
Individually Tailored Remote Physiotherapy Program Improves Participation and Autonomy in Activities of Everyday Life along with Exercise Capacity, Self-Efficacy, and Low-Moderate Physical Activity in Patients with Pulmonary Arterial Hypertension: A Randomized Controlled Study


Abstract
:1. Introduction
2. Materials and Methods
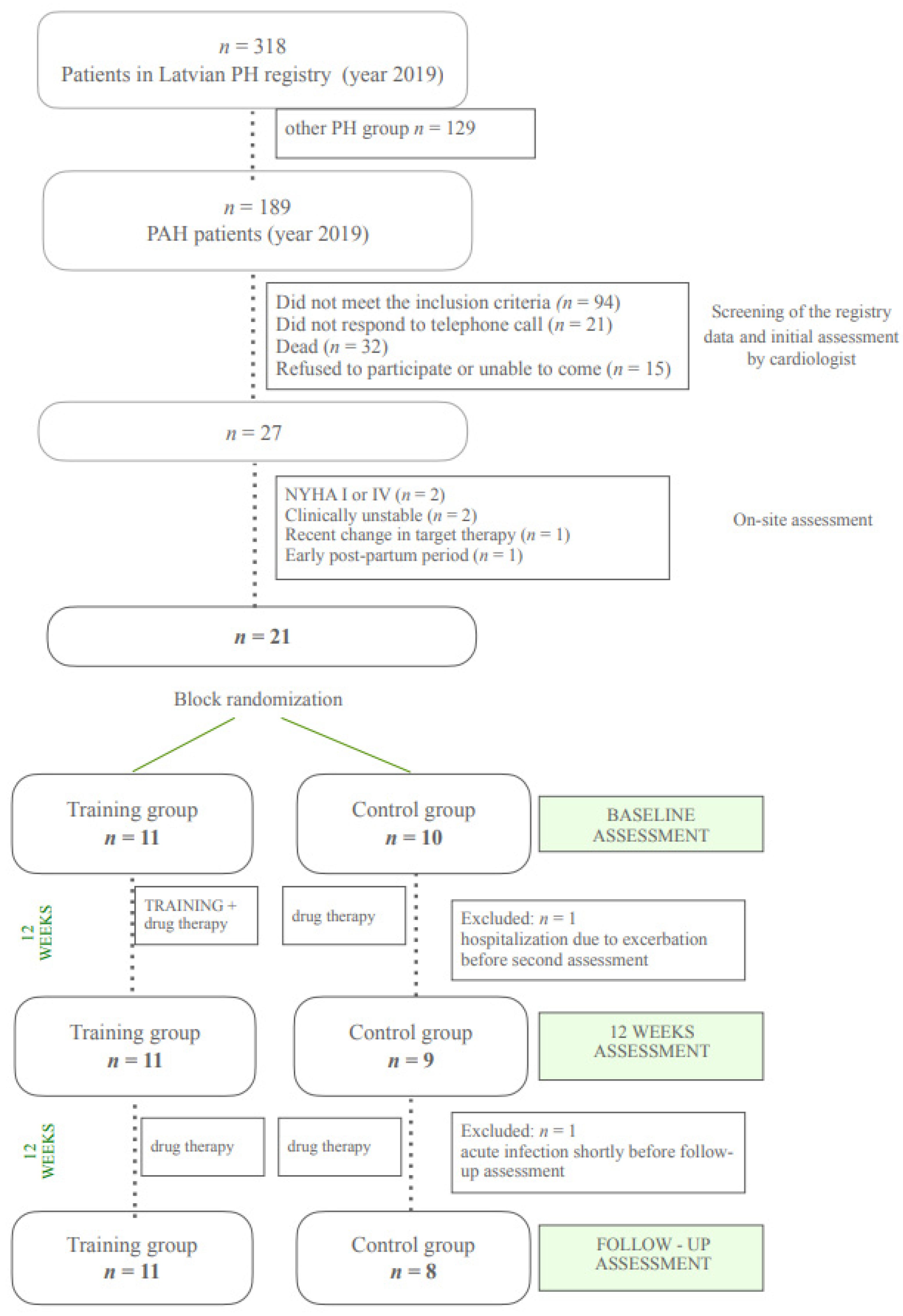
2.1. Study Population
2.2. Study Protocol
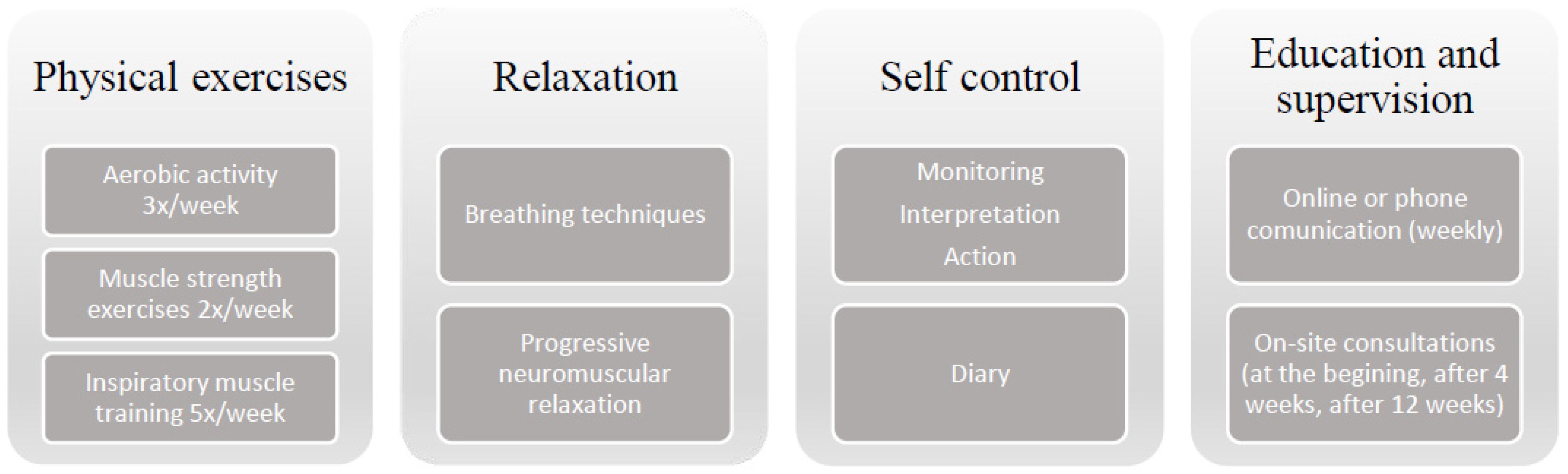
2.3. Intervention
- (I)
- Aerobic activity: 20 to 40 min of cyclic activity, three times a week. The type of activity was selected individually (e.g., walking, bicycle ergometer). Intensity: perceived exertion as 5–6 on the 10 point Borg scale and sustained SpO2 or a decrease of no more than 5% from baseline. Progression was based on individual tolerability and was provided by an increase in training duration and limited by ‘alarm signs’: maximum heart rate of more than 120 bpm, decrease in SpO2 to 85%; perceived exertion as very hard (>6 on the Borg scale) and subjective symptoms of exercise intolerance (severe dyspnea or fatigue, dizziness, pain, etc.).
- (II)
- Strength training: five to six resistance exercises (involving upper or lower limbs) with 5 to 10 repetitions in each set, twice a week; performed using the person’s own body weight or low weights (dumbbells or water bottles (0.5–1 kg)).
- (III)
- Inspiratory muscle training: with PHILIPS Threshold IMT breathing trainer, five times a week. Progression: repetitions from 3 × 3 to 3 × 7 in each set; resistance from 30% to 65–70% from max.
- (IV)
- Relaxation: five times a week. Includes breathing techniques (diaphragmatic breathing; slow breathing; pursed lip breathing; breathing pattern perception and awareness) and elements of progressive neuromuscular relaxation and body awareness.
2.4. Outcome Measures
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
2.5. Data Analysis
3. Results
3.1. Characteristics of the Participants at Baseline
3.2. Adherence and Adverse Effects
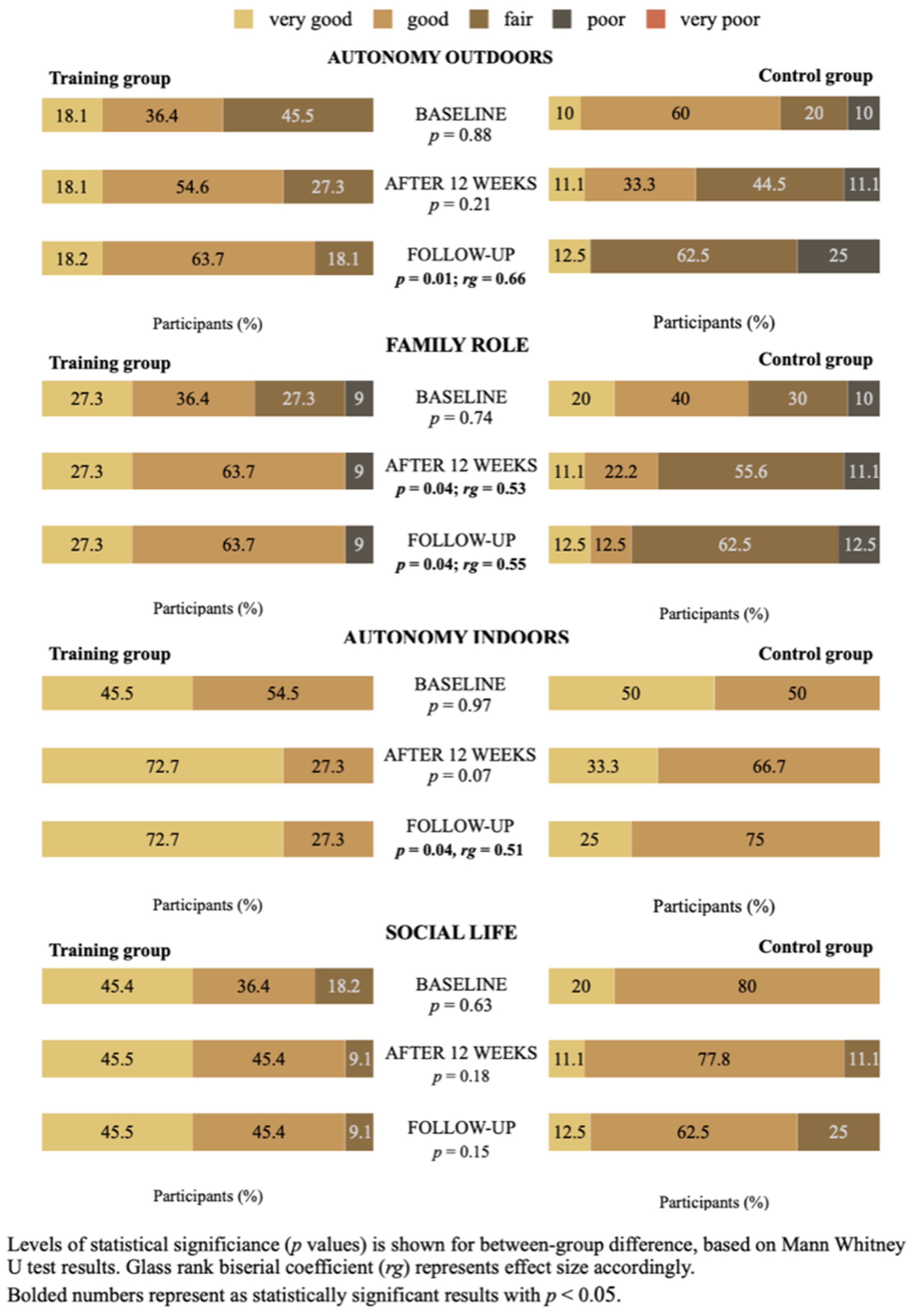
3.3. Primary Outcomes
3.4. Secondary Outcomes
4. Discussion
Strenghts and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lan, N.S.H.; Massam, B.D.; Kulkarni, S.S.; Lang, C.C. Pulmonary Arterial Hypertension: Pathophysiology and Treatment. Diseases 2018, 6, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thenappan, T.; Ormiston, M.; Ryan, J.J.; Archer, S.L. Pulmonary arterial hypertension: Pathogenesis and clinical management. BMJ 2018, 360, j5492. [Google Scholar] [CrossRef] [PubMed]
- Rawlings, G.H.; Beail, N.; Armstrong, I.; Condliffe, R.; Kiely, D.G.; Sabroe, I.; Thompson, A.R. Adults’ experiences of living with pulmonary hypertension: A thematic synthesis of qualitative studies. BMJ Open 2020, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, P.; Skåra, H. My life with pulmonary arterial hypertension: A patient perspective. Eur. Heart J. Suppl. 2019, 21, K54–K59. [Google Scholar] [CrossRef] [Green Version]
- Humbert, M.; Lau, E.M.T. Risk Stratification in Pulmonary Arterial Hypertension: Do Not Forget the Patient Perspective. Am. J. Respir. Crit. Care Med. 2021, 203, 675–677. [Google Scholar] [CrossRef]
- Eassey, D.; Reddel, H.K.; Ryan, K.; Smith, L. ‘It is like learning how to live all over again’ A systematic review of people’s experiences of living with a chronic illness from a self-determination theory perspective. Health Psychol. Behav. Med. 2020, 8, 270–291. [Google Scholar] [CrossRef]
- Åberg, C.; Gillsjö, C.; Hallgren, J.; Berglund, M. “It is like living in a diminishing world”: Older persons’ experiences of living with long-term health problems–prior to the STRENGTH intervention. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1747251. [Google Scholar] [CrossRef] [Green Version]
- Steckermeier, L.C. The Value of Autonomy for the Good Life. An Empirical Investigation of Autonomy and Life Satisfaction in Europe; Springer: Enschede, The Netherlands, 2021. [Google Scholar] [CrossRef]
- Cardol, M.; A De Jong, B.; Bos, G.A.V.D.; Beelen, A.; De Groot, I.J.M.; De Haan, R.J. Beyond disability: Perceived participation in people with a chronic disabling condition. Clin. Rehabil. 2002, 16, 27–35. [Google Scholar] [CrossRef]
- Butane, L.; Šmite, D.; Šablinskis, M.; Skride, A. Individualized home-based exercise program for idiopathic pulmonary arterial hypertension patients: A preliminary study. Cor Vasa 2019, 61, 403–410. [Google Scholar] [CrossRef] [Green Version]
- Butāne, L.; Šablinskis, M.; Skride, A.; Šmite, D. Individually tailored 12-week home-based exercise program improves both physical capacity and sleep quality in patients with pulmonary arterial hypertension. Cor Vasa 2021, 63, 325–332. [Google Scholar] [CrossRef]
- Cardol, M.; de Haan, R.J.; de Jong, B.A.; Bos, G.A.V.D.; de Groot, I.J. Psychometric properties of the impact on participation and autonomy questionnaire. Arch. Phys. Med. Rehabil. 2001, 82, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976) 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Kersten, P. Impact on Participation and Autonomy (IPA): Manual to English Version: IPA. Utr Neth. Inst. Health Serv. 2007. Available online: https://www.nivel.nl/sites/default/files/bestanden/INT-IPA-Manual.pdf (accessed on 12 March 2022).
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. American Thoracic Society ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Mathai, S.C.; Puhan, M.; Lam, D.; Wise, R. The minimal important difference in the 6-minute walk test for patients with pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2012, 186, 428–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Weegen, S.; Essers, H.; Spreeuwenberg, M.; Verwey, R.; Tange, H.; de Witte, L.; Meijer, K. Concurrent Validity of the MOX Activity Monitor Compared to the ActiGraph GT3Xle. Telemed. e-Health 2015, 21, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sport Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy Scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Nfer-Nelson: Windsor, ON, Canada, 1995; pp. 35–37. [Google Scholar]
- Buliņa, R. Perfekcionisma, Pašefektivitātes un Subjektīvās Labklājības Saistība; Latvijas Universitāte: Riga, Latvia, 2009. [Google Scholar]
- Morgan, C.J. Use of proper statistical techniques for research studies with small samples. Am. J. Physiol.-Lung Cell Mol. Physiol. 2017, 313, L873–L877. [Google Scholar] [CrossRef]
- Van Belle, G.; Fisher, L.D.; Heagerty, P.J.; Lumley, T. Biostatistics: A Methodology for the Health Sciences; Wiley: Hoboken, NJ, USA, 2004. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approachin pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 1–27. [Google Scholar] [CrossRef]
- Kerby, D.S. The Simple Difference Formula: An Approach to Teaching Nonparametric Correlation. Compr. Psychol. 2014, 3, 11.IT.3.1. [Google Scholar] [CrossRef]
- Hedman, M.; Pöder, U.; Mamhidir, A.-G.; Nilsson, A.; Kristofferzon, M.-L.; Häggström, E. Life memories and the ability to act: The meaning of autonomy and participation for older people when living with chronic illness. Scand. J. Caring Sci. 2015, 29, 824–833. [Google Scholar] [CrossRef]
- De Coninck, L.; Declercq, A.; Bouckaert, L.; Vermandere, M.; Graff, M.J.L.; Aertgeert, B. Perspectives of older adults with a chronic condition on functioning, social participation and health: A qualitative study. BMC Geriatr. 2021, 21, 418. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Chen, H.; Ruan, H.; Ye, X.; Li, J.; Hong, C. Effectiveness and safety of exercise training and rehabilitation in pulmonary hypertension: A systematic review and meta-analysis. J. Thorac. Dis. 2020, 12, 2691–2705. [Google Scholar] [CrossRef] [PubMed]
- Grünig, E.; Eichstaedt, C.; Barberà, J.-A.; Benjamin, N.; Blanco, I.; Bossone, E.; Cittadini, A.; Coghlan, G.; Corris, P.; D’Alto, M.; et al. ERS statement on exercise training and rehabilitation in patients with severe chronic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1800332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHOQOL: Measuring Quality of Life. Available online: https://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/ (accessed on 15 March 2022).
- Krahn, G.L.; Robinson, A.; Murray, A.J.; Havercamp, S.M.; Andridge, R.; Arnold, L.E.; Barnhill, J.; Bodle, S.; Boerner, E.; Bonardi, A.; et al. It’s time to reconsider how we define health: Perspective from disability and chronic condition. Disabil. Health J. 2021, 14, 101129. [Google Scholar] [CrossRef]
- Goddard, J.C.; Armstrong, I.J.; Kiely, D.G.; A Elliot, C.; Charalampopoulos, A.; Condliffe, R.; Stone, B.J.; Sabroe, I. Combining creative writing and narrative analysis to deliver new insights into the impact of pulmonary hypertension. BMJ Open Respir. Res. 2017, 4, e000184. [Google Scholar] [CrossRef] [Green Version]
- Maguire, R.; Hanly, P.; Maguire, P. Living well with chronic illness: How social support, loneliness and psychological appraisals relate to well-being in a population-based European sample. J. Health Psychol. 2021, 26, 1494–1507. [Google Scholar] [CrossRef]
- Meulenkamp, T.; Rijken, M.; Cardol, M.; Francke, A.L.; Rademakers, J. People with activity limitations’ perceptions of their health condition and their relationships with social participation and experienced autonomy. BMC Public Health 2019, 19, 1536. [Google Scholar] [CrossRef]
- McGoon, M.D.; Ferrari, P.; Armstrong, I.; Denis, M.; Howard, L.S.; Lowe, G.; Mehta, S.; Murakami, N.; Wong, B.A. The importance of patient perspectives in pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801919. [Google Scholar] [CrossRef]
- Fors, A.; Blanck, E.; Ali, L.; Ekberg-Jansson, A.; Fu, M.; Kjellberg, I.L.; Mäkitalo, Å.; Swedberg, K.; Taft, C.; Ekman, I. Effects of a person-centred telephone-support in patients with chronic obstructive pulmonary disease and/or chronic heart failure—A randomized controlled trial. PLoS ONE 2018, 13, e0203031. [Google Scholar] [CrossRef] [Green Version]
- Ali, L.; Wallström, S.; Ekman, I.; Swedberg, K.; Fors, A. Effects of person-centred care via telephone on self-efficacy in patients with chronic obstructive pulmonary disease: Subgroup analysis of a randomized controlled trial. Nurs. Open 2021, 8, 927–935. [Google Scholar] [CrossRef]
- Waller, L.; Krüger, K.; Conrad, K.; Weiss, A.; Alack, K. Effects of Different Types of Exercise Training on Pulmonary Arterial Hypertension: A Systematic Review. J. Clin. Med. 2020, 9, 1689. [Google Scholar] [CrossRef] [PubMed]
- Wojciuk, M.; Ciolkiewicz, M.; Kuryliszyn-Moskal, A.; Chwiesko-Minarowska, S.; Sawicka, E.; Ptaszynska-Kopczynska, K.; Kaminski, K. Effectiveness and safety of a simple home-based rehabilitation program in pulmonary arterial hypertension: An interventional pilot study. BMC Sports Sci. Med. Rehabil. 2021, 13, 79. [Google Scholar] [CrossRef] [PubMed]
- Chia, K.S.; Brown, K.; Kotlyar, E.; Wong, P.K.K.; Faux, S.G.; Shiner, C.T. ‘Tired, afraid, breathless’ An international survey of the exercise experience for people living with pulmonary hypertension. Pulm. Circ. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | TG (n = 11) | CG (n = 10) | Difference between Groups (p) |
|---|---|---|---|
| Age (years) | 68 (16) | 66 (11.5) | 0.78 |
| (n) < 45 | 2 | 1 | |
| 45–55 | - | - | |
| 55–65 | 2 | 2 | |
| 65–75 | 5 | 5 | |
| >75 | 2 | 2 | |
| Gender (n) Women/Men | 10/1 | 9/1 | |
| BMI (kg/m2) | 25.7 (6.7) | 26.7 (10.4) | 0.41 |
| (n) 18.5–24.99 | 6 | 5 | |
| 25–29.99 | 2 | 1 | |
| >30 | 3 | 4 | |
| PAH etiology (n) | |||
| Idiopathic | 6 | 4 | |
| Connective tissue disease | 2 | 3 | |
| Congenital heart disease | 2 | 2 | |
| PAH target therapy (n) | |||
| PDE5 inhibitor | 11 | 10 | |
| ERA | 4 | 5 | |
| Ventavis | 1 | - | |
| Spironolactonum | 11 | 9 | |
| Oxygen therapy | - | 2 | |
| Co-morbidities (n) | |||
| Hypertension | 6 | 5 | |
| Dislipidemia | 5 | 7 | |
| CHF | 9 | 7 | |
| AF | 7 | 5 | |
| Time since diagnosis (years) | |||
| Cardiac catheterization | |||
| mPAP (mmHg) | 46 (15.2) | 54.5 (20.5) | 0.31 |
| PVR (WU) | 6.8 (2.1) | 7.8 (3.5) | 0.57 |
| PAWP (mmHg) | 11 (4.5) | 11.5 (4.3) | 0.72 |
| (n) ≤ 12 | 7 | 6 | |
| 15–13 | 2 | 2 | |
| >15 | 2 | 2 | |
| Cpc-PH * | 2 | 2 | |
| Echocardiographic data | |||
| TAPSE (mm) | 18 (4) | 18 (5) | 0.93 |
| LVEF (%) | 50 (11.5) | 50 (2) | 0.97 |
| Spirometry | |||
| FVC (% pred) | 72 (21.5) | 71 (26) | 0.54 |
| FEV1 (% pred) | 74 (7.5) | 76 (26) | 0.88 |
| FEV1/FVC (% pred) | 90.6 (11.1) | 87 (24.1) | 0.24 |
| Characteristics | Baseline Mean ± SD | After 12 Weeks Mean ± SD | Change within Group p Value (Cohen’s d Value) | Follow-Up Mean ± SD | Change within Group p Value (Cohen’s d Value) | |
|---|---|---|---|---|---|---|
| 6MWT results (distance, m) | TG | 378.3 ± 124.3 | 450 ± 114 | 0.001 (1.7) ** | 473.6 ± 118.8 | <0.001 (2.1) ** |
| CG | 296.1 ±110.1 | 290.6 ± 112.2 | 0.84 (0.2) | 302.5 ± 139.7 | 0.13 (0.2) | |
| Difference between the groups p value (Cohen’s d value) | 0.12 (0.7) | 0.01 (1.4) ** | 0.01 (1.3) ** | |||
| Accelerometry results (% from total awake time) SEDENTARY | TG | 67.2 ± 8.8 | 60.7 ± 10.1 | 0.01 (0.9) ** | 58.1 ± 10.1 | 0.005 (1.0) ** |
| CG | 75.6 ± 3.6 | 63.4 ± 9.1 | 0.003 (1.4) ** | 65.2 ± 11.2 | 0.04 (0.9) | |
| Difference between the groups p value (Cohen’s d value) | 0.20 (0.9) | 0.55 (0.2) | 0.17 (0.6) | |||
| STANDING | TG | 25.4 ± 6.4 | 28.7 ± 8.8 | 0.03 (0.8) | 28.8 ± 8.9 | 0.06 (0.7) |
| CG | 21.6 ± 5.7 | 29.8 ± 7.7 | 0.03 (0.9) | 28.8 ± 9.7 | 0.03 (0.7) | |
| Difference between the groups p value (Cohen’s d value) | 0.18 (0.6) | 0.72 (0.1) | 0.97 (0) | |||
| LOW INTENSITY | TG | 1.3 ± 0.4 | 1.6 ± 0.5 | <0.001 (1.6) ** | 1.8 ± 0.7 | 0.002 (1.2) ** |
| CG | 1.0 ± 0.6 | 1.1 ± 0.4 | 0.77 (0.3) | 0.9 ± 0.4 | 0.60 (0.2) | |
| Difference between the groups p value (Cohen’s d value) | 0.23 (0.6) | 0.04 (1.1) | 0.005 (1.6) ** | |||
| MODERATE INTENSITY | TG | 7.1 ± 3.4 | 8.0 ± 2.4 | 0.21 (0.4) | 9.5 ± 3.5 | 0.002 (1.3) ** |
| CG | 4.9 ± 2.8 | 5.4 ± 2.0 | 0.67 (0.2) | 4.8 ± 1.8 | 0.19 (0.0) | |
| Difference between the groups p value (Cohen’s d value) | 0.11 (0.7) | 0.02 (1.2) | 0.002 (1.7) ** | |||
| HIGH INTENSITY | TG | 1.4 ± 1.4 | 1.3 ± 0.8 | 0.78 (0.1) | 1.7 ± 1.5 | 0.50 (0.2) |
| CG | 0.3 ± 0.3 | 0.4 ± 0.6 | 0.28 (0.2) | 0.3 ± 0.3 | 0.14 (0) | |
| Difference between the groups p value (Cohen’s d value) | 0.03 (0.8) | 0.01 (1.1) | 0.01 (0.9) | |||
| GSE results (transformed %) | TG | 64.9 ± 22.7 | 74.2 ± 17.5 | 0.004 (1.04) ** | 69.4 ± 16.5 | 0.22 (0.34) |
| CG | 55.2 ± 25.0 | 50.7 ± 20.1 | 0.37 (0.28) | 46.3 ± 25.0 | 0.25 (0.51) | |
| Difference between the groups p value (Cohen’s d value) | 0.62 (0.24) | 0.014 (1.21) | 0.043 (1.08) | |||
| IPA total score (transformed %) | TG | 24.4 ± 13.0 | 20.0 ± 10.7 | 0.005 (1.1) ** | 18.6 ± 10.2 | 0.004 (1.1) ** |
| CG | 25.6 ± 16.1 | 30.6 ± 18.0 | 0.092 (0.6) | 31.3 ± 20.2 | 0.068 (0.8) | |
| Difference between the groups p value (Cohen’s d value) | 0.98 (0) | 0.15 (0.7) | 0.14 (0.8) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butāne, L.; Spilva-Ekerte, L.; Skride, A.; Šmite, D. Individually Tailored Remote Physiotherapy Program Improves Participation and Autonomy in Activities of Everyday Life along with Exercise Capacity, Self-Efficacy, and Low-Moderate Physical Activity in Patients with Pulmonary Arterial Hypertension: A Randomized Controlled Study. Medicina 2022, 58, 662. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050662
Butāne L, Spilva-Ekerte L, Skride A, Šmite D. Individually Tailored Remote Physiotherapy Program Improves Participation and Autonomy in Activities of Everyday Life along with Exercise Capacity, Self-Efficacy, and Low-Moderate Physical Activity in Patients with Pulmonary Arterial Hypertension: A Randomized Controlled Study. Medicina. 2022; 58(5):662. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050662
Chicago/Turabian StyleButāne, Līna, Liene Spilva-Ekerte, Andris Skride, and Daina Šmite. 2022. "Individually Tailored Remote Physiotherapy Program Improves Participation and Autonomy in Activities of Everyday Life along with Exercise Capacity, Self-Efficacy, and Low-Moderate Physical Activity in Patients with Pulmonary Arterial Hypertension: A Randomized Controlled Study" Medicina 58, no. 5: 662. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050662