittal, S. Very long-term outcome after initially successful catheter ablation of atrial fibrillation. Hear. Rhythm. 2014, 11, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Sultan, A.; Luker, J.; Andresen, D.; Kuck, K.H.; Hoffmann, E.; Brachmann, J.; Hochadel, M.; Willems, S.; Eckardt, L.; Lewalter, T.; et al. Predictors of Atrial Fibrillation Recurrence after Catheter Ablation: Data from the German Ablation Registry. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarman, J.W.; Hunter, T.D.; Hussain, W.; March, J.L.; Wong, T.; Markides, V. Mortality, stroke, and heart failure in atrial fibrillation cohorts after ablation versus propensity-matched cohorts. Pragmatic Obs. Res. 2017, 8, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, J.B.; Fritsche, L.G.; Zhou, W.; Teslovich, T.M.; Holmen, O.L.; Gustafsson, S.; Gabrielsen, M.E.; Schmidt, E.M.; Beaumont, R.; Wolford, B.N.; et al. Genome-wide Study of Atrial Fibrillation Identifies Seven Risk Loci and Highlights Biological Pathways and Regulatory Elements Involved in Cardiac Development. Am. J. Hum. Genet. 2018, 102, 103–115. [Google Scholar] [CrossRef] [Green Version]
- Husser, D.; Buttner, P.; Stubner, D.; Ueberham, L.; Platonov, P.G.; Dinov, B.; Arya, A.; Hindricks, G.; Bollmann, A. PR interval associated genes, atrial remodeling and rhythm outcome of catheter ablation of atrial fibrillation-A gene-based analysis of GWAS data. Front. Genet. 2017, 8, 224. [Google Scholar] [CrossRef] [Green Version]
- Tian, Y.; Wang, Y.; Chen, W.; Yin, Y.; Qin, M. Role of serum TGF-β1 level in atrial fibrosis and outcome after catheter ablation for paroxysmal atrial fibrillation. Medicines 2017, 96, 2017. [Google Scholar] [CrossRef]
- Scridon, R.C.Ş.; Chevalier, P. Atrial fibrillation: Neurogenic or myogenic? Arch. Cardiovasc. Dis. 2017, 111, 59–69. [Google Scholar] [CrossRef]
- Maupoil, V.; Bronquard, C.; Cosnay, J.-L.P.; Findlay, I. Ectopic activity in the rat pulmonary vein can arise from simultaneous activation of alpha1- and beta1-adrenoceptors. Br. J. Pharmacol. 2007, 150, 899–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heijman, J.; Kirchner, D.; Kunze, F.; Chretien, E.M.; Michel-Reher, M.B.; Voigt, N.; Knaut, M.; Michel, M.C.; Ravens, U.; Dobrev, D. Muscarinic type-1 receptors contribute to IK, AChin human atrial cardiomyocytes and are upregulated in patients with chronic atrial fibrillation. Int. J. Cardiol. 2018, 255, 61–68. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All (N = 935) | Paroxysmal (N = 663) | Persistent (N = 272) | p-Value | |
|---|---|---|---|---|
| Male No. (%) | 437 (46.7) | 303 (45.7) | 134 (49.3) | 0.36 |
| Age (years) | 75.0 (65.0, 81.0) | 75.0 (65.0, 81.0) | 74.0 (65.0, 79.0) | 0.064 |
| First diagnosis of AF at ED No. (%) | 342 (36.7) | 294 (44.5) | 48 (17.7) | <0.001 |
| Hypertension No. (%) | 644 (69.0) | 456 (69.0) | 188 (69.1) | 1.00 |
| Dyslipidemia No. (%) | 147 (16.8) | 90 (14.7) | 57 (21.6) | 0.016 |
| Diabetes mellitus No. (%) | 125 (13.4) | 86 (13.0) | 39 (14.3) | 0.65 |
| Family history of CAD No. (%) | 67 (7.2) | 34 (5.2) | 33 (12.2) | <0.001 |
| CAD No. (%) | 200 (21.5) | 139 (21.1) | 61 (22.4) | 0.72 |
| max NT-proBNP (ng/L) | 2779 (1081, 6262) | 2426 (1015, 5719) | 3588 (1549, 6951) | 0.020 |
| Concomitant bacterial infection No. (%) | 265 (28.3) | 204 (30.8) | 61 (22.4) | 0.013 |
| Current smoker No. (%) | 91 (9.8) | 67 (10.1) | 24 (8.8) | 0.027 |
| Never smoked No. (%) | 732 (78.5) | 528 (79.9) | 204 (75.0) | |
| Ex-smoker No. (%) | 110 (11.8) | 66 (10.0) | 44 (16.2) | |
| Conversion during hospital stay No. (%) | 610 (66.3) | 443 (68.4) | 167 (61.4) | 0.050 |
| Conversion due to medication No. (%) | 210 (22.8) | 193 (29.6) | 17 (6.3) | <0.001 |
| Conversion due to electric CV No. (%) | 345 (37.1) | 208 (31.6) | 137 (50.4) | <0.001 |
| Secondary AF No. (%) | 234 (25.1) | 191 (28.9) | 43 (15.8) | <0.001 |
| Previous ablations No. (%) | 176 (18.9) | 75 (11.3) | 101 (37.4) | <0.001 |
| Existing antiarrhythmic medics No. (%) | 598 (64.2) | 400 (60.6) | 198 (72.8) | <0.001 |
| Administration of K+ No. (%) | 319 (34.2) | 228 (34.5) | 91 (33.5) | 0.82 |
| Administration of Mg+ No. (%) | 613 (65.6) | 433 (65.4) | 180 (66.2) | 0.88 |
| Administration of beta-blocker No. (%) | 615 (65.8) | 438 (66.2) | 177 (65.1) | 0.81 |
| Hx previous electric cardioversion No. (%) | 258 (27.7) | 108 (16.3) | 150 (55.6) | <0.001 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Secondary AF | 0.37 (0.26, 0.51) | <0.001 |
| Previous ablations | 3.87 (2.40, 6.54) | <0.001 |
| Existing antiarrhythmic medication | 0.89 (0.65, 1.20) | 0.44 |
| Administration of K+ | 1.35 (0.99, 1.85) | 0.056 |
| Administration of Mg+ | 2.32 (1.72, 3.13) | <0.001 |
| Administration of beta-blocker | 1.91 (1.41, 2.57) | <0.001 |
| First diagnosis of AF at ED presentation | 0.87 (0.65, 1.17) | 0.36 |
| Hypertension | 1.11 (0.80, 1.52) | 0.53 |
| Dyslipidemia | 1.12 (0.75, 1.67) | 0.59 |
| Diabetes mellitus | 0.69 (0.46, 1.04) | 0.075 |
| Family history of CAD | 2.57 (1.30, 5.70) | 0.011 |
| Known CAD | 0.87 (0.62, 1.24) | 0.43 |
| Previous electric cardioversion | 2.54 (1.77, 3.70) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulte-Steinberg, B.; Aydin, M.A.; Moser, A.T.; Ojeda, F.; Karakas, M. Previous Catheter Ablation Predicts In-Hospital Restoration of Sinus Rhythm in Patients Presenting with Recent-Onset Atrial Fibrillation—The Retrospective HAMBURG-AF Study. Medicina 2021, 57, 776. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080776
Schulte-Steinberg B, Aydin MA, Moser AT, Ojeda F, Karakas M. Previous Catheter Ablation Predicts In-Hospital Restoration of Sinus Rhythm in Patients Presenting with Recent-Onset Atrial Fibrillation—The Retrospective HAMBURG-AF Study. Medicina. 2021; 57(8):776. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080776
Chicago/Turabian StyleSchulte-Steinberg, Benedict, Muhammet Ali Aydin, Ana Theresa Moser, Francisco Ojeda, and Mahir Karakas. 2021. "Previous Catheter Ablation Predicts In-Hospital Restoration of Sinus Rhythm in Patients Presenting with Recent-Onset Atrial Fibrillation—The Retrospective HAMBURG-AF Study" Medicina 57, no. 8: 776. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080776