
Combined Microwave Ablation and Osteosynthesis for Long Bone Metastases

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
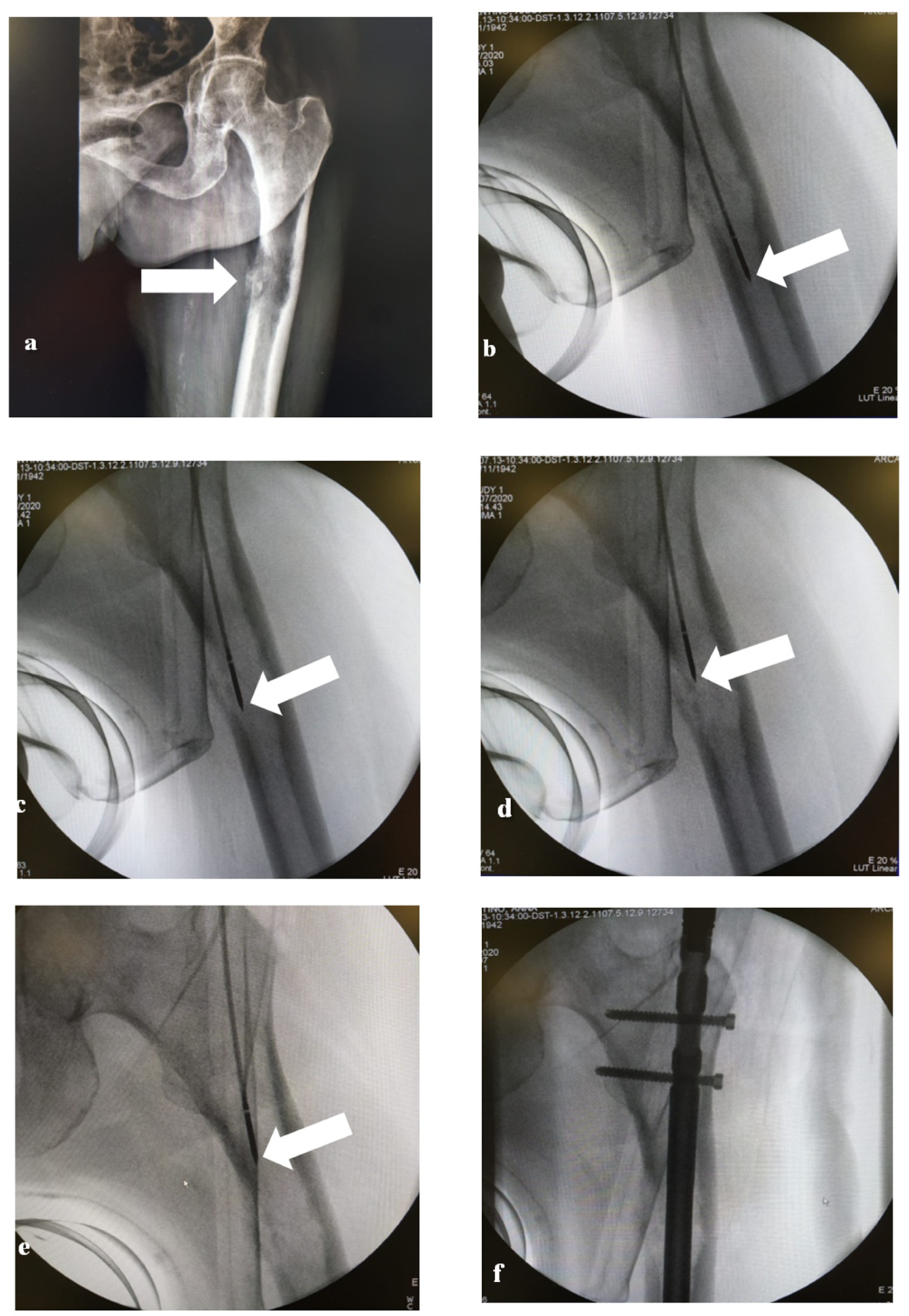
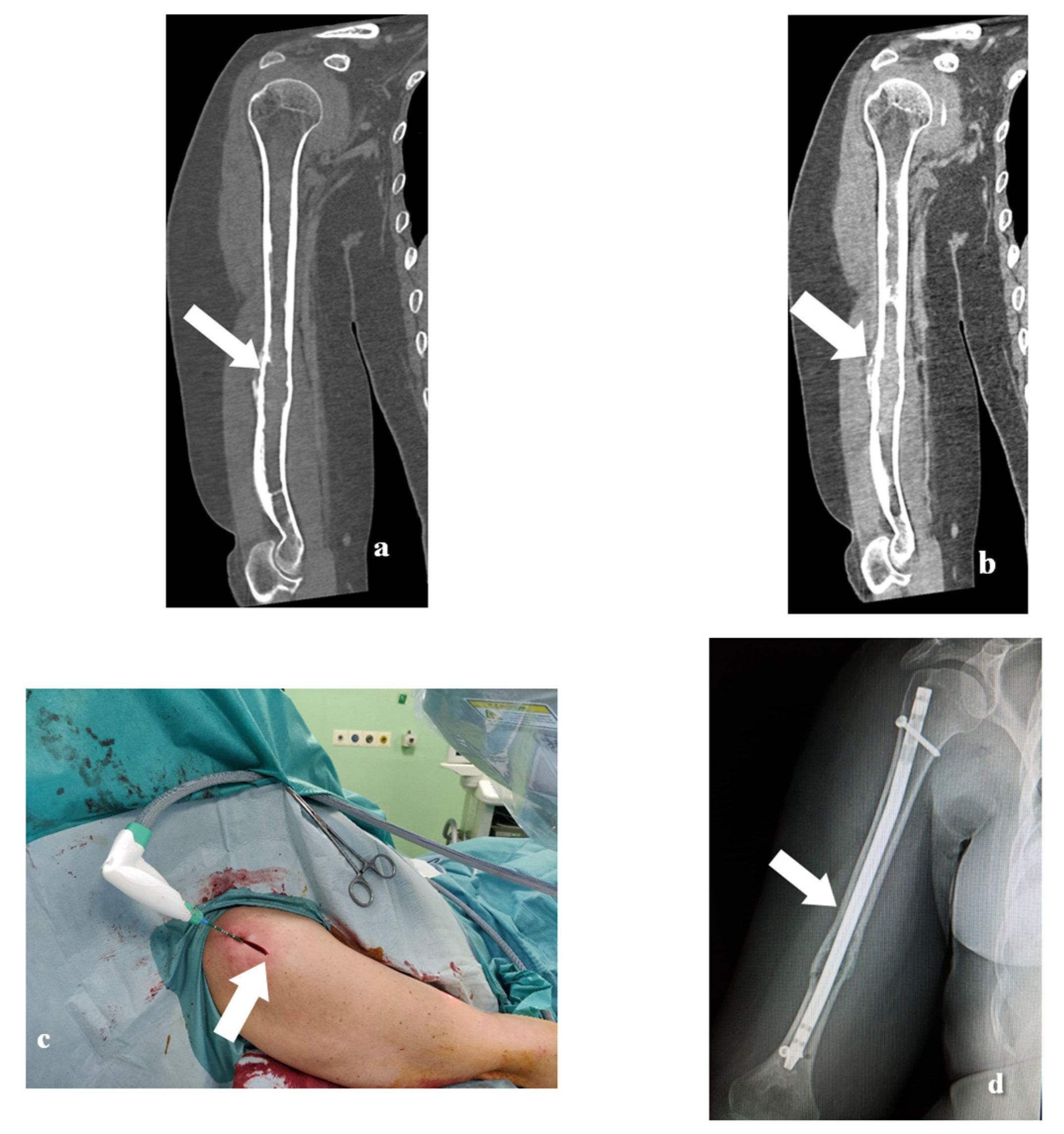
2.2. MWA Technique
2.3. Surgical Technique
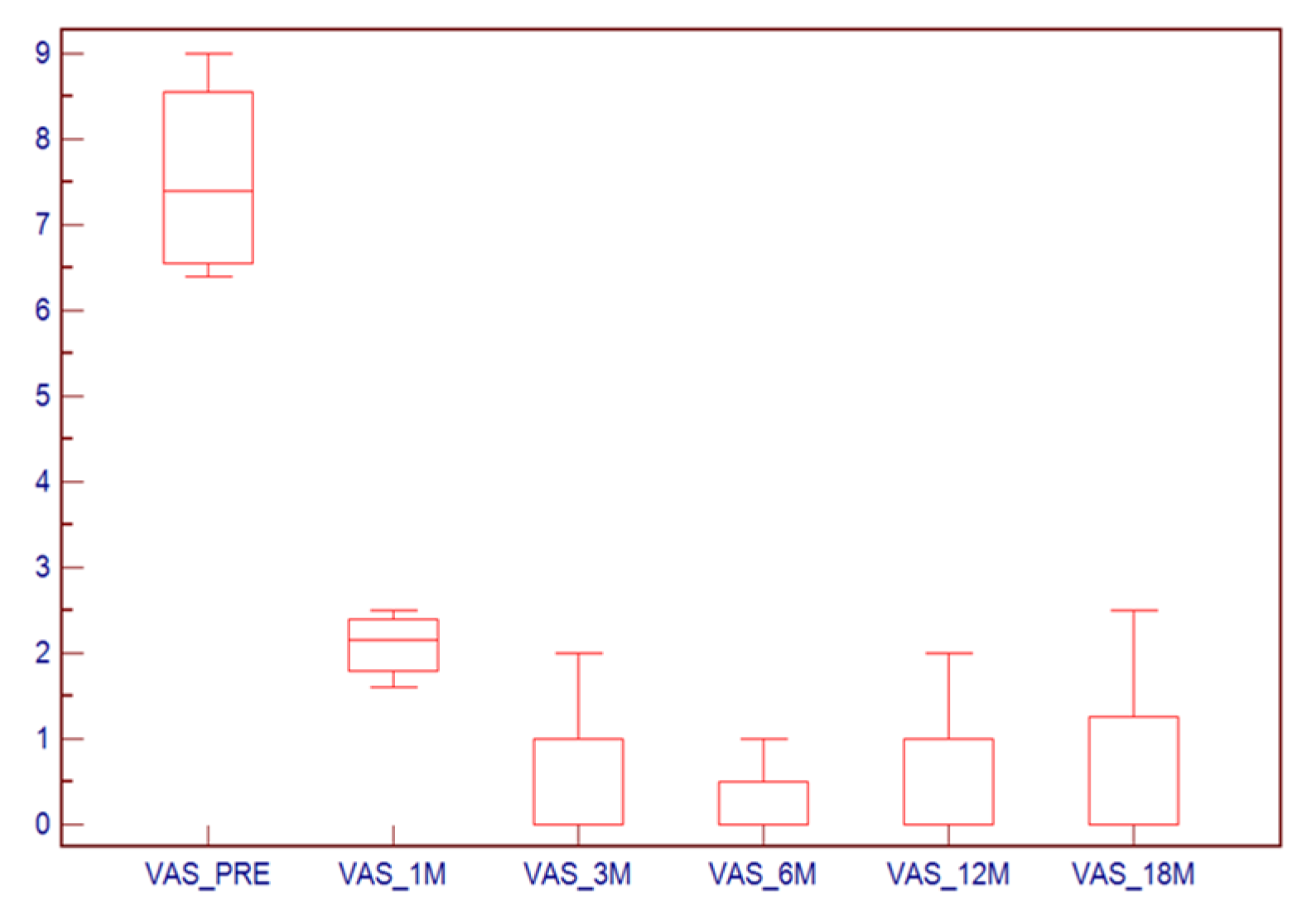
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jacofsky, D.J.; Haidukewych, G.J.; Zhang, H.; Sim, F.H. Complications and results of arthroplasty for salvage of failed treatment of malignant pathologic fractures of the hip. Clin. Orthop. Relat. Res. 2004, 427, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Hage, W.D.; Aboulafia, A.J.; Aboulafia, D.M. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop. Clin. North Am. 2000, 31, 515–528. [Google Scholar] [CrossRef]
- Capanna, R.; Campanacci, D.A. The Treatment Of Metastases In The Appendicular Skeleton. J. Bone Joint Surg. 2001, 83, 471–481. [Google Scholar] [CrossRef]
- Angelini, A.; Trovarelli, G.; Berizzi, A.; Pala, E.; Breda, A.; Maraldi, M.; Ruggieri, P. Treatment of pathologic fractures of the proximal femur. Injury 2018, 49, S77–S83. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Mirza, A.N.; Lin, P.P.; Lewis, V.O.; Yasko, A.W. Proximal femoral endoprosthesis for the treatment of metastatic. Orthopedics 2008, 31, 361. [Google Scholar] [CrossRef] [PubMed]
- Dijstra, S.; Wiggers, T.; Van Geel, B.N.; Boxma, H. Impending and actual pathological fractures in patients with bone metastases of the long bones. A retrospective study of 233 surgically treated fractures. Eur. J. Surg. Acta Chir. 1994, 160, 535–542. [Google Scholar]
- Winter, T.C.; Laeseke, P.F.; Lee, F.T. Focal tumor ablation: A new era in cancer therapy. Ultrasound Q. 2006, 22, 195–217. [Google Scholar] [CrossRef] [PubMed]
- Fan, Q.Y.; Zhou, Y.; Zhang, M.; Ma, B.; Yang, T.; Long, H.; Yu, Z.; Li, Z. Microwave ablation of primary malignant pelvic bone tumors. Front. Surg. 2019, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.J.; va der Linden, Y.M.; va de Sande, M.A.J.; Dijkstra, P.D.S. Treatment of pathological fractures of the long bones. EFORT Open Rev. 2016, 1, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Kuo, P.L. Bone metastasis from renal cell carcinoma. Int. J. Mol. Sci. 2016, 17, 987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Q.; Ma, B.; Guo, A. Treatment of malignant or aggressive bone tumors with microwave induced hyperthermia. Chin. J. Surg. 1997, 35, 484–487. [Google Scholar] [PubMed]
- Fan, Q.; Ma, B.; Guo, A.; Li, Y.; Ye, J.; Zhou, Y.; Qiu, X. Surgical treatment of bone tumors in conjunction with microwave-induced hyperthermia and adjuvant immunotherapy: A preliminary report. Chin. Med. J. 1996, 109, 425–431. [Google Scholar] [PubMed]
- Pap, D.P.; Mayerson, J.L.; Scharschmidt, T.J. Soft tissue tumor recurrence after intramedullary stabilization of impending pathologic fractures. Orthopedics 2012, 35, e448–e452. [Google Scholar] [CrossRef] [Green Version]
- Miller, B.J.; Carmody Soni, E.E.; Gibbs, C.P.; Scarborough, M.T. Intramedullary nails for long bone metastases: Why do they fail? Orthopedics 2011, 34, 4. [Google Scholar] [CrossRef] [PubMed]
- Locklin, J.K.; Mannes, A.; Berger, A.; Wood, B.J. Palliation of soft tissue cancer pain with radiofrequency ablation. J. Support. Oncol. 2004, 2, 439–445. [Google Scholar]
- Carrafiello, G.; Laganà, D.; Ianniello, A.; Nicotera, P.; Fontana, F.; Dizonno, M.; Cuffari, S.; Fugazzola, C. Radiofrequency thermal ablation for pain control in patients with single painful bone metastasis from hepatocellular carcinoma. Eur. J. Radiol. 2009, 71, 363–368. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Sex | Age | Primary Tumor | Localization of Bone Metastases | Size of Metastases (cm) | Fracture Type | Mirels’ Score | No. of MW Antenna Placements | MW Power/Time |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 68 | Prostate | Humerus | 10.0 | IF | 8 | 4 | 50 W 3 min |
| 2 | F | 81 | Breast | Femur | 16.5 | AF | - | 5 | 60 W 3 min |
| 3 | F | 57 | Breast | Femur | 3.0 | IF | 7 | 1 | 50 W 3 min |
| 4 | F | 58 | Breast | Femur | 5.0 | IF | 8 | 3 | 50 W 3 min |
| 5 | F | 56 | Breast | Humerus | 7.5 | IF | 7 | 4 | 50 W 3 min |
| 6 | F | 56 | Breast | Humerus | 4.0 | IF | 8 | 2 | 50 W 3 min |
| 7 | M | 60 | NSCLC | Femur | 5.4 | IF | 8 | 4 | 50 W 3 min |
| 8 | M | 75 | Kidney | Humerus | 3.5 | IF | 8 | 2 | 50 W 3 min |
| 9 | F | 54 | Breast | Femur | 7.5 | IF | 10 | 4 | 60 W 3 min |
| 10 | F | 72 | CRC | Tibia | 5.3 | IF | 8 | 4 | 50 W 3 min |
| 11 | M | 52 | MM | Femur | 6.9 | IF | 9 | 4 | 50 W 3 min |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pusceddu, C.; Dessì, G.; Melis, L.; Fancellu, A.; Ruggiu, G.; Sailis, P.; Congia, S.; Derudas, D.; Cau, R.; Senis, I.; et al. Combined Microwave Ablation and Osteosynthesis for Long Bone Metastases. Medicina 2021, 57, 825. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080825
Pusceddu C, Dessì G, Melis L, Fancellu A, Ruggiu G, Sailis P, Congia S, Derudas D, Cau R, Senis I, et al. Combined Microwave Ablation and Osteosynthesis for Long Bone Metastases. Medicina. 2021; 57(8):825. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080825
Chicago/Turabian StylePusceddu, Claudio, Giuseppe Dessì, Luca Melis, Alessandro Fancellu, Giuseppe Ruggiu, Paolo Sailis, Stefano Congia, Daniele Derudas, Riccardo Cau, Ignazio Senis, and et al. 2021. "Combined Microwave Ablation and Osteosynthesis for Long Bone Metastases" Medicina 57, no. 8: 825. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080825