
Reduced External Iliac Venous Blood Flow Rate Is Associated with Asymptomatic Compression of the Common Iliac Veins

 , , and
, , and
Abstract
:1. Introduction
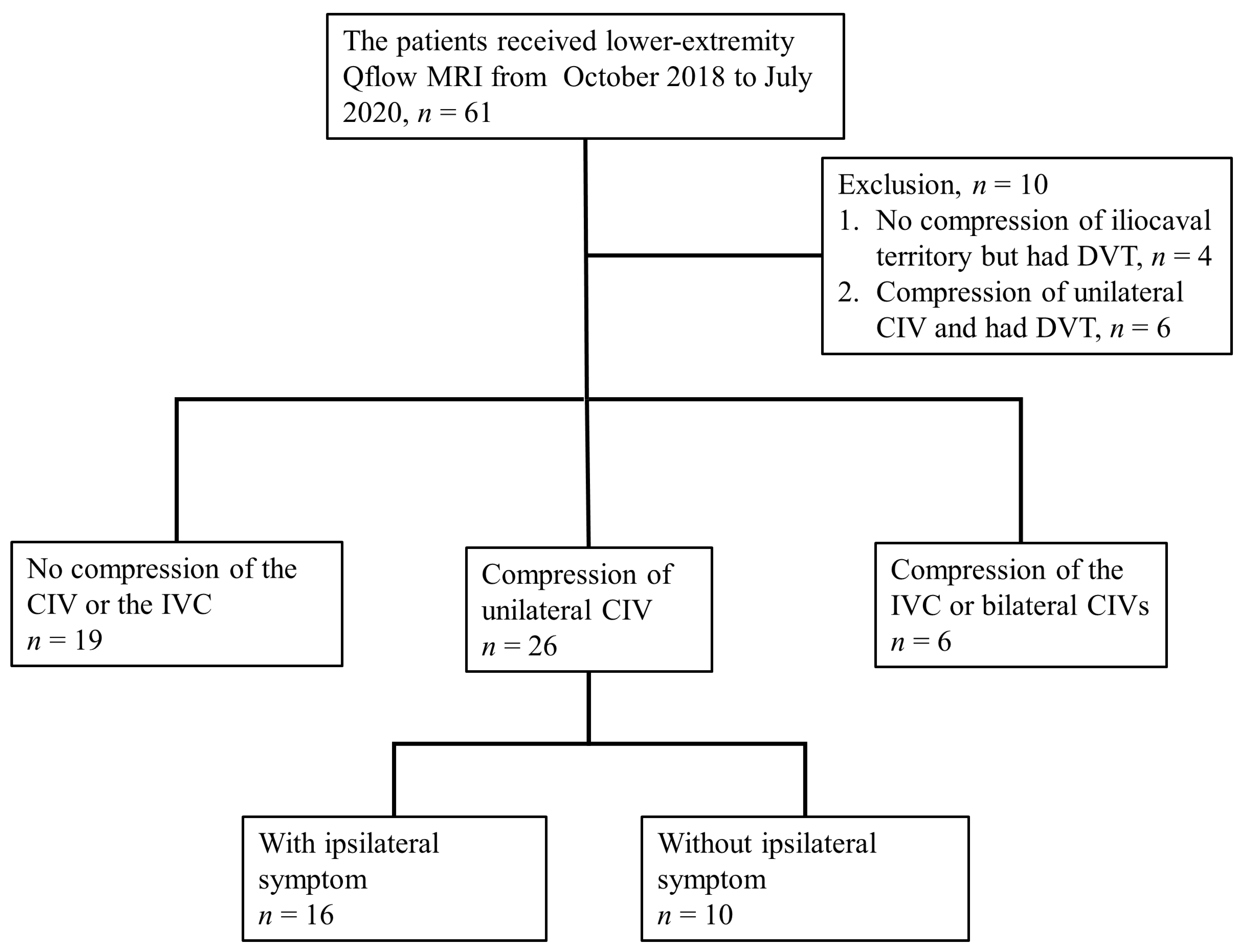
2. Materials and Methods
Statistical Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brinegar, K.N.; Sheth, R.A.; Khademhosseini, A.; Bautista, J.; Oklu, R. Iliac vein compression syndrome: Clinical, imaging and pathologic findings. World J. Radiol. 2015, 7, 375–381. [Google Scholar] [CrossRef]
- Fretz, V.; Binkert, C.A. Compression of the inferior vena cava by the right iliac artery: A rare variant of May-Thurner syndrome. Cardiovasc. Interv. Radiol. 2010, 33, 1060–1063. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.Y. May-Thurner syndrome. In UpToDate; Collins, K.A., Ed.; UpToDate: Waltham, MA, USA, 2019; Available online: https://www.uptodate.com/contents/may-thurner-syndrome (accessed on 16 July 2019).
- Tarannum, N.; Lakshman, K.H.V.V.S.S.; Azam, M.S.; Premchand, R.K. May-Thurner Syndrome and Recurrent DVT: A Case Report. Indian J. Clin. Cardiol. 2020, 1, 13–16. [Google Scholar] [CrossRef]
- Zhang, X.; Shi, X.; Gao, P.; Wang, J.; Li, S.; Yao, S.; Zhang, X.; Huo, J.; Wang, J. Endovascular Management of May-Thurner Syndrome: A Case Report. Medicine 2016, 95, e2541. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.K.; Tseng, Y.H.; Lin, C.H.; Tsai, Y.H.; Hsu, Y.C.; Wang, S.C.; Chen, C.W. Evaluation of venous pathology of the lower extremities with triggered angiography non-contrast-enhanced magnetic resonance imaging. BMC Med. Imaging 2019, 19, 96. [Google Scholar] [CrossRef] [Green Version]
- Clifford, P.S. Local control of blood flow. Adv. Physiol. Educ. 2011, 35, 5–15. [Google Scholar] [CrossRef]
- Coffman, J.D.; Lempert, J.A. Venous flow velocity, venous volume and arterial blood flow. Circulation 1975, 52, 141–145. [Google Scholar] [CrossRef] [Green Version]
- Golub, A.S.; Pittman, R.N. A paradigm shift for local blood flow regulation. J. Appl. Physiol. 2014, 116, 703–705. [Google Scholar] [CrossRef] [Green Version]
- Kurstjens, R.L.; de Wolf, M.A.; Konijn, H.W.; Toonder, I.M.; Nelemans, P.J.; de Graaf, R.; Wittens, C.H. Intravenous pressure changes in patients with postthrombotic deep venous obstruction: Results using a treadmill stress test. J. Thromb. Haemost. 2016, 14, 1163–1170. [Google Scholar] [CrossRef] [Green Version]
- Kibbe, M.R.; Ujiki, M.; Goodwin, A.L.; Eskandari, M.; Yao, J.; Matsumura, J. Iliac vein compression in an asymptomatic patient population. J. Vasc. Surg. 2004, 39, 937–943. [Google Scholar] [CrossRef] [Green Version]
- Knuttinen, M.G.; Naidu, S.; Oklu, R.; Kriegshauser, S.; Eversman, W.; Rotellini, L.; Thorpe, P.E. May-Thurner: Diagnosis and endovascular management. Cardiovasc. Diagn. Ther. 2017, 7, S159–S164. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.W.; Yoon, C.J.; Jung, S.I.; Kim, H.C.; Lee, W.; Kim, Y.I.; Jae, H.J.; Park, J.H. Acute iliofemoral deep vein thrombosis: Evaluation of underlying anatomic abnormalities by spiral CT venography. J. Vasc. Interv. Radiol. 2004, 15, 249–256. [Google Scholar] [CrossRef]
- Fraser, D.G.W.; Moody, A.R.; Martel, A.; Morgan, P.S. Re-evaluation of iliac compression syndrome using magnetic resonance imaging in patients with acute deep venous thromboses. J. Vasc. Surg. 2004, 40, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Kaltenmeier, C.T.; Erben, Y.; Indes, J.; Lee, A.; Dardik, A.; Sarac, T.; Ochoa Chaar, C.I. Systematic review of May-Thurner syndrome with emphasis on gender differences. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 399–407.e4. [Google Scholar] [CrossRef]
- Peters, M.; Syed, R.K.; Katz, M.; Moscona, J.; Press, C.; Nijjar, V.; Bisharat, M.; Baldwin, D. May-Thurner syndrome: A not so uncommon cause of a common condition. Bayl. Univ. Med Cent. Proc. 2012, 25, 231–233. [Google Scholar] [CrossRef] [Green Version]
- May, R.; Thurner, J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology 1957, 8, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Mcmurrich, J.P. The occurrence of congenital adhesions in the common iliac veins and their relation to thrombosis of the femoral and iliac veins. Am. J. Med. Sci. 1908, 135, 342–346. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, W.; Al Safran, Z.; Hasan, H.; Zeid, W.A. Endovascular management of may-thurner syndrome. Ann. Vasc. Dis. 2012, 5, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.H.; Stookey, K.R.; Ketcham, D.B.; Cragg, A.H. Endovascular Management of Acute Extensive Iliofemoral Deep Venous Thrombosis Caused by May-Thurner Syndrome. J. Vasc. Interv. Radiol. 2000, 11, 1297–1302. [Google Scholar] [CrossRef]
- Hager, E.S.; Yuo, T.; Tahara, R.; Dillavou, E.; Al-Khoury, G.; Marone, L.; Makaroun, M.; Chaer, R.A. Outcomes of endovascular intervention for May-Thurner syndrome. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Hurst, D.R.; Forauer, A.R.; Bloom, J.R.; Greenfield, L.J.; Wakefield, T.W.; Williams, D.M. Diagnosis and endovascular treatment of iliocaval compression syndrome. J. Vasc. Surg. 2001, 34, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, T.; Spirk, D.; Engelberger, R.P.; Dopheide, J.F.; Baumann, F.A.; Barco, S.; Spescha, R.; Leeger, C.; Kucher, N. Incidence of Stent Thrombosis after Endovascular Treatment of Iliofemoral or Caval Veins in Patients with the Postthrombotic Syndrome. Thromb. Haemost. 2019, 119, 2064–2073. [Google Scholar] [CrossRef] [PubMed]
- Strijkers, R.H.; de Wolf, M.A.; Arnoldussen, C.W.; Timbergen, M.J.; de Graaf, R.; ten Cate-Hoek, A.J.; Wittens, C.H. Venous in-stent thrombosis treated by ultrasound accelerated catheter directed thrombolysis. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 440–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, J.P.; Holland, G.A.; Baum, R.A.; Owen, R.S.; Carpenter, J.T.; Cope, C. Magnetic resonance venography for the detection of deep venous thrombosis: Comparison with contrast venography and duplex Doppler ultrasonography. J. Vasc. Surg. 1993, 18, 734–741. [Google Scholar] [CrossRef]
- McDermott, S.; Oliveira, G.; Ergül, E.; Brazeau, N.; Wicky, S.; Oklu, R. May-Thurner syndrome: Can it be diagnosed by a single MR venography study? Diagn. Interv. Radiol. 2013, 19, 44–48. [Google Scholar] [CrossRef]
- Laissy, J.P.; Cinqualbre, A.; Loshkajian, A.; Henry-Feugeas, M.C.; Crestani, B.; Riquelme, C.; Schouman-Claeys, E. Assessment of deep venous thrombosis in the lower limbs and pelvis: MR venography versus duplex Doppler sonography. Am. J. Roentgenol. 1996, 167, 971–975. [Google Scholar] [CrossRef] [Green Version]
- Tamura, K.; Nakahara, H. MR Venography for the Assessment of Deep Vein Thrombosis in Lower Extremities with Varicose Veins. Ann. Vasc. Dis. 2014, 7, 399–403. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.W.; Tseng, Y.H.; Lin, C.C.; Kao, C.C.; Wong, M.Y.; Lin, B.S.; Huang, Y.K. Novel Diagnostic Options without Contrast Media or Radiation: Triggered Angiography Non-Contrast-Enhanced Sequence Magnetic Resonance Imaging in Treating Different Leg Venous Diseases. Diagnostics 2020, 10, 355. [Google Scholar] [CrossRef]
- Bammer, R.; Hope, T.A.; Aksoy, M.; Alley, M.T. Time-resolved 3D quantitative flow MRI of the major intracranial vessels: Initial experience and comparative evaluation at 1.5 T and 3.0 T in combination with parallel imaging. Magn. Reson. Med. 2007, 57, 127–140. [Google Scholar] [CrossRef] [Green Version]
- Bertelsen, L.; Vejlstrup, N.; Andreasen, L.; Olesen, M.S.; Svendsen, J.H. Cardiac magnetic resonance systematically overestimates mitral regurgitations by the indirect method. Open Heart 2020, 7, e001323. [Google Scholar] [CrossRef]
- Fučík, R.; Galabov, R.; Pauš, P.; Eichler, P.; Klinkovský, J.; Straka, R.; Tintěra, J.; Chabiniok, R. Investigation of phase-contrast magnetic resonance imaging underestimation of turbulent flow through the aortic valve phantom: Experimental and computational study using lattice Boltzmann method. Magma 2020, 33, 649–662. [Google Scholar] [CrossRef] [Green Version]
- Geurts, L.; Biessels, G.J.; Luijten, P.; Zwanenburg, J. Better and faster velocity pulsatility assessment in cerebral white matter perforating arteries with 7 T quantitative flow MRI through improved slice profile, acquisition scheme, and postprocessing. Magn. Reson. Med. 2018, 79, 1473–1482. [Google Scholar] [CrossRef] [Green Version]
- Kilner, P.J.; Gatehouse, P.D.; Firmin, D.N. Flow measurement by magnetic resonance: A unique asset worth optimising. J. Cardiovasc. Magn. Reson. 2007, 9, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Vuuren, T.M.A.J.; Kurstjens, R.; Wittens, C.; Laanen, J.; Graaf, R. Illusory Angiographic Signs of Significant Iliac Vein Compression in Healthy Volunteers. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 874–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamboni, P.; Franceschi, C.; Frate, R. The overtreatment of illusory May Thurner syndrome. Veins Lymphat. 2019, 8. [Google Scholar] [CrossRef]
- Zamboni, P.; Franceschi, C. How to Assess Illusory May-Thurner Syndrome by Ultrasound. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 305. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N = 51 |
|---|---|
| Age (yrs) | 62 (48, 74) |
| Sex, n (%) | |
| Male | 12 (23.5) |
| Female | 39 (76.5) |
| Comorbidities | |
| Hypertension, n (%) | 17 (33.3) |
| Diabetes mellitus, n (%) | 11 (21.6) |
| Hyperlipidemia, n (%) | 7 (13.7) |
| History of cerebrovascular accident, n (%) | 2 (3.9) |
| Chronic kidney disease, n (%) | 3 (5.9) |
| Coronary artery disease, n (%) | 2 (3.9) |
| Atrial fibrillation, n (%) | 2 (3.9) |
| Smoking, n (%) | |
| No | 44 (86.3) |
| Yes | 6 (11.8) |
| Quit | 1 (2.0) |
| Chronic lung disease, n (%) | 2 (3.9) |
| Symptom and sign | |
| Edema, n (%) | 18 (35.3) |
| Right, n (%) | 7 (13.7) |
| Left, n (%) | 8 (15.7) |
| Bilateral, n (%) | 3 (5.9) |
| Skin changes, n (%) | 9 (17.6) |
| Right, n (%) | 7 (13.7) |
| Left, n (%) | 1 (2.0) |
| Bilateral, n (%) | 1 (2.0) |
| Ulcer, n (%) | 10 (19.6) |
| Right, n (%) | 4 (7.8) |
| Left, n (%) | 6 (11.8) |
| Bilateral, n (%) | 0 (0) |
| Right Lower Extremity N = 19 | Left Lower Extremity N = 19 | p | |
|---|---|---|---|
| EIV | |||
| MF (mL/s) | 2.56 (2.15, 5.33) | 2.58 (1.56, 3.95) | 0.26 |
| MV (cm/s) | 7.96 (4.26, 9.92) | 6.51 (5.20, 10.63) | 0.60 |
| FV | |||
| MF (mL/s) | 1.00 (0.71, 1.61) | 1.06 (0.57, 1.41) | 0.73 |
| MV (cm/s) | 4.49 (2.97, 6.75) | 3.56 (2.78, 5.62) | 0.95 |
| PV | |||
| MF (mL/s) | 0.56 (0.34, 1.08) | 0.59 (0.35, 0.77) | 0.75 |
| MV (cm/s) | 2.21 (1.38, 4.08) | 2.27 (1.54, 3.09) | 0.53 |
| With Ipsilateral Symptoms N = 16 | Without Ipsilateral Symptoms N = 10 | |||||
|---|---|---|---|---|---|---|
| Non-Compression Side | Compression Side | p | Non-Compression Side | Compression Side | p | |
| EIV | ||||||
| MF (mL/s) | 2.49 (1.72, 3.02) | 2.37 (1.79, 4.58) | 0.67 | 2.79 (1.77, 4.00) | 1.67 (0.88, 1.90) | 0.04 |
| MV (cm/s) | 7.38 (5.08, 9.92) | 6.06 (5.30, 8.92) | 0.56 | 6.65 (3.54, 9.00) | 5.63 (2.84, 7.28) | 0.32 |
| FV | ||||||
| MF (mL/s) | 1.01 (0.72, 1.76) | 1.15 (0.56, 2.13) | 0.90 | 1.11 (0.95, 2.15) | 1.00 (0.54, 1.25) | 0.22 |
| MV (cm/s) | 4.34 (3.58, 6.71) | 4.26 (2.74, 8.62) | 0.93 | 5.12 (4.38, 6.86) | 4.47 (3.67, 5.93) | 0.28 |
| PV | ||||||
| MF (mL/s) | 0.72 (0.48, 1.04) | 0.68 (0.43, 1.22) | 0.99 | 0.51 (0.22, 1.39) | 0.52 (0.26, 0.68) | 0.73 |
| MV (cm/s) | 2.26 (1.53, 3.87) | 2.07 (1.45, 3.71) | 0.90 | 1.91 (1.08, 3.19) | 1.42 (1.03, 2.71) | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, Y.-H.; Chen, C.-W.; Wong, M.-Y.; Yang, T.-Y.; Lin, Y.-H.; Lin, B.-S.; Huang, Y.-K. Reduced External Iliac Venous Blood Flow Rate Is Associated with Asymptomatic Compression of the Common Iliac Veins. Medicina 2021, 57, 835. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080835
Tseng Y-H, Chen C-W, Wong M-Y, Yang T-Y, Lin Y-H, Lin B-S, Huang Y-K. Reduced External Iliac Venous Blood Flow Rate Is Associated with Asymptomatic Compression of the Common Iliac Veins. Medicina. 2021; 57(8):835. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080835
Chicago/Turabian StyleTseng, Yuan-Hsi, Chien-Wei Chen, Min-Yi Wong, Teng-Yao Yang, Yu-Hui Lin, Bor-Shyh Lin, and Yao-Kuang Huang. 2021. "Reduced External Iliac Venous Blood Flow Rate Is Associated with Asymptomatic Compression of the Common Iliac Veins" Medicina 57, no. 8: 835. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080835