
Epidemiological Surveillance of Eye Disease and People Awareness in the Abruzzo Region, Italy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
4.1. Main Findings
4.2. Comparisons with Existing Knowledge
4.3. Implications for Research and Clinical Practice
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sabanayagam, C.; Cheng, C.Y. Global causes of vision loss in 2015: Are we on track to achieve the Vision 2020 target? Lancet Glob. Health 2017, 5, e1164–e1165. [Google Scholar] [CrossRef] [Green Version]
- McCarty, C.A.; Nanjan, M.B.; Taylor, H.R. Vision impairment predicts 5 years mortality. Br. J. Ophthalmol 2001, 85, 322–326. [Google Scholar] [CrossRef]
- Ramrattan, R.S.; Wolfs, R.C.; Panda-Jonas, S.; Jonas, J.B.; Bakker, D.; Pols, H.A.; Hofman, A.; de Jong, P.T. Prevalence and causes of visual field loss in the elderly and associations with impairment in daily functioning: The Rotterdam Study. Arch. Ophthalmol. 2001, 119, 1788–1794. [Google Scholar] [CrossRef] [Green Version]
- Bourne, R.R.; Flaxman, S.R.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; Leasher, J.; Limburg, H.; et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e888–e897. [Google Scholar] [CrossRef] [Green Version]
- Flaxman, S.R.; Bourne, R.R.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.; Koch, R.G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. Available online: www.jstor.org/stable/2529310 (accessed on 12 June 2021). [CrossRef] [PubMed] [Green Version]
- Congdon, N.; O’Colmain, B.; Klaver, C.C.; Klein, R.; Muñoz, B.; Friedman, D.S.; Kempen, J.; Taylor, H.R.; Mitchell, P.; Eye Diseases Prevalence Research Group; et al. Causes and prevalence of visual impairment among adults in the United States. Arch. Ophthalmol. 2004, 122, 477–485. [Google Scholar]
- Furtado, J.M.; Lansingh, V.C.; Carter, M.J.; Milanese, M.F.; Peña, B.N.; Ghersi, H.A.; Bote, P.L.; Nano, M.E.; Silva, J.C. Causes of blindness and visual impairment in Latin America. Surv. Ophthalmol. 2012, 57, 149–177. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Wang, Y.; Li, Y.; Wang, Y.; Cui, T.; Li, J.; Jonas, J.B. Causes of blindness and visual impairment in urban and rural areas in Beijing: The Beijing Eye Study. Ophthalmology 2006, 113, 1134.e1–1134.e11. [Google Scholar] [CrossRef]
- Taylor, H.R.; Keeffe, J.E.; Vu, H.T.; Wang, J.J.; Rochtchina, E.; Mitchell, P.; Pezzullo, M.L. Vision loss in Australia. Med. J. Aust. 2005, 182, 565–568. [Google Scholar] [CrossRef]
- Cedrone, C.; Nucci, C.; Scuderi, G.; Ricci, F.; Cerulli, A.; Culasso, F. Prevalence of blindness and low vision in an Italian population: A comparison with other European studies. Eye (Lond.) 2006, 20, 661–667. [Google Scholar] [CrossRef] [Green Version]
- Piermarocchi, S.; Segato, T.; Scopa, P.; Masetto, M.; Ceca, S.; Cavarzeran, F.; Peto, T.; PAMDI Study Group. The prevalence of age-related macular degeneration in Italy (PAMDI) study: Report 1. Ophthalmic Epidemiol. 2011, 18, 129–136. [Google Scholar] [CrossRef]
- Haddad, M.F.; Bakkar, M.M.; Abdo, N. Public awareness of common eye diseases in Jordan. BMC Ophthalmol. 2017, 17, 177. [Google Scholar] [CrossRef] [Green Version]
- Dandona, R.; Dandona, L.; John, R.K.; McCarty, C.A.; Rao, G.N. Awareness of eye diseases in an urban population in southern India. Bull. World Health Organ. 2001, 79, 96–102. [Google Scholar]
- Shrestha, M.K.; Guo, C.W.; Maharjan, N.; Gurung, R.; Ruit, S. Health literacy of common ocular diseases in Nepal. BMC Ophthalmol. 2014, 14, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attebo, K.; Mitchell, P.; Cumming, R.; BMath, W.S. Knowledge and beliefs about common eye diseases. Aust. N. Z. J. Ophthalmol. 1997, 25, 283–287. [Google Scholar] [CrossRef]
- Chew, Y.K.; Reddy, S.C.; Karina, R. Awareness and knowledge of common eye diseases among the academic staff (non-medical faculties) of University of Malaya. Med. J. Malays. 2004, 59, 305–311. [Google Scholar]
- Noertjojo, K.; Maberley, D.; Bassett, K.; Courtright, P. Awareness of eye diseases and risk factors: Identifying needs for health education and promotion in Canada. Can. J. Ophthalmol. 2006, 41, 617–623. [Google Scholar] [CrossRef]
- Sathyamangalam, R.V.; Paul, P.G.; George, R.; Baskaran, M.; Hemamalini, A.; Madan, R.V.; Augustian, J.; Prema, R.; Lingam, V. Determinants of glaucoma awareness and knowledge in urban Chennai. Indian J. Ophthalmol. 2009, 57, 355–360. [Google Scholar] [PubMed]
- Vijaya, L.; George, R.; Arvind, H.; Baskaran, M.; Ramesh, S.V.; Raju, P.; Kumaramanickavel, G.; McCarty, C. Prevalence of primary angle-closure disease in an urban south Indian population and comparison with a rural population. The Chennai Glaucoma Study. Ophthalmology 2008, 115, 655–660.e1. [Google Scholar] [CrossRef] [PubMed]
- Vijaya, L.; George, R.; Baskaran, M.; Arvind, H.; Raju, P.; Ramesh, S.V.; Kumaramanickavel, G.; McCarty, C. Prevalence of primary open-angle glaucoma in an urban south Indian population and comparison with a rural population. The Chennai Glaucoma Study. Ophthalmology 2008, 115, 648–654.e1. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.R.; Jonas, J.B.; Bron, A.M.; Cicinelli, M.V.; Das, A.; Flaxman, S.R.; Friedman, D.S.; Keeffe, J.E.; Kempen, J.H.; Leasher, J.; et al. Prevalence and causes of vision loss in high-income countries and in Eastern and Central Europe in 2015: Magnitude, temporal trends and projections. Br. J. Ophthalmol. 2018, 102, 575–585. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n with Available Data | Mean and Standard Deviation or Frequency and Proportions | |
|---|---|---|
| n | 983 | |
| Socio-demographic characteristics | ||
| Men (%) | 983 | 451 (45.9) |
| Mean age (years) | 983 | 66.0 ± 9.5 |
| Age in classes (%): | 983 | |
| <65 years | 438 (44.6) | |
| ≥65 years | 545 (55.4) | |
| School education (%): | 983 | |
| <5 years | 62 (6.3) | |
| Primary school | 271 (27.6) | |
| Secondary school | 312 (31.7) | |
| High school | 280 (28.5) | |
| University degree | 58 (5.9) | |
| Civil status (%) | 983 | |
| Married/Partner | 851 (86.6) | |
| Single/Divorced/Widow | 132 (13.4) | |
| Working status (%) | 983 | |
| Employed | 230 (23.4) | |
| Unemployed/retired | 753 (76.6) | |
| Lifestyle | ||
| Physical activity (%) | 983 | |
| Regular | 95 (9.7) | |
| Occasional | 108 (11.0) | |
| Never | 780 (79.3) | |
| Alcohol consumption (%) | 983 | |
| Regular | 411 (41.8) | |
| Occasional | 107 (10.9) | |
| Never | 465 (47.3) | |
| Smoking (%) | 983 | |
| Yes | 152 (15.5) | |
| Ex | 273 (27.8) | |
| No | 558 (56.8) | |
| If yes, no. of cigarettes/day (%) | 145 | |
| ≤10 | 88 (60.7) | |
| 11–20 | 48 (33.1) | |
| >20 | 9 (6.2) | |
| If ex, date of cessation (%) | 273 | |
| <10 years | 28 (10.3) | |
| >10 years | 56 (20.5) | |
| >20 years | 64 (23.4) | |
| >30 years | 77 (28.2) | |
| >40 years | 40 (14.7) | |
| Unknown | 8 (2.9) | |
| Daily exposition to ultraviolet rays (%) | 982 | |
| None | 4 (0.4) | |
| Low (1–2 h/day) | 230 (23.4) | |
| Intermediate (2–3 h/day) | 320 (32.6) | |
| High (>3 h/day) | 428 (43.6) | |
| Clinical characteristics | ||
| Mean BMI (kg/m2) | 972 | 26.6 ± 4.1 |
| BMI in classes (%): | 972 | |
| Underweight | 11 (1.1) | |
| Normal weight | 346 (35.7) | |
| Overweight | 430 (44.4) | |
| Obesity | 181 (18.7) | |
| Type 2 diabetes (%) | 983 | 130 (13.2) |
| Hypertension (%) | 983 | 411 (41.8) |
| Cardiovascular diseases (%) | 983 | 119 (12.1) |
| Neurologic diseases (%) | 983 | 26 (2.6) |
| Renal diseases (%) | 983 | 50 (5.1) |
| Rheumatological diseases (%) | 983 | 234 (23.8) |
| Attention to the own health status | ||
| Do you check regularly your health status? (%) | 983 | |
| Yes | 767 (78.0) | |
| Sometimes/only in case of problems | 198 (20.1) | |
| Never | 18 (1.8) | |
| How would you define your health? (%) | 982 | |
| Excellent | 109 (11.1) | |
| Good | 724 (73.7) | |
| Intermediate | 142 (14.5) | |
| Poor | 7 (0.7) | |
| Frequency of eye examination (%) | 983 | |
| More than once a year | 75 (7.6) | |
| Once a year | 305 (31.0) | |
| Every 2 years | 219 (22.3) | |
| Occasionally | 384 (39.1) |
| Eye Examination | n with Available Data | Mean and Standard Deviation or Frequency and Proportions |
|---|---|---|
| n | 983 | |
| Visual perception (%) | ||
| See well with or without glasses (20/20 snellen visual acuity) | 983 | 550 (56.0) |
| Low vision (best corrected or uncorrected) | 983 | 32 (3.3) |
| Refractive error (%) | 983 | |
| Myopia (>−0.25 sph) | 96 (9.8) | |
| Hyperopia (>+0.25 sph) | 313 (31.8) | |
| Astigmatism (±0.25 cyl) | 435 (44.3) | |
| None | 139 (14.1) | |
| AMSLER grid: presence of (%) | 965 | |
| Metamorphopsia | 63 (6.5) | |
| Scotoma | 2 (0.2) | |
| Scotoma and metamorphopsia | 2 (0.2) | |
| None | 898 (93.1) | |
| Discromatopsia (Ishihara test) (%) | 971 | 38 (3.9) |
| Strabismus (Cover–uncover test) (%) | 954 | 46 (4.8) |
| Corneal disorder (%) | 919 | 5 (0.5) |
| Mean tone (mmHg) | 977 | 14.7 ± 3.2 |
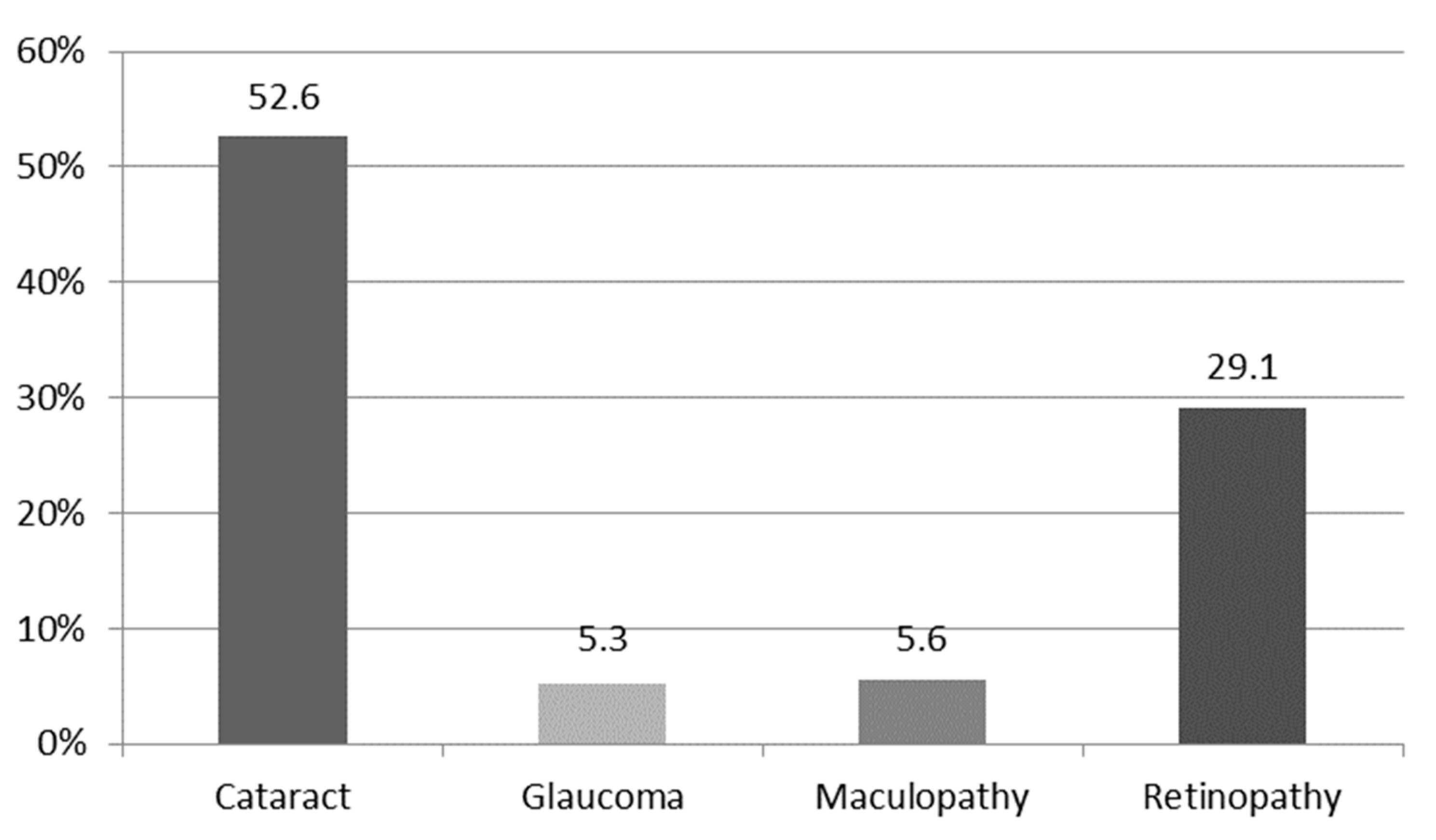
| Cataract (%) | 916 | 482 (52.6) |
| History of surgical treatment for cataract (%) | 186 | 97 (52.2) |
| Satisfaction with surgical treatment for cataract (%) | 97 | |
| Very satisfied | 9 (9.3) | |
| Satisfied | 83 (85.6) | |
| Partly satisfied | 5 (5.2) | |
| Glaucoma-related optic nerve head alterations (%) | 981 | 52 (5.3) |
| Advanced Age-Related Macular Degeneration (AMD)/maculopathy (%) | 480 | 27 (5.6) |
| Vascular eye diseases (diabetic retinopathy, hypertensive retinopathy, occlusive vasculopathies)/retinopathy (%) | 474 | 138 (29.1) |
| Aware | Not Aware | p-Value * | |
|---|---|---|---|
| n | 105 | 377 | |
| Socio-demographic characteristics | |||
| Men (%) | 42 (40.0) | 172 (45.6) | 0.30 |
| Mean age (years) | 73.0 ± 6.8 | 67.0 ± 8.4 | <0.0001 |
| School education (%) | |||
| <Secondary school | 61 (58.1) | 128 (33.9) | 0.0005 |
| ≥Secondary school | 44 (41.9) | 249 (66.1) | |
| Civil status: | |||
| Married/Partner | 78 (74.3) | 333 (88.3) | 0.0003 |
| Single/Divorced/Widow | 27 (25.7) | 44 (11.7) | |
| Working status (%) | |||
| Retired | 88 (83.8) | 245 (65.0) | <0.0001 |
| Employed | 17 (16.2) | 132 (35.0) | |
| Lifestyle | |||
| Physical activity (%) | |||
| Regular | 3 (2.9) | 28 (7.4) | 0.16 |
| Sometimes | 9 (8.6) | 42 (11.1) | |
| Never | 93 (88.6) | 307 (81.4) | |
| Alcohol consumption (%) | |||
| Regular | 37 (35.2) | 160 (42.4) | 0.15 |
| Sometimes | 9 (8.6) | 45 (11.9) | |
| Never | 59 (56.2) | 172 (45.6) | |
| Smoking (%) | |||
| Yes | 10 (9.5) | 62 (16.4) | 0.18 |
| Ex | 29 (27.6) | 106 (28.1) | |
| No | 66 (62.9) | 209 (55.4) | |
| Clinical characteristics | |||
| Mean BMI (kg/m2) | 27.1 ± 4.7 | 26.7 ± 4.0 | 0.95 |
| BMI in classes (%): | |||
| Underweight | 0 (0.0) | 4 (1.1) | 0.78 |
| Normal weight | 37 (36.3) | 123 (33.2) | |
| Overweight | 43 (42.2) | 170 (45.8) | |
| Obesity | 22 (21.6) | 74 (19.9) | |
| Type 2 diabetes (%) | 16 (15.2) | 60 (15.9) | 0.87 |
| Hypertension (%) | 62 (59.0) | 158 (41.9) | 0.002 |
| Cardiovascular diseases (%) | 19 (18.1) | 45 (11.9) | 0.10 |
| Neurologic diseases (%) | 2 (1.9) | 11 (2.9) | 0.74 |
| Renal diseases (%) | 8 (7.6) | 25 (6.6) | 0.72 |
| Rheumatological diseases (%) | 27 (25.7) | 106 (28.1) | 0.63 |
| Attention to the own health status | |||
| Do you check regularly your health status? (%) | |||
| Yes | 85 (81.0) | 299 (79.3) | 0.37 |
| Sometimes/only in case of problem | 20 (19.0) | 71 (18.8) | |
| Never | 0 (0.0) | 7 (1.9) | |
| How would you define your health? (%) | |||
| Excellent | 2 (1.9) | 34 (9.0) | 0.003 |
| Good | 76 (72.4) | 286 (76.1) | |
| Intermediate | 26 (24.8) | 55 (14.6) | |
| Poor | 1 (1.0) | 1 (0.3) | |
| Frequency of eye examination (%) | |||
| More than once a year | 9 (8.6) | 26 (6.9) | 0.21 |
| Once a year | 39 (37.1) | 104 (27.6) | |
| Every 2 years | 22 (21.0) | 91 (24.1) | |
| Occasionally | 35 (33.3) | 156 (41.4) | |
| Other eye disease | |||
| Glaucoma (%) | 8 (7.6) | 8 (2.1) | 0.01 |
| Maculopathy (%) | 3 (2.9) | 5 (1.3) | 0.38 |
| Retinopathy (%) | 1 (1.0) | 0 (0.0) | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastropasqua, L.; D’Aloisio, R.; Mastrocola, A.; Perna, F.; Cerino, L.; Cerbara, L.; Cruciani, F.; Toto, L. Epidemiological Surveillance of Eye Disease and People Awareness in the Abruzzo Region, Italy. Medicina 2021, 57, 978. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090978
Mastropasqua L, D’Aloisio R, Mastrocola A, Perna F, Cerino L, Cerbara L, Cruciani F, Toto L. Epidemiological Surveillance of Eye Disease and People Awareness in the Abruzzo Region, Italy. Medicina. 2021; 57(9):978. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090978
Chicago/Turabian StyleMastropasqua, Leonardo, Rossella D’Aloisio, Alessandra Mastrocola, Fabiana Perna, Luca Cerino, Loredana Cerbara, Filippo Cruciani, and Lisa Toto. 2021. "Epidemiological Surveillance of Eye Disease and People Awareness in the Abruzzo Region, Italy" Medicina 57, no. 9: 978. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090978