
Orthopedic Surgeons’ Views of Hyaluronic Acid Formulations in the Management of Knee Osteoarthritis: A Questionnaire-Based Cross-Sectional Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Ethical Approval of the Study
2.2. Study Design and Population
2.3. Questionnaire Development
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A
- 1.
- Your age:
- ☐
- 30–34 years
- ☐
- 35–44 years
- ☐
- 45–55 years
- ☐
- >55 years
- 2.
- Gender:
- ☐
- Male
- ☐
- Female
- 3.
- Which country are you practicing in?
- ☐
- Saudi Arabia
- ☐
- Jordan
- 4.
- Where did you receive your postgraduate training?
- ☐
- Middle East (e.g., Saudi Arabia, Jordan, Egypt, Syria, Bahrain)
- ☐
- North America (e.g., United States, Canada)
- ☐
- Western Europe (e.g., Germany, France, United Kingdom)
- ☐
- Others: ________________________
- 5.
- How many years of experience do you have in orthopedic practice?
- 1–5 years
- 5–10 years
- >10 years
- 6.
- Where do you primarily practice?
- Public/government healthcare institutions
- Private clinics or hospitals
- 7.
- Do you use hyaluronic acid injections in the management of patients with osteoarthritis?☐ Yes ☐ No
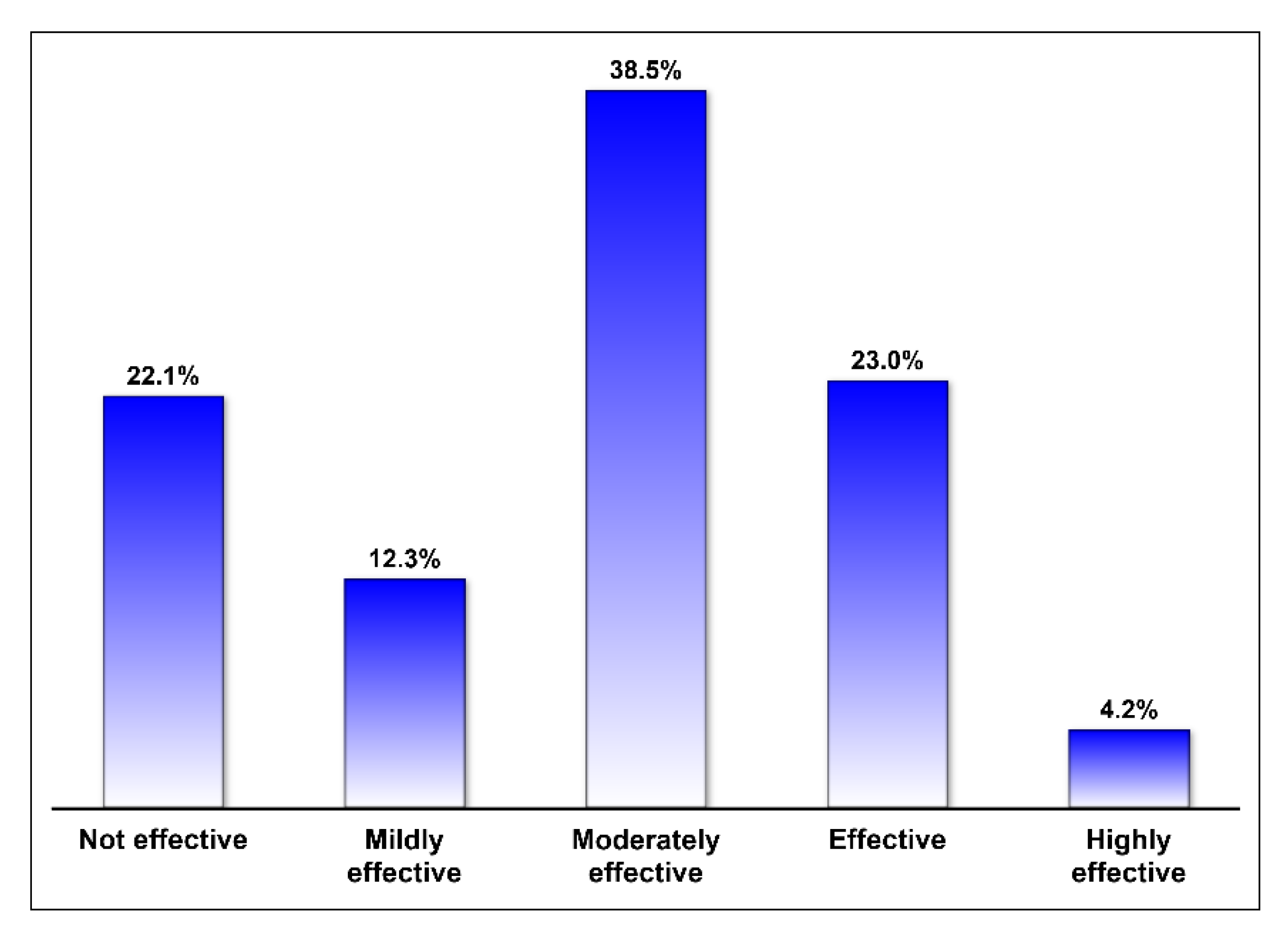
- 8.
- Please rate the efficacy of hyaluronic acid injections in the management of osteoarthritis:☐ Not effective ☐ Mildly effective ☐ Moderately effective☐ Effective ☐ Highly effective
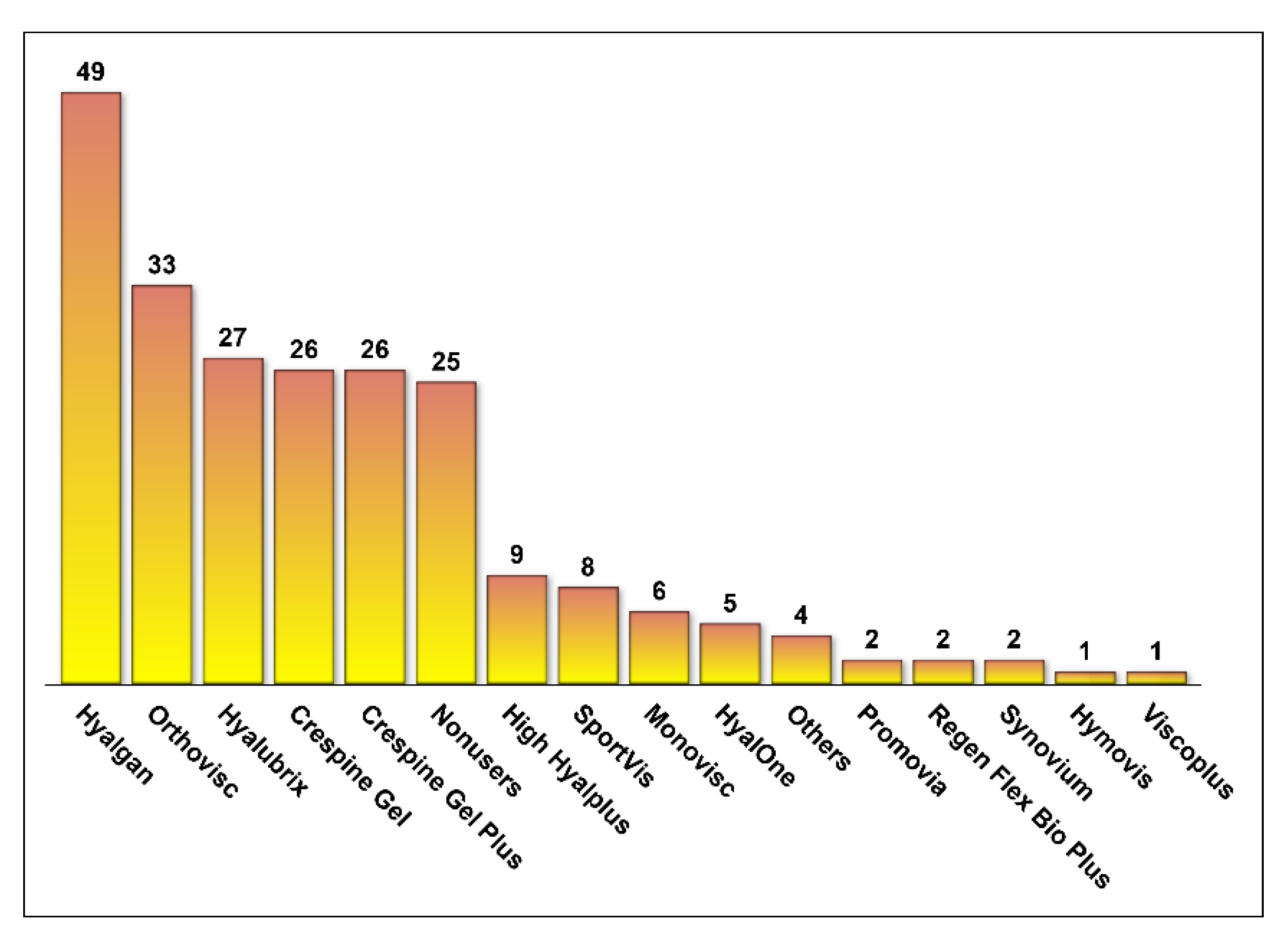
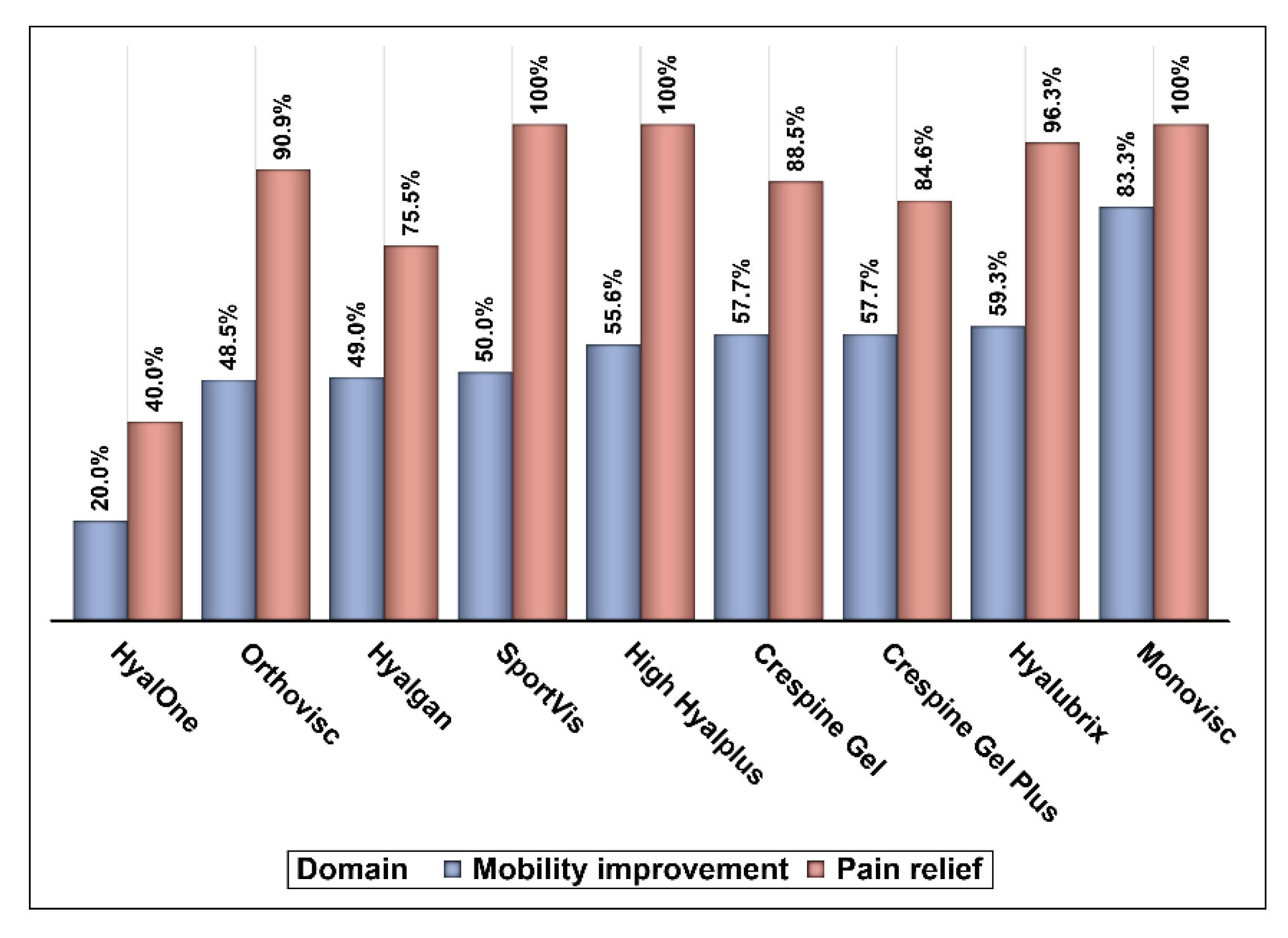
- 9.
- The following are some examples of hyaluronic acid injections that are used in the management of osteoarthritis. Please let us know whether you are using any of them by checking the box and let us know whether the hyaluronic acid products that you are using improve mobility and/or relieve pain by checking the appropriate boxes. Please note that you can check multiple boxes.
- ☐
- HyalOne®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Orthovisc®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Hyalgan®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- SportVis®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- High Hyalplus®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Crespine Gel®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Crespine Gel Plus®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Hyalubrix®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Monovisc®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Hymovis®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Viscoplus®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Synovium®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Regen Flex Bio Plus®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Promovia®
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
- ☐
- Others: _____________________
- Does it improve patient mobility?☐ Yes ☐ No
- Does it relieve pain?☐ Yes ☐ No
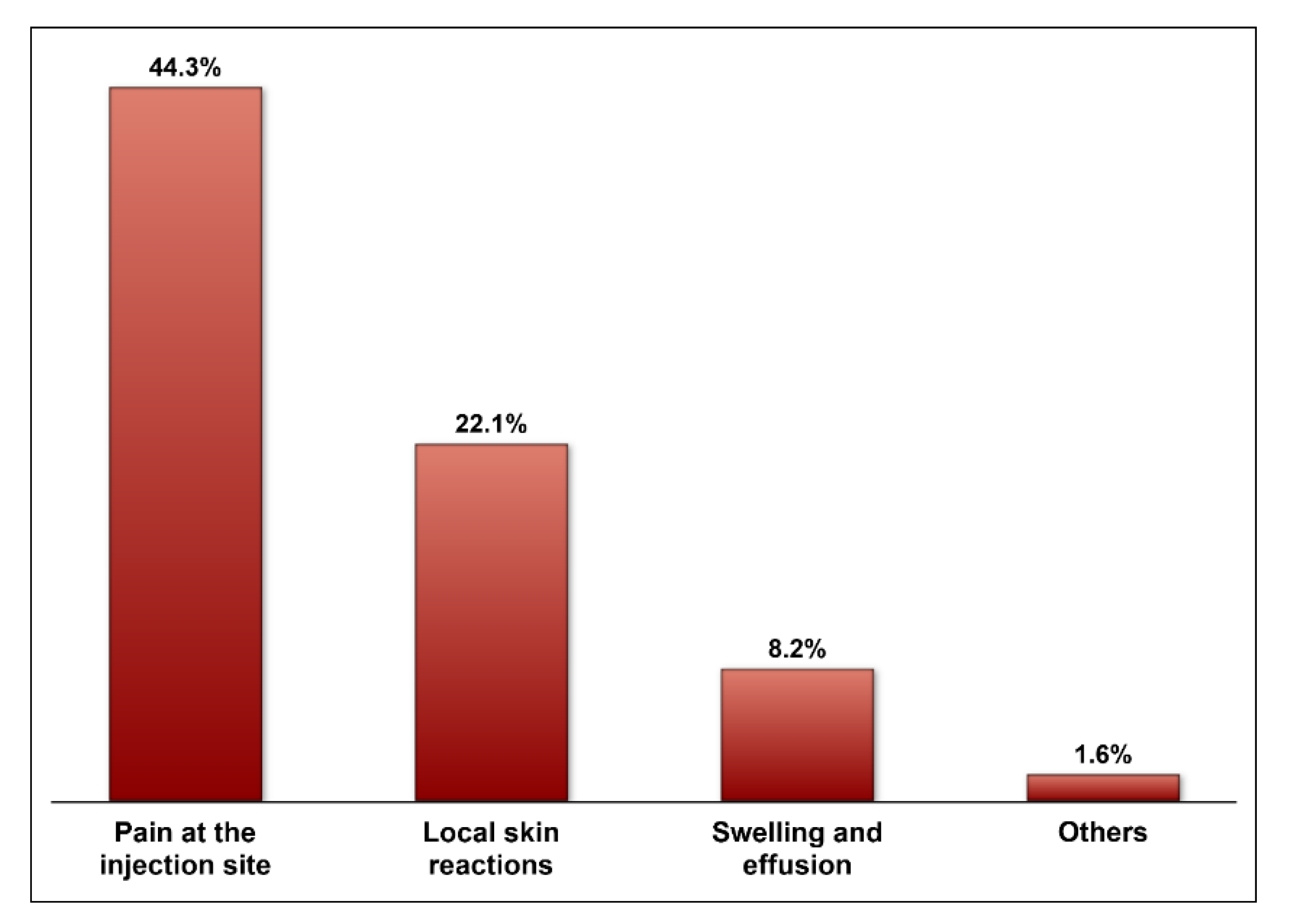
- 10.
- Which of the following side effects have you noticed in patients treated with hyaluronic acid injections for osteoarthritis?
- ☐
- Pain at the injection site
- ☐
- Swelling and effusion
- ☐
- Local skin reactions (rash, ecchymosis)
- ☐
- Others: _______________________________________________
References
- Walker, K.; Basehore, B.M.; Goyal, A.; Bansal, P.; Zito, P.M. Hyaluronic Acid; StatPearls: online publisher, 2020. [Google Scholar]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Roth, M.; Karakiulakis, G. Hyaluronic acid: A key molecule in skin aging. Dermato-Endocrinology 2012, 4, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Huynh, A.; Priefer, R. Hyaluronic acid applications in ophthalmology, rheumatology, and dermatology. Carbohydr. Res. 2020, 489, 107950. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.F.; Ruano-Ravina, A. Efficacy and safety of intraarticular hyaluronic acid in the treatment of hip osteoarthritis: A systematic review. Osteoarthr. Cartil. 2006, 14, 1306–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29, 100587. [Google Scholar] [CrossRef]
- AlKuwaity, K.W.; Mohammad, T.N.; Hussain, M.A.; Alkhanani, A.J.; Ali, A.M.B. Prevalence and determinant factors of osteoarthritis of the knee joint among elderly in Arar, KSA. Egypt. J. Hosp. Med. 2018, 72, 5173–5177. [Google Scholar] [CrossRef]
- Mukharrib, M.S.; Al-Sharif, M.N.; Alshehri, T.K.; Shaker, A. Knowledge of knee osteoarthritis among general population in Aseer region. J. Fam. Med. Prim. Care 2018, 7, 1385. [Google Scholar] [CrossRef]
- Maheu, E.; Rannou, F.; Reginster, J.Y. Efficacy and safety of hyaluronic acid in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Semin. Arthritis Rheum. 2016, 45 (Suppl. 4), S28–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sze, J.H.; Brownlie, J.C.; Love, C.A. Biotechnological production of hyaluronic acid: A mini review. 3 Biotech 2016, 6, 67. [Google Scholar] [CrossRef] [Green Version]
- Fallacara, A.; Baldini, E.; Manfredini, S.; Vertuani, S. Hyaluronic Acid in the Third Millennium. Polymers 2018, 10, 701. [Google Scholar] [CrossRef] [Green Version]
- Nicholls, M.; Manjoo, A.; Shaw, P.; Niazi, F.; Rosen, J. A Comparison Between Rheological Properties of Intra-articular Hyaluronic Acid Preparations and Reported Human Synovial Fluid. Adv Ther. 2018, 35, 523–530. [Google Scholar] [CrossRef] [Green Version]
- van der Weegen, W.; Wullems, J.A.; Bos, E.; Noten, H.; van Drumpt, R.A. No difference between intra-articular injection of hyaluronic acid and placebo for mild to moderate knee osteoarthritis: A randomized, controlled, double-blind trial. J. Arthroplast. 2015, 30, 754–757. [Google Scholar] [CrossRef] [PubMed]
- Concoff, A.; Sancheti, P.; Niazi, F.; Shaw, P.; Rosen, J. The efficacy of multiple versus single hyaluronic acid injections: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lana, J.F.S.D.; Weglein, A.; Sampson, S.E.; Vicente, E.F.; Huber, S.C.; Souza, C.V.; Ambach, M.A.; Vincent, H.; Urban-Paffaro, A.; Onodera, C.M.K.; et al. Randomized controlled trial comparing hyaluronic acid, platelet-rich plasma and the combination of both in the treatment of mild and moderate osteoarthritis of the knee. J. Stem Cells Regen. Med. 2016, 12, 69. [Google Scholar] [PubMed]
- He, W.-w.; Kuang, M.-j.; Zhao, J.; Sun, L.; Lu, B.; Wang, J.; Ma, J.-x.; Ma, X.-l. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. Int. J. Surg. 2017, 39, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Bashaireh, K.; Naser, Z.; Al Hawadya, K.; Sorour, S.; Al-Khateeb, R.N. Efficacy and safety of cross-linked hyaluronic acid single injection on osteoarthritis of the knee: A post-marketing Phase IV study. Drug Des. Dev. Ther. 2015, 9, 2063. [Google Scholar] [CrossRef] [Green Version]
- Trigkilidas, D.; Anand, A. The effectiveness of hyaluronic acid intra-articular injections in managing osteoarthritic knee pain. Ann. R. Coll. Surg. Engl. 2013, 95, 545–551. [Google Scholar] [CrossRef]
- Salmon, J.-H.; Rat, A.-C.; Charlot-Lambrecht, I.; Eschard, J.-P.; Jolly, D.; Fautrel, B. Cost effectiveness of intra-articular hyaluronic acid and disease-modifying drugs in knee osteoarthritis. PharmacoEconomics 2018, 36, 1321–1331. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Dasa, V.; DeKoven, M.; Sun, K.; Scott, A.; Lim, S. Clinical and cost outcomes from different hyaluronic acid treatments in patients with knee osteoarthritis: Evidence from a US health plan claims database. Drugs Context 2016, 5, 212296. [Google Scholar] [CrossRef]
- Bhandari, M.; Bannuru, R.R.; Babins, E.M.; Martel-Pelletier, J.; Khan, M.; Raynauld, J.-P.; Frankovich, R.; Mcleod, D.; Devji, T.; Phillips, M.; et al. Intra-articular hyaluronic acid in the treatment of knee osteoarthritis: A Canadian evidence-based perspective. Ther. Adv. Musculoskelet. Dis. 2017, 9, 231–246. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.A. AAOS clinical practice guideline: Treatment of osteoarthritis of the knee: Evidence-based guideline. JAAOS-J. Am. Acad. Orthop. Surg. 2013, 21, 577–579. [Google Scholar]
- Cucurnia, I.; Pudda, A.; Madonna, V.; Berruto, M.; Zaffagnini, S. Patient-reported outcomes of intra-articular hyaluronic acid for osteoarthritis of the knee: A prospective and multicentric case series. Musculoskelet. Surg. 2021, 1–8. [Google Scholar] [CrossRef]
- Gusho, C.A.; Jenson, M. Patient-reported outcomes of short-term intra-articular hyaluronic acid for osteoarthritis of the knee: A consecutive case series. Cureus 2019, 11, e4972. [Google Scholar] [CrossRef] [Green Version]
- Mochizuki, T.; Ikari, K.; Yano, K.; Okazaki, K. Comparison of patient-reported outcomes of treatment with low-and intermediate molecular weight hyaluronic acid in Japanese patients with symptomatic knee osteoarthritis: A prospective, randomized, single-blind trial. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2020, 21, 22–26. [Google Scholar] [CrossRef]
- Qiu, Y.; Ma, Y.; Huang, Y.; Li, S.; Xu, H.; Su, E. Current advances in the biosynthesis of hyaluronic acid with variable molecular weights. Carbohydr. Polym. 2021, 269, 118320. [Google Scholar] [CrossRef]
- Vázquez-Morales, E.; Verdugo-Meza, R.; Godínez-Alvarado, M.; Chávez-Covarrubias, G. Efficacy of viscosupplementation with high and medium molecular weight hyaluronic acid in patients with symptomatic gonarthrosis grades II-III. Acta Ortopedica Mexicana 2019, 33, 166–168. [Google Scholar]
- Webner, D.; Huang, Y.; Hummer, C.D., III. Intraarticular Hyaluronic Acid Preparations for Knee Osteoarthritis: Are Some Better Than Others? Cartilage 2021. [Google Scholar] [CrossRef] [PubMed]
- Migliore, A.; Paoletta, M.; Moretti, A.; Liguori, S.; Iolascon, G. The perspectives of intra-articular therapy in the management of osteoarthritis. Expert Opin. Drug Deliv. 2020, 17, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Bloom, J.E.; Rischin, A.; Johnston, R.V.; Buchbinder, R. Image-guided versus blind glucocorticoid injection for shoulder pain. Cochrane Database Syst. Rev. 2012, 15, CD009147. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.A. Mail and Internet surveys: The Tailored Design Method-2007 Update with New Internet, Visual, and Mixed-Mode Guide; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Country | |
| Saudi Arabia | 73 (59.84) |
| Jordan | 49 (40.16) |
| Age | |
| 30–34 years | 16 (13.11) |
| 35–44 years | 51 (41.80) |
| 45–55 years | 32 (26.23) |
| >55 years | 23 (18.85) |
| Years of experience | |
| 1–5 | 13 (10.66) |
| 5–10 | 25 (20.49 |
| >10 | 84 (68.85) |
| Gender | |
| Male | 120 (98.36) |
| Female | 2 (1.64) |
| Postgraduate training | |
| North America (e.g., United States, Canada) | 17 (13.93) |
| Europe (e.g., France, Germany, United Kingdom) | 22 (18.03) |
| Middle East (e.g., Saudi Arabia, Jordan, Egypt, Syria, Bahrain) | 83 (68.03) |
| Type of practice | |
| Public | 80 (65.57) |
| Private | 42 (34.43) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnasser, S.; AlHussain, F.; Asiri, H.; Almutairi, A.; Alsanawi, H.; Altamimi, A.A.; Asiri, Y.A.; Almohammed, O.A.; AlRuthia, Y. Orthopedic Surgeons’ Views of Hyaluronic Acid Formulations in the Management of Knee Osteoarthritis: A Questionnaire-Based Cross-Sectional Study. Medicina 2021, 57, 990. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090990
Alnasser S, AlHussain F, Asiri H, Almutairi A, Alsanawi H, Altamimi AA, Asiri YA, Almohammed OA, AlRuthia Y. Orthopedic Surgeons’ Views of Hyaluronic Acid Formulations in the Management of Knee Osteoarthritis: A Questionnaire-Based Cross-Sectional Study. Medicina. 2021; 57(9):990. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090990
Chicago/Turabian StyleAlnasser, Shahd, Fatima AlHussain, Hassan Asiri, Abdullah Almutairi, Hisham Alsanawi, Anas AR Altamimi, Yousif A. Asiri, Omar A. Almohammed, and Yazed AlRuthia. 2021. "Orthopedic Surgeons’ Views of Hyaluronic Acid Formulations in the Management of Knee Osteoarthritis: A Questionnaire-Based Cross-Sectional Study" Medicina 57, no. 9: 990. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090990