
Lung Fluid Volume during Cardiopulmonary Exercise Testing


1
Second Department of Internal Medicine, University of Toyama, Toyama 930-0194, Japan
2
Advocate Christ Medical Center, Oak Lawn, IL 60453, USA
*
Author to whom correspondence should be addressed.
Medicina 2022, 58(5), 685; https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050685
Submission received: 14 April 2022
/
Revised: 16 May 2022
/
Accepted: 21 May 2022
/
Published: 22 May 2022
(This article belongs to the Section Cardiology)
Abstract
:Background and Objectives: Cardiopulmonary exercise testing can be used to quantify exercise capacity in patients with heart failure with reduced ejection fraction (HfrEF). Lung fluid levels as measured non-invasively by remote dielectric sensing (ReDSTM), often correlate with intracardiac filling pressures. The change in lung fluid levels in patients with HfrEF during cardiopulmonary exercise testing is unknown. Materials and Methods: Patients with chronic HfrEF who underwent cardiopulmonary exercise testing between October 2021 and March 2022 were prospectively included in this proof-of-concept study, with ReDS values measured before and after testing. Results: Thirteen patients (median age 41 (37, 52) years, 69% men, plasma B-type natriuretic peptide 141 (57, 368) pg/mL) were included. Median peak oxygen consumption was 11.4 (10.7, 14.0) mL/kg/min. During the test, ReDS values increased from 25% to 32% only in one patient on inotropic support, whereas ReDS values remained unchanged in the other 12 patients. The former patient remained hospitalized, whereas the other patients were dischargeable without any new incidence of clinical events during the observational period (median duration 69 (33, 112] days). Conclusions: The ReDS system may be a feasible complementary tool to noninvasively assess the changes in lung fluid levels during cardiopulmonary exercise testing. The clinical implications of ReDS values during exercise needs further investigation.
1. Introduction
Cardiopulmonary exercise testing (CPET) is a well-validated risk prognostication tool in patients with chronic heart failure with reduced ejection fraction (HfrEF) for the assessment of exercise capacity [1]. Typically, a peak oxygen consumption (VO2) less than 12 mL/kg/min (on beta-blockers) or 14 mL/kg/min (off beta-blockers) at maximum exercise is strongly associated with worse clinical outcomes and progression to advanced heart failure [2]. One of the mechanisms of dyspnea in chronic HfrEF patients is the rise in left atrial pressure and subsequent worsening pulmonary congestion during exercise [3]. This can be quantified accurately with the use of simultaneous right heart catheterization [4], though routine implementation of invasive cardiopulmonary exercise stress testing is both challenging and resource-consuming.
The remote dielectric sensing (ReDSTM, Sensible Medical Innovations Ltd., Netanya, Israel) system is a novel electromagnetic-based modality to quantify lung fluid volume noninvasively. Prior data has suggested that lung fluid volume levels measured with ReDS (Figure 1) correlate with pulmonary capillary wedge pressure in patients with HfrEF [5]. The ReDS system additionally has been shown to quantify lung fluid volume levels, with a resolution comparable to chest imaging with computerized tomography [6].
The ReDS system may be a promising tool to non-invasively estimate the change in lung fluid volumes during CPET. This additional data may offer further risk stratification, in addition to consideration of beneficial therapeutic adjustments. In this proof-of-concept study, we aimed to measure the change in ReDS values during CPET in patients with chronic HfrEF.
2. Methods
2.1. Participant Selection
Patients with chronic HfrEF who underwent CPET at our institution at clinically table condition between October 2021 and March 2022 were prospectively studied. All included patients received ReDS measurements before and after CPET, as detailed below.
Patients who were not appropriate to engage in exercise due to active diseases, including uncontrolled hypertension, severe valvular diseases, pulmonary embolism, aortic dissection, severe systemic infection, and unstable ischemic heart diseases, were not included. Those who could not engage in exercise due to sarcopenia were excluded. Patients with active intra-thoracic diseases, including pulmonary pneumonia and lung cancer, were also excluded because they might affect ReDS values.
This study was approved by the institutional review board, and all participants signed informed consent prior to study inclusion.
2.2. Cardiopulmonary Exercise Test
A symptom-limited CPET was performed using a bicycle ergometer with a ventilator and expired gas analyzer (Minato Medical Science, Osaka, Japan), according to the guidelines [7]. All patients initiated the test at 20 W for a 4-minute warm-up period following the initial 3-minute rest period, and underwent a 10-Watt-per-minute ramp incremental protocol.
Continuous data of VO2, production of carbon dioxide, and minute ventilation were measured during the tests on a breath-by-breath basis. Peak VO2 was defined as the highest mean VO2 over 20 s during the exercise.
Considering the Borg scale, which indicated patients’ objective fatigue in a range of 6–20, a score above 17 was targeted to terminate the tests. The respiratory exchange ratio was targeted at above 1.10.
2.3. ReDS System
ReDS values were measured just before and after CPET in all patients. ReDS employs low-power electromagnetic signals emitted between two sensors embedded in wearable devices (Figure 1). The analyzed signals reflect the dielectric properties of the lung portion. Their dielectric coefficients are represented by a frequency-dependent number describing its interaction with electromagnetic energy. As a result, ReDS estimates the lung fluid volume as a percentage with the manufacture-proposed normal range between 20% and 35%.
2.4. Statistical Procedures
All continuous data are presented as medians with interquartile range (IQR). Categorical data are presented as numbers and percentages. The primary aim of the study is to determine the change in ReDS values prior to and after CPET. Changes in ReDS values during exercise tests were analyzed using Wilcoxon signed-rank test. All calculations were performed with SPSS Statistics 23.0 software (IBM Corp, Armonk, NY, USA), and two-sided p values less than 0.05 were considered significant.
3. Results
3.1. Baseline Characteristics
Thirteen patients in total were included, with all of them completing CPET without complications. Median age was 41 (37, 52) years, and 69% were men (Table 1). Half of them had dilated cardiomyopathy. More than half of the patients had a history of heart failure admissions. All patients had reduced or mildly reduced left ventricular ejection fraction. All patients were on appropriate guideline-directed medical therapy as tolerated, with two patients requiring continuous inotropes support.
Median (IQR) peak VO2 was 11.4 (10.7, 14.0) mL/kg/min, and the minute ventilation/carbon dioxide production slope was 33.1 (30.9, 36.7). The procedures were performed during their hospitalization for six patients, and in outpatient clinics for the remaining seven patients.
3.2. Change in ReDS Values during Cardiopulmonary Exercise Tests
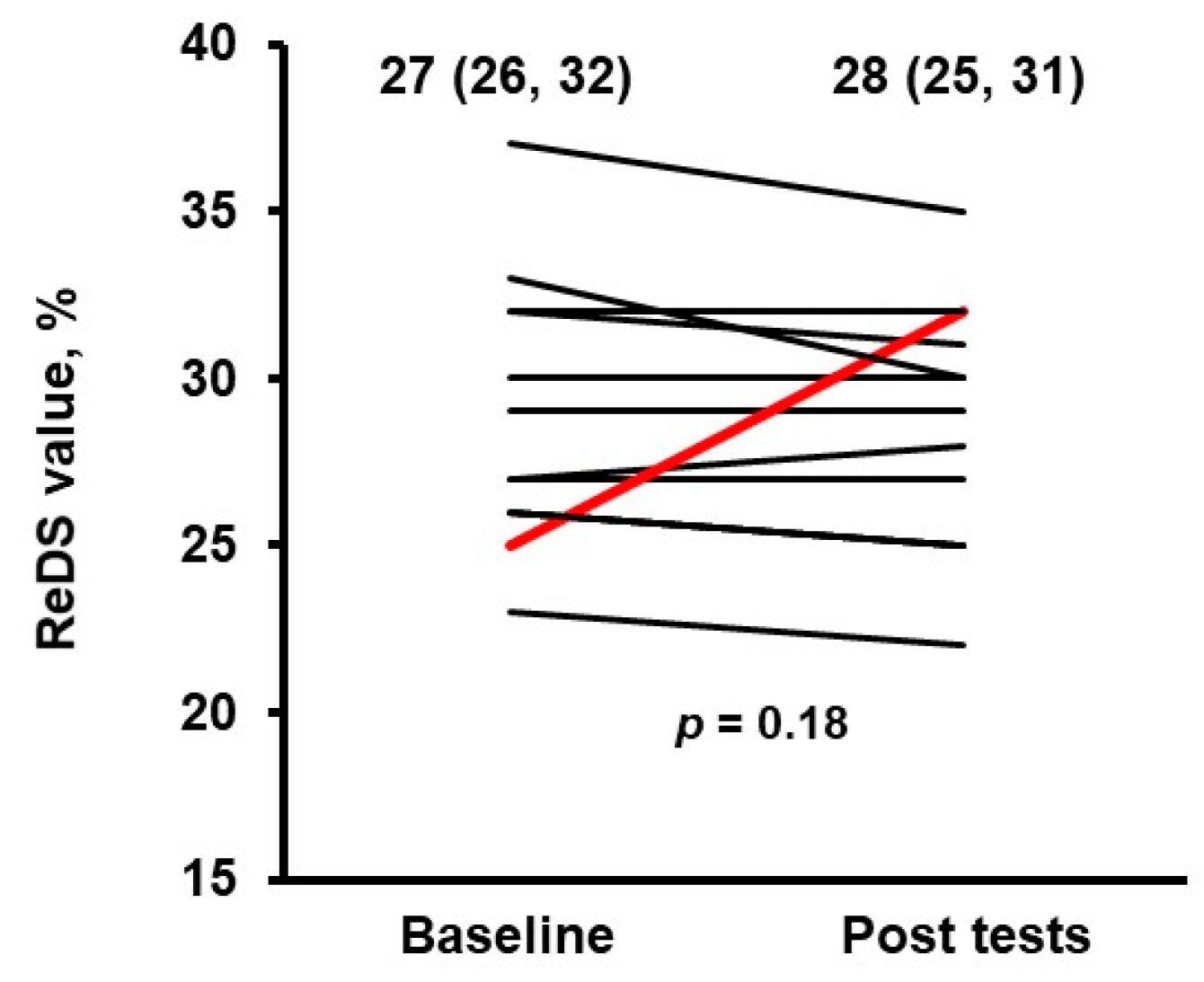
All patients completed ReDS measurements just before and after cardiopulmonary exercise tests without any troubles and measurement errors. Overall, ReDS values did not significantly change pre- and post-CPET in nearly all patients (27% [26%, 32%] to 28% [25%, 31%]; p = 0.18; Figure 2). However, ReDS values increased considerably (from 25% to 32%) in one patient who was on inotropic support (Table 1). The patient was a 45 year-old man with a left ventricular ejection fraction of 33%, and left ventricular end-diastolic diameter of 75 mm. His peak VO2 of 16.1 mL/kg/min was higher compared to the majority of the study cohort.
3.3. Post-Procedure Course
The patient with incremental ReDS values during the test remained hospitalized for 34 days as of the end of this study, undergoing evaluation for heart transplantation.
Median follow-up period of the other 12 patients was 69 (33, 112) days; Of these, five patients were hospitalized at the time of testing and were eventually discharged.
4. Discussion
In this preliminary, proof-of-concept, prospective study, we assessed the feasibility of ReDS measurements before and after CPET in patients with chronic HFrEF, in order to quantify the change in lung fluid levels during exercise. We observed no significant change in ReDS values in the majority of patients, except for a single patient dependent on inotropic support, whose ReDS value increased from 25% to 32%.
CPET is an established diagnostic modality to objectively quantify patients’ exercise capacity in the setting of chronic heart failure, offering incremental risk prognostication over the spectrum of heart failure progression [1,8]. Peak oxygen consumption offers strong prognostic information, but can be limited in interpretation when an adequate respiratory exchange ratio is not met. Furthermore, the relationships with intracardiac filling pressures during exercise and ventilator efficiency parameters including peak VO2 are not entirely known.
Incremental changes in intracardiac pressure during exercise are one of the major causes of dyspnea in patients with chronic HFrEF, and hemodynamic monitoring during exercise using invasive right heart catheterization can be used to accurately assess for these changes [4,9,10]. Although clinically informative, invasive CPET testing is both time- and resource-consuming, which may limit its widespread implementation.
The ReDS system is a novel noninvasive tool used to quantify lung fluid volume, which correlates well with intracardiac filling pressures by right heart catheterization and intraparenchymal fluid using high resolution computed tomography, when measured at rest condition [5,6,11]. The prognostic impact of ReDS values measured at rest condition was previously investigated [12].
We demonstrated only the feasibility of measuring ReDS during exercise, whereas the utility of conducting ReDS measurements during exercise as compared with other modalities remains unknown. The association between the change in ReDS during exercise and ventilator efficiency parameters also remains unknown. Of note, the patient observed with increased ReDS values during exercise had relatively preserved exercise capacity. Whether the increase in ReDS values during exercise has an independent and additional prognostic impact upon conventional ventilator efficiency parameters, including peak VO2, requires further time-to-event analyses. Furthermore, strategies to aggressively intervene upon the increase in ReDS values during exercise remain in need of further prospective analysis.
This is a preliminary proof-of-concept study, and has several limitations. All participants had reduced or mildly reduced ejection fraction, and the applicability of our findings to other etiologies, including heart failure with preserved ejection fraction, requires further analysis. With a small sample size and a skewed distribution of the outcome towards the null, larger scale studies are needed in order to understand the phenotypes of patients who have clinically meaningful changes in ReDS values following exercise. We did not compare the ReDS values with any other modalities that assess lung fluid amounts, and we only showed the feasibility of taking ReDS measurements during CPET. The usefulness of the ReDS system should be validated by comparison with other modalities in subsequent studies.
5. Conclusion
The ReDS system may be a feasible complementary tool to noninvasively assess the changes in lung fluid amounts during cardiopulmonary exercise testing. Its clinical implication needs further investigation.
Author Contributions
Conceptualization, T.I.; methodology, T.I.; software, M.H.; validation, T.I.; formal analysis, T.I.; investigation, M.H.; resources, K.K.; data curation, M.H.; writing—original draft preparation, T.I.; writing—review and editing, N.N.; visualization, T.I.; supervision, K.K.; project administration, T.I.; funding acquisition, K.K.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Ethics Committee, University of Toyama (MTK2020007, 3 March 2021).
Informed Consent Statement
Informed consents were obtained from all patients.
Data Availability Statement
Data are available upon reasonable requests.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Malhotra, R.; Bakken, K.; D’Elia, E.; Lewis, G.D. Cardiopulmonary Exercise Testing in Heart Failure. JACC Heart Fail. 2016, 4, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Mancini, D.M.; Eisen, H.; Kussmaul, W.; Mull, R.; Edmunds, L.H., Jr.; Wilson, J.R. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991, 83, 778–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayor, M.; Houstis, N.E.; Namasivayam, M.; Rouvina, J.; Hardin, C.; Shah, R.V.; Ho, J.E.; Malhotra, R.; Lewis, G.D. Impaired Exercise Tolerance in Heart Failure With Preserved Ejection Fraction: Quantification of Multiorgan System Reserve Capacity. JACC Heart Fail. 2020, 8, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Metra, M.; Faggiano, P.; D’Aloia, A.; Nodari, S.; Gualeni, A.; Raccagni, D.; Dei Cas, L. Use of cardiopulmonary exercise testing with hemodynamic monitoring in the prognostic assessment of ambulatory patients with chronic heart failure. J. Am. Coll. Cardiol. 1999, 33, 943–950. [Google Scholar] [CrossRef]
- Uriel, N.; Sayer, G.; Imamura, T.; Rodgers, D.; Kim, G.; Raikhelkar, J.; Sarswat, N.; Kalantari, S.; Chung, B.; Nguyen, A.; et al. Relationship Between Noninvasive Assessment of Lung Fluid Volume and Invasively Measured Cardiac Hemodynamics. J. Am. Heart Assoc. 2018, 7, e009175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, T.; Gonoi, W.; Hori, M.; Ueno, Y.; Narang, N.; Onoda, H.; Tanaka, S.; Nakamura, M.; Kataoka, N.; Ushijima, R.; et al. Validation of Noninvasive Remote Dielectric Sensing System to Quantify Lung Fluid Levels. J. Clin. Med. 2021, 11, 164. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. European Association for Cardiovascular P, Rehabilitation, American Heart A. EACPR/AHA Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef]
- Stelken, A.M.; Younis, L.T.; Jennison, S.H.; Miller, D.D.; Miller, L.W.; Shaw, L.J.; Kargl, D.; Chaitman, B.R. Prognostic value of cardiopulmonary exercise testing using percent achieved of predicted peak oxygen uptake for patients with ischemic and dilated cardiomyopathy. J. Am. Coll. Cardiol. 1996, 27, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Burrage, M.K.; Hundertmark, M.; Valkovic, L.; Watson, W.D.; Rayner, J.; Sabharwal, N.; Ferreira, V.M.; Neubauer, S.; Miller, J.J.; Rider, O.J.; et al. Energetic Basis for Exercise-Induced Pulmonary Congestion in Heart Failure With Preserved Ejection Fraction. Circulation 2021, 144, 1664–1678. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.N.V.; Obokata, M.; Wiley, B.; Koepp, K.E.; Jorgenson, C.C.; Egbe, A.; Melenovsky, V.; Carter, R.E.; Borlaug, B.A. The haemodynamic basis of lung congestion during exercise in heart failure with preserved ejection fraction. Eur. Heart J. 2019, 40, 3721–3730. [Google Scholar] [CrossRef] [PubMed]
- Amir, O.; Rappaport, D.; Zafrir, B.; Abraham, W.T. A novel approach to monitoring pulmonary congestion in heart failure: Initial animal and clinical experiences using remote dielectric sensing technology. Congest. Heart Fail. 2013, 19, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Bensimhon, D.; Alali, S.A.; Curran, L.; Gelbart, E.; Garman, D.W.V.; Taylor, R.; Chase, P.; Peacock, W.F. The use of the reds noninvasive lung fluid monitoring system to assess readiness for discharge in patients hospitalized with acute heart failure: A pilot study. Heart Lung 2021, 50, 59–64. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
An ReDS system consists of a monitor and a sensor unit [6].
Figure 1.
An ReDS system consists of a monitor and a sensor unit [6].

Figure 2.
Change in ReDS values before and after cardiopulmonary exercise tests. p value was calculated by Wilcoxon signed-rank test.
Figure 2.
Change in ReDS values before and after cardiopulmonary exercise tests. p value was calculated by Wilcoxon signed-rank test.


{kind=link}
{kind=link}
Table 1.
Baseline characteristics.
| (N = 13) | |
|---|---|
| Demographics | |
| Age, years | 41 (37, 52) |
| Men | 9 (69%) |
| Body mass index | 23.2 (19.9, 26.9) |
| Etiology | |
| Hypertensive heart disease | 2 (15%) |
| Ischemic heart disease | 0 (0%) |
| Dilated cardiomyopathy | 7 (54%) |
| Dilated phase of hypertensive cardiomyopathy | 2 (15%) |
| Others | 2 (15%) |
| Comorbidity | |
| Atrial fibrillation | 3 (23%) |
| Diabetes mellitus | 2 (15%) |
| History of stroke | 1 (8%) |
| History of smoking | 6 (46%) |
| History of heart failure admission | 9 (69%) |
| Previous heart failure admission times | 2 (1, 3) |
| Echocardiography data | |
| Left ventricular end-diastolic diameter, cm | 66 (54, 77) |
| Left ventricular ejection fraction, % | 29 (19, 40) |
| Left atrial diameter, mm | 38 (31, 47) |
| Moderate or greater mitral regurgitation | 1 (8%) |
| Moderate or greater tricuspid regurgitation | 1 (8%) |
| Laboratory data | |
| Hemoglobin, g/dL | 14.0 (11.9, 16.4) |
| Serum albumin, mg/dL | 3.6 (2.9, 4.5) |
| Serum sodium, mEq/L | 138 (136, 140) |
| Estimated glomerular filtration ratio, mL/min/1.73 m2 | 63.9 (47.7, 81.8) |
| Plasma B-type natriuretic peptide, pg/mL | 139 (73, 373) |
| Medication | |
| Beta-blocker | 13 (100%) |
| Renin-angiotensin system inhibitor | 13 (100%) |
| Mineralocorticoid receptor antagonist | 1 (8%) |
| Diuretics | 9 (69%) |
| Intravenous catecholamine infusion | 2 (15%) |
| New York Heart Association functional class (I/II/III/IV) | 0/8/3/2 |
| Cardiopulmonary exercise test parameters | |
| Exercise duration, min | 449 (362, 506) |
| Work load, Watt | 42 (32, 66) |
| Respiratory exchange ratio | 1.12 (1.10, 1.14) |
| Peak heart rate, bpm | 112 (95, 130) |
| Peak oxygen consumption, mL/kg/min | 11.4 (10.7, 14.0) |
| Anaerobic threshold, mL/kg/min | 8.2 (6.9, 8.7) |
| Minute ventilation/carbon dioxide production slope | 33.1 (30.9, 36.7) |
| Oxygen uptake efficiency slope | 1232 (828, 1410) |
| Peak end-tidal carbon dioxide, % | 5.0 (4.8, 5.1) |
| Peak oxygen consumption/heart rate, mL/bpm | 6.4 (5.7, 9.6) |
| Δ oxygen consumption/Δ work load, mL/min/Watt | 7.8 (5.9, 9.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Imamura, T.; Hori, M.; Narang, N.; Kinugawa, K. Lung Fluid Volume during Cardiopulmonary Exercise Testing. Medicina 2022, 58, 685. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050685
AMA Style
Imamura T, Hori M, Narang N, Kinugawa K. Lung Fluid Volume during Cardiopulmonary Exercise Testing. Medicina. 2022; 58(5):685. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050685
Chicago/Turabian StyleImamura, Teruhiko, Masakazu Hori, Nikhil Narang, and Koichiro Kinugawa. 2022. "Lung Fluid Volume during Cardiopulmonary Exercise Testing" Medicina 58, no. 5: 685. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58050685