How Technology in Care at Home Affects Patient Self-Care and Self-Management: A Scoping Review

Abstract
:1. Introduction
- What is already Known about the Topic?
- The use of technology in the care at home has potential benefits, such as improved patient outcomes, increased quality of care and increased patient involvement in the care process.
- Implementation of technology in the care at home is not always successful and it takes a long time before innovation of promising technology is implemented on a wide scale.
- What Does This Paper Add?
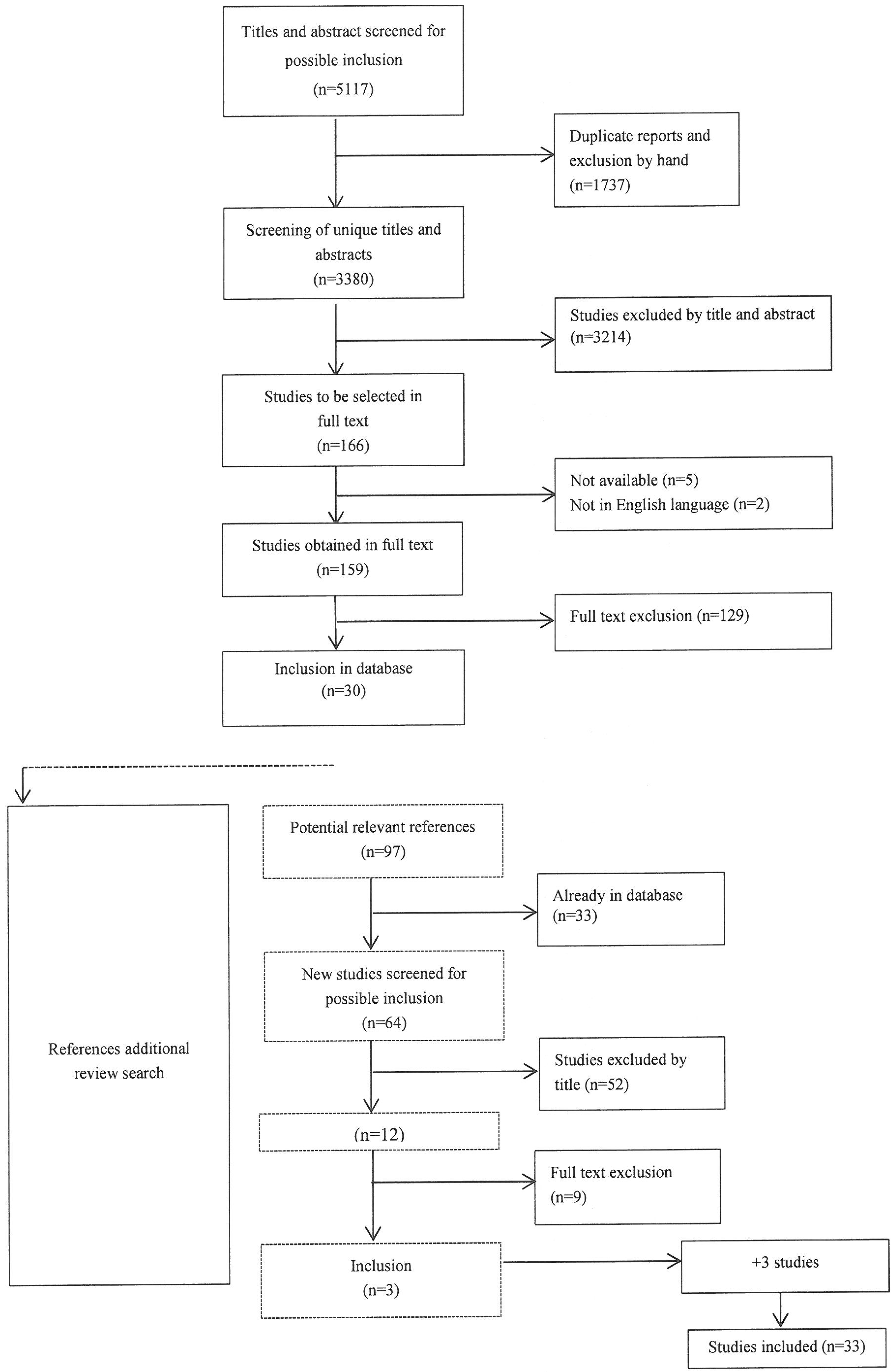
- In our review, we found 33 studies (six review studies and twenty seven individual studies) that reported effects of technology in the care at home on patient self-care and self-management.
- In almost all of the 33 included studies the authors did not use a clear definition or operationalization of self-care and self-management.
- Most of the included studies show effects of technology on the level of increased patient competence: patients using technology have a better understanding of their disease and more knowledge of the disease.
- We did not find strong convincing evidence that technology in the care at home has (a positive) effect on patient self-care and self-management.
- These findings can help to guide future research and clinical practice that support self-management efforts.
- Technology in Care at Home
- Technology in care at home is a broad term and there are many different types of technology. We give some examples. Home telemonitoring is defined as an automated process for the transmission of data about a patient’s health status from the patient’s home to the respective health care setting [1,8]. Its aim is to provide information to the health professionals without their having to visit the patient.
- Home telecare is focused on providing support from a distance to patients in their own home. Home telemedicine is defined as the direct provision of clinical care, including diagnosing, treating or consultation, via telecommunication. This may include the sharing of scans and visual images [1]. The primary function of home telemedicine is to provide specialist consultation to distant communities, rather than offer a tool for self-management of chronic disease. Assistive technology applications are very diverse, and can range from specific alarm and monitoring devices to ambient living technology. These can be used in several ways, for example to increase the comfort and independence of (chronically) ill patients [9]. For this paper, all these described domains of technology in care at home are included.
1.1. Conceptualization of Self-Care and Self-Management
1.2. Research Focus
2. Methods
2.1. Scoping Review
2.2. Literature Search
- (1).
- pubmed (United States National Library of Medicine)
- (2).
- EMBASE (Excerpta Medica Database)
- (3).
- COCHRANE LIBRARY (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Database of Abstracts of Reviews of Effects, Health Technology Assessment Database, NHS Economic Evaluation Database)
- (4).
- CINAHL (Cumulative Index to Nursing and Allied Health Literature)
- (5).
- PICARTA (Dutch Central Catalogue NCC and the Online Contents)
- (6).
- NIVEL (Netherlands Institute for Health Services Research)

{kind=link}
| “Technology” search terms: Technology, homecare, hometelecare, telecommunications, telemonitoring, telemedicine, teleconsultation, e-health, telehealth, telenursing, smart phone, mobile device, apps, ipad, social media, sms, robotics, remote care, remote sensing, video-communication, e-coaching, mobile health, m-health, gaming, health 2.0, wireless communication, data storage device, computer storage device, mobile device, electronic care, gerotechnology, sensor, camera, webcam, domotica |
| “Self-(disease)management/self-care” terms: Self-care, self-management, disease management, independence |
| “Care at home” terms: Care at home, home care, assisted living, assisted living facilities, independent living, home bound patients, home bound persons, community dwelling, ambient assisted living, home environment, patients home |
2.3. Search Terms and Strategy
2.4. Inclusion and Exclusion Criteria
- (1)
- year of publication: only from 2002 to 2012;
- (2)
- language: published in the English language;
- (3)
- type of publication: appearing in peer-reviewed journals;
- (4)
- country: only Western, Anglo-Saxon or Asian countries.
2.5. Inclusion Criteria
- The study is aimed at technology for patients living at home (sheltered housing, e.g., for persons with disabilities, was also included).
- The publication documents outcome effects of technology, i.e., patients self-management, disease management, self-care or independence.
2.6. Exclusion Criteria
- Studies that focussed exclusively on the technology itself, or on technology that is used only by care providers.
- Studies in which technology features, but is not the focus of the study, for example studies about technology-dependent children.
2.7. Data Extraction and Synthesis
2.8. Search Results

| Author and year of publication | Country | Type of patients | Type of study | Sample | Type of technology |
|---|---|---|---|---|---|
| Reviews | |||||
| Paré et al., 2007 [1] | Canada | chronic diseases | systematic review | 65 studies, number of patients not mentioned | telemonitoring: the use of audio, video and other telecommunication technologies to monitor patient status at a distance |
| Bowles & Baugh, 2007 [2] | USA | adult patients with chronic illness | summary of publications | 19 studies (28 papers) | telehomecare: telehealth technology with peripheral medical devices |
| Stumbo et al., 2009 [17] | USA | individuals with disabilities | literature and research synthesis | 71 studies, number of patients not mentioned | assistive technology |
| Gately et al., 2008 [18] | UK | patients with long-term conditions | synthesis of qualitative studies | 12 studies, 253 patients | health technologies at home |
| Jaana & Paré 2007 [19] | Canada | diabetes | literature review | 17 studies, 1,535 patients | telemonitoring: transmission and remote interpretation of patients’ data |
| Jaana et al., 2007 [20] | Canada | hypertension | literature review | 14 studies, 1,119 patients | telemonitoring: automated timely transmission of data, without involvement of health professionals |
| Individual studies | |||||
| Gomez et al., 2002 [21] | Spain | diabetes | collecting data via patient unit | 10 patients | telemedicine system: blood glucose readings downloaded in patient unit |
| Bujnowska-Fedak et al., 2011 [22] | Poland | diabetes | monitoring at home, patient questionnaires | 100 patients (50 intervention group, 50 control group) | telehome diabetes monitoring and treatment |
| Bowles & Dansky, 2002 [23] | USA | diabetes | patient questionnaires and care providers scores | 174 patients (84 intervention group, 90 control group) | telehomecare: video visits |
| Frühauf et al., 2012 [24] | Australia | psoriasis patients | patient and provider questionnaires | 10 patients | teledermatology: mobile phone with built-in camera for wireless transmission |
| Finkelstein et al., 2008 [25] | USA | multiple sclerosis | patient questionnaires | 12 patients | home automated telemedicine |
| Pecina et al., 2011 [26] | USA | complex medical illnesses | qualitative telephone survey | 20 patients | telemonitoring: remote monitoring of health parameters, videoconferencing |
| Marziali, 2009 [27] | Canada | chronic disease | patient interviews | 18 patients | protected website with links to e-mail-addresses, discussion forum, videoconferencing |
| Kuo et al., 2012 [28] | Taiwan | stroke patients | in-home monitoring | 84 patients | telehealthcare: 24-h tracing and monitoring system of health status and care use |
| LaFramboise et al., 2009 [29] | USA | heart failure | patient focus groups and interviews | 13 patients | Health Buddy: device attached to a telephone line, asking 7 questions daily, followed by educational “pearl”. |
| Dansky et al., 2008 [30] | USA | heart failure | patient telephone interview, Self-Care of Heart Failure Index | 284 patients | videobased, interactive telehealth system |
| Bowles et al., 2010 [11] | USA | heart failure | patient interviews | 188 patients | telehomecare equipment including videophone and wireless devices |
| Finkelstein & Wood, 2011 [31] | USA | heart failure | patient self-test, survey and interview | 10 patients | home automated telemedicine |
| Papasifakis & Vanderveen, 2009 [32] | USA | heart failure | patient surveys | 85 patients | self-monitoring through the use of telehealth |
| Guendelman et al., 2002 [33] | USA | children with paediatric asthma | Health buddy, diary | 134 patients (66 intervention group, 68 control group) | Health buddy |
| Brennan et al., 2010 [34] | USA | patients with chronic cardiac disease | patient questionnaires | 282 patients (146 intervention group, 136 control group) | technology-enhanced practice |
| Vontetsianos et al., 2005 [35] | Greece | COPD patients | monitoring at home, patient questionnaires | 18 patients | telehealth services: transmission of health data, videoconference |
| Sicotte et al., 2011 [36] | Canada | COPD patients | patient and care providers questionnaires | 46 patients (23 intervention group, 23 control group) | telemonitoring: web phone with touch-screen monitor, to enter and send data, receive feedback on predetermined parameters and send warnings to nursing staff |
| Wilson et al., 2009 [37] | USA | people aging with disability | home interviews and telephone contacts | 91 patients (47 intervention group, 44 control group) | assistive technology, home modifications, adjusted task performance |
| Shea & Chamoff, 2012 [38] | USA | patients with chronic conditions | secondary analysis of patient and care provider survey data | 43 patients | telemonitoring: data collection, knowledge transfer and (asynchronous) communication |
| Cardozo & Steinberg, 2010 [39] | USA | patients with chronic conditions following discharge | monitoring at home, patient questionnaires | 851 patients | case-managed telemedicine: remote monitoring of health status, electronic patient record and Health Buddy |
| Hoenig et al., 2003 [40] | USA | disabled elderly | patient survey, interviews | 2,368 patients | technological assistance |
| Chumbler et al., 2004 [41] | USA | frail elderly men | monitoring at home, patient questionnaires | 226 patients (111 intervention group, 115 control group) | distance monitoring technology: Health Buddy, two-way audio-video with or without biometric monitoring |
| Hui et al., 2006 [42] | China | older women with urinary incontinence | questionnaires and focus group | 58 patients (27 intervention group, 31 control group) | telemedicine: videoconferencing |
| Bewernitz et al., 2009 [43] | USA | dementia | observing three self-care tasks | 11 patients | intercom, remote camera, pre-recorded voice, synthesized voice, visual prompts |
| Evans et al., 2011 [44] | UK | dementia | patient questionnaires, semi-structured interviews | 1 patient | enabling smart technology: sensors and verbal messages |
| Mihailidis et al., 2008 [45] | Canada | dementia | score sheet, video | 6 patients | COACH system: tracking and prompting system |
| Maguire et al., 2005 [46] | UK | cancer patients receiving chemotherapy | grading system, patient questionnaires and interviews | 10 patients (4 intervention group, 6 control group) | handheld computer to monitor symptoms |
2.9. Study Characteristics
3. Results and Discussion
3.1. Effects of Technology on Self-Care and Self-Management
3.2. Lack of Conceptual Clarity
3.3. Meta-Synthesis of the Concepts Self-Care and Self-Management
| Author and year of publication | Type of patient | Competence | Illness-management | Independence |
|---|---|---|---|---|
| Reviews | ||||
| Paré et al., 2007 [1] | chronic diseases | improvement of awareness and feeling of security, leading to empowerment active participation in the process of care | ||
| Bowles & Baugh 2007 [2] | adult patients with chronic illness | positive effects on self-management | ||
| Stumbo et al., 2009 [17] | individuals with disabilities | more control more self confidence | assistive technology is a foundational support that produces multiple and life-changing benefits | |
| Gately et al., 2008 [18] | patients with long-term conditions | disruptive effects of health technologies on personal identities more self-regulation | disruptive effects of health technologies on strategies of managing illness | |
| Jaana & Paré, 2007 [19] | diabetes | receptiveness, empowerment, education | management of medical condition | |
| Jaana et al., 2007 [20] | hypertension | significant reduction in blood pressure, significant improvement of disease knowledge | ||
| Individual studies | ||||
| Gomez et al., 2002 [21] | diabetes | increasing patient empowerment and education | ||
| Bujnowska-Fedak et al., 2011 [22] | diabetes | achieving a sense of independence | ||
| Bowles & Dansky, 2002 [23] | diabetes | improved knowledge (not significant) | improved self-management | |
| Frühauf et al., 2012 [24] | psoriasis patients | more flexible and empowered lifestyle | ||
| Finkelstein et al., 2008 [25] | multiple sclerosis | improvement of functional outcomes | ||
| Pecina et al., 2011 [26] | complex medical illnesses | moderate increase in knowledge earlier detection of decline in health status increased personal awareness leading to behavioural changes | ||
| Marziali, 2009 [27] | chronic disease | reduced sense of isolation, maintenance of optimal healthcare strategies | ||
| Kuo et al., 2012 [28] | stroke patients | reduce daily abnormal blood pressure rate by proper measurement | ||
| LaFramboise et al., 2009 [29] | heart failure | ease of use, promote comprehension and self-management | ||
| Dansky et al., 2008 [30] | heart failure | confidence is a predictor of self-management behaviours | ||
| Bowles et al., 2010 [11] | heart failure | early identification of and intervention in clinical changes | ||
| Finkelstein & Wood, 2011 [31] | heart failure | assumed utility in daily self-management | ||
| Papasifakis & Vanderveen, 2009 [32] | heart failure | improvement of self-care improvement of disease management | ||
| Guendelman et al., 2002 [33] | paediatric asthma | self-care behaviours improved far more for the intervention group; increased self-management skills | improved asthma outcomes | |
| Brennan et al., 2010 [34] | patients with chronic cardiac disease | better self-management | improved outcome | |
| Vontetsianos et al., 2005 [35] | COPD patients | improvement of disease knowledge | improvement of self-management | |
| Sicotte et al., 2011 [36] | COPD patients | improving attitudes and behaviours concerning management of the illness | ||
| Wilson et al., 2009 [37] | people aging with disability | reducing or slowing down functional and frailty problems | improved ability to gain or maintain independence | |
| Shea & Chamoff, 2012 [38] | patients with chronic conditions | improved self-care behaviour | ||
| Cardozo & Steinberg, 2010 [39] | patients with chronic conditions following discharge | improved disease understanding | ||
| Hoenig et al., 2003 [40] | disabled elderly | technological assistance may be substituted for some personal assistance | ||
| Chumbler et al., 2004 [41] | frail elderly men | improvement in functional and cognitive outcomes | ||
| Hui et al., 2006 [42] | older women with urinary incontinence | videoconferencing is as effective as conventional management | ||
| Bewernitz et al., 2009 [43] | dementia | increased independence in some tasks | ||
| Evans et al., 2011 [44] | dementia | potential tool to support independent living | ||
| Mihailidis et al., 2008 [45] | dementia | improvement in independence | ||
| Maguire et al., 2005 [46] | cancer patients receiving chemotherapy | improving symptom management | ||
3.4. New Classification of Outcome Measures
- (1)
- competence (a better understanding of the disease, disease knowledge);
- (2)
- illness management (making choices, acting responsibly);
- (3)
- independence (social participation, autonomy).
3.5. Discussion
3.6. Methodological Quality of the Studies
3.7. Strengths and Limitations
3.8. Knowledge Gaps
4. Conclusions
Authors’ Contributions
Acknowledgments
Conflicts of Interest
References
- Paré, G.; Jaana, M.; Sicotte, C. Systematic review of home telemonitoring for chronic diseases: The evidence base. JAMA 2007, 14, 269–277. [Google Scholar]
- Barlow, J.; Bayer, S.; Castleton, B.; Curry, R. Meeting government objectives for telecare in moving from local implementation to mainstream services. J. Telemed. Telecare 2005, 11, 49–51. [Google Scholar] [CrossRef]
- Bowles, K.H.; Baugh, A.C. Applying research evidence to optimize telehomecare. J. Cardiovasc. Nurs. 2007, 22, 5–15. [Google Scholar] [CrossRef]
- Rumberger, J.; Dansky, K. Is there a business case for telehealth in home health agencies? Telemed. J. e-Health 2006, 12, 122–127. [Google Scholar] [CrossRef]
- Barlow, J.; Wright, C.; Sheasby, J.; Turber, A.; Hainsworth, J. Self-management approaches for people with chronic illness: A review. Patient Educ. Couns. 2002, 48, 177–187. [Google Scholar] [CrossRef]
- Ryan, P.; Sawin, K.J. The individual and family self-management theory: Background and perspectives on context, process and outcomes. Nurs. Outlook 2009, 57, 217–225. [Google Scholar] [CrossRef]
- Black, A.D.; Car, J.; Pagliari, C.; Anandan, C.; Cresswell, K.; Bokun, T.; McKinstry, B.; Procter, R.; Majeed, A.; Sheikh, A. The impact of eHealth on the quality and safety of health care: A systematic overview. PLoS Med. 2011, 8, e1000387. [Google Scholar] [CrossRef]
- Postema, T.R.F.; Peeters, J.M.; Friele, R.D. Key factors influencing the implementation success of a home telecare application. Int. J. Med. Inform. 2012, 81, 415–423. [Google Scholar] [CrossRef]
- Zwijsen, S.A.; Niemeijer, A.R.; Hertogh, C.M. Ethics of using technology in the care for community-dwelling elderly people: An overview of the literature. Aging Ment. Health 2011, 15, 419–427. [Google Scholar] [CrossRef]
- Lorig, K.R.; Holman, M.D. Self-management education: History, definition, outcomes and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef]
- Bowles, K.; Riegel, B.; Weiner, M.G.; Glick, H.; Naylor, M.D. The effect of telehomecare on heart failure self care. AMIA Annu. Symp. Proc. 2010, 2010, 71–75. [Google Scholar]
- Riegel, B.; Dickson, V.V. A situation specific theory of heart failure self-care. J. Cardiovasc. Nurs. 2008, 23, 190–196. [Google Scholar] [CrossRef]
- Davis, K.; Drey, N.; Gould, D. What are scoping studies? A review of the nursing literature. Int. J. Nurs. Stud. 2009, 46, 1386–1400. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Arksey, H.; Malley, L.O. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.; Booth, A. A typology of reviews: An analysis of 14 reviews types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Stumbo, N.J.; Martin, J.K.; Hedrick, B.N. Assistive technology: Impact on education, employment, and independence of individuals with physical disabilities. J. Vocat. Rehabil. 2009, 30, 99–110. [Google Scholar]
- Gately, C.; Rogers, A.; Kirk, S.; McNally, R. Integration of devices into long-term condition management: A synthesis of qualitative studies. Chronic Illn. 2008, 4, 135–148. [Google Scholar] [CrossRef]
- Jaana, M.; Paré, G. Home telemonitoring of patients with diabetes: A systematic assessment of observed effects. J. Eval. Clin. Pract. 2007, 13, 242–253. [Google Scholar] [CrossRef]
- Jaana, M.; Paré, G.; Sicotte, C. Hypertension home telemonitoring: Current evidence and recommendations for future studies. Dis. Manag. Health Outcomes 2007, 15, 19–31. [Google Scholar] [CrossRef]
- Gómez, E.J.; Hernando, M.E.; García, A.; del Pozo, F.; Cermeño, J.; Corcoy, R.; Brugués, E.; de Leiva, A. Telemedicine as a tool for intensive management of diabetes: The DIABTel experience. Comput. Methods Programs Biomed. 2002, 69, 163–177. [Google Scholar] [CrossRef]
- Bujnowska-Fedak, M.M.; Puchola, E.; Steciwko, A. The impact of telehomecare on health status and quality of life among patients with diabetes in a primary care setting in Poland. Telemed. J. e-Health 2011, 17, 153–163. [Google Scholar] [CrossRef]
- Bowles, K.H.; Dansky, K.H. Teaching self-management of diabetes. Home Healthc. Nurse 2002, 20, 36–42. [Google Scholar] [CrossRef]
- Frühauf, J.; Schwantzer, G.; Ambros-Rudolph, M.; Weger, W.; Ahlgrimm-Siess, V.; Salmhofer, W.; Hofmann-Wellenhof, R. Pilot study on the acceptance of mobile teledermatology for the home monitoring of high-need patients with psoriasis. Australas. J. Dermatol. 2012, 53, 41–46. [Google Scholar] [CrossRef]
- Finkelstein, J.; Lapshin, O.; Castro, H.; Cha, E.; Provance, P.G. Home-based physical telerehabilitation in patients with multiple sclerosis: A pilot study. J. Rehabil. Res. Dev. 2008, 45, 1361–1374. [Google Scholar] [CrossRef]
- Pecina, J.L.; Vickers, K.S.; Finnie, D.M.; Hathaway, J.C.; Hanson, G.J.; Takahashi, P.Y. Telemonitoring increases patient awareness of health and prompts health-related action: Initial evaluation of the TELE-ERA study. Telemed. J. e-Health 2011, 17, 461–466. [Google Scholar] [CrossRef]
- Marziali, E. e-Health program for patients with chronic disease. Telemed. J. e-Health 2009, 15, 176–181. [Google Scholar] [CrossRef]
- Kuo, Y.H.; Chien, Y.K.; Wang, W.R.; Chen, C.H.; Chen, L.S.; Liu, C.K. Development of a home-based telehealthcare model for improving the effectiveness of the chronic care of stroke patients. Kaohsiung J. Med. Sci. 2012, 28, 38–43. [Google Scholar] [CrossRef]
- LaFramboise, L.M.; Woster, J.; Yager, A.; Yates, B.C. A technological life buoy: Patient perceptions of the Health Buddy. J. Cardiovasc. Nurs. 2009, 24, 216–224. [Google Scholar] [CrossRef]
- Dansky, K.H.; Vasey, J.; Bowles, K. Use of telehealth by older adults to manage heart failure. Res. Gerontol. Nurs. 2008, 1, 25–32. [Google Scholar] [CrossRef]
- Finkelstein, J.; Wood, J. Implementing Home Telemanagement of Congestive Heart Failure Using Xbox Gaming Platform. In Proceedings of the 33rd Annual International Conference of the IEEE EMBS, Boston, MA, USA, 30 August–3 September 2011; pp. 3158–3163.
- Papasifakis, B.K.; Vanderveen, S. Self-care strategies are critical to disease management in home care. Heart Lung J. Acute Crit. Care 2009, 38, 263. [Google Scholar] [CrossRef]
- Guendelman, S.; Meade, K.; Benson, M.; Chen, Y.Q.; Samuels, S. Improving asthma outcomes and self-management behaviors of inner-city children. Arch. Pediatr. Adolesc. Med. 2002, 156, 114–120. [Google Scholar] [CrossRef]
- Brennan, P.F.; Casper, G.R.; Burke, L.J.; Johnson, K.; Brown, R.; Valdez, R.S.; Sebern, M.; Perez, O.; Sturgeon, B. Technology-enhanced practice for patients with chronic cardiac disease: Home implementation and evaluation. Heart Lung 2010, 39, S34–S46. [Google Scholar] [CrossRef]
- Vontetsianos, T.; Giovas, P.; Katsaras, T.; Rigopoulou, A.; Mpirmpa, G.; Giaboudakis, P.; Koyrelea, S.; Kontopyrgias, G.; Tsoulkas, B. Telemedicine-assisted home support for patients with advanced chronic obstructive pulmonary disease: Preliminary results after nine-month follow-up. J. Telemed. Telecare 2005, 11, S1:86–S1:88. [Google Scholar]
- Sicotte, C.; Paré, G.; Morin, S.; Potvin, J.; Moreault, M.P. Effects of home telemonitoring to support improved care for chronic obstructive pulmonary diseases. Telemed. J. e-Health 2011, 17, 95–104. [Google Scholar] [CrossRef]
- Wilson, D.J.; Mitchell, J.M.; Kemp, B.J.; Adkins, R.H.; Mann, W. Effects of assistive technology on functional decline in people aging with a disability. Assist. Technol. 2009, 21, 208–217. [Google Scholar] [CrossRef]
- Shea, K.; Chamoff, B. Telehomecare communication and self-care in chronic conditions: Moving toward a shared understanding. Worldviews Evid. Based Nurs. 2012, 9, 109–116. [Google Scholar] [CrossRef]
- Cardozo, L.; Steinberg, J. Telemedicine for recently discharged older patients. Telemed. J. e-Health 2010, 16, 49–55. [Google Scholar] [CrossRef]
- Hoenig, H.; Taylor, D.H., Jr.; Sloan, F.A. Does assistive technology substitute for personal assistance among the disabled elderly? Am. J. Public Health 2003, 93, 330–337. [Google Scholar] [CrossRef]
- Chumbler, N.R.; Mann, W.C.; Wu, S.; Schmid, A.; Kobb, R. The association of home-telehealth use and care coordination with improvement of functional and cognitive functioning in frail elderly men. Telemed. J. e-Health 2004, 10, 129–137. [Google Scholar] [CrossRef]
- Hui, E.; Lee, P.S.; Woo, J. Management of urinary incontinence in older women using videoconferencing versus conventional management: A randomized controlled trial. J. Telemed. Telecare 2006, 12, 343–347. [Google Scholar] [CrossRef]
- Bewernitz, M.W.; Mann, W.C.; Dasler, P.; Belchior, P. Feasibility of machine-based prompting to assist persons with dementia. Assist. Technol. 2009, 21, 196–207. [Google Scholar] [CrossRef]
- Evans, N.; Carey-Smith, B.; Orpwood, R. Using smart technology in an enabling way: A review of using technology to support daily life for a tenant with moderate dementia. Br. J. Occup. Ther. 2011, 74, 249–253. [Google Scholar] [CrossRef]
- Mihailidis, A.; Boger, J.N.; Craig, T.; Hoey, J. The COACH prompting system to assist older adults with dementia through handwashing: An efficacy study. BMC Geriatr. 2008, 8, 28. [Google Scholar] [CrossRef]
- Maguire, R.; Miller, M.; Sage, M.; Norrie, J.; McCann, L.; Taylor, L.; Kearney, N. Results of a UK based pilot study of a mobile phone based advanced symptom management system (ASyMS) in the remote monitoring of chemotherapy related toxicity. Clin. Eff. Nurs. 2005, 9, 202–210. [Google Scholar] [CrossRef]
- Wilson, P.M.; Kendall, S.; Brooks, F. Nurses’ responses to expert patients: The rhetoric and reality of self-management in long-term conditions: A grounded theory study. Int. J. Nurs. Stud. 2006, 43, 803–818. [Google Scholar] [CrossRef]
- Song, M. Diabetes mellitus and the importance of self-care. J. Cardiovasc. Nurs. 2010, 25, 93–98. [Google Scholar] [CrossRef]
- Schulman-Green, D.; Jaser, S.; Martin, F.; Alonzo, A.; Grey, M.; McCorkle, R.; Redeker, S.; Reynolds, N.; Whittermore, R. Processes of self-management in chronic illness. J. Nurs. Scholarsh. 2012, 44, 136–144. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Peeters, J.M.; Wiegers, T.A.; Friele, R.D. How Technology in Care at Home Affects Patient Self-Care and Self-Management: A Scoping Review. Int. J. Environ. Res. Public Health 2013, 10, 5541-5564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph10115541
Peeters JM, Wiegers TA, Friele RD. How Technology in Care at Home Affects Patient Self-Care and Self-Management: A Scoping Review. International Journal of Environmental Research and Public Health. 2013; 10(11):5541-5564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph10115541
Chicago/Turabian StylePeeters, José M., Therese A. Wiegers, and Roland D. Friele. 2013. "How Technology in Care at Home Affects Patient Self-Care and Self-Management: A Scoping Review" International Journal of Environmental Research and Public Health 10, no. 11: 5541-5564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph10115541