Vitamin D and Psoriasis Pathology in the Mediterranean Region, Valencia (Spain)

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
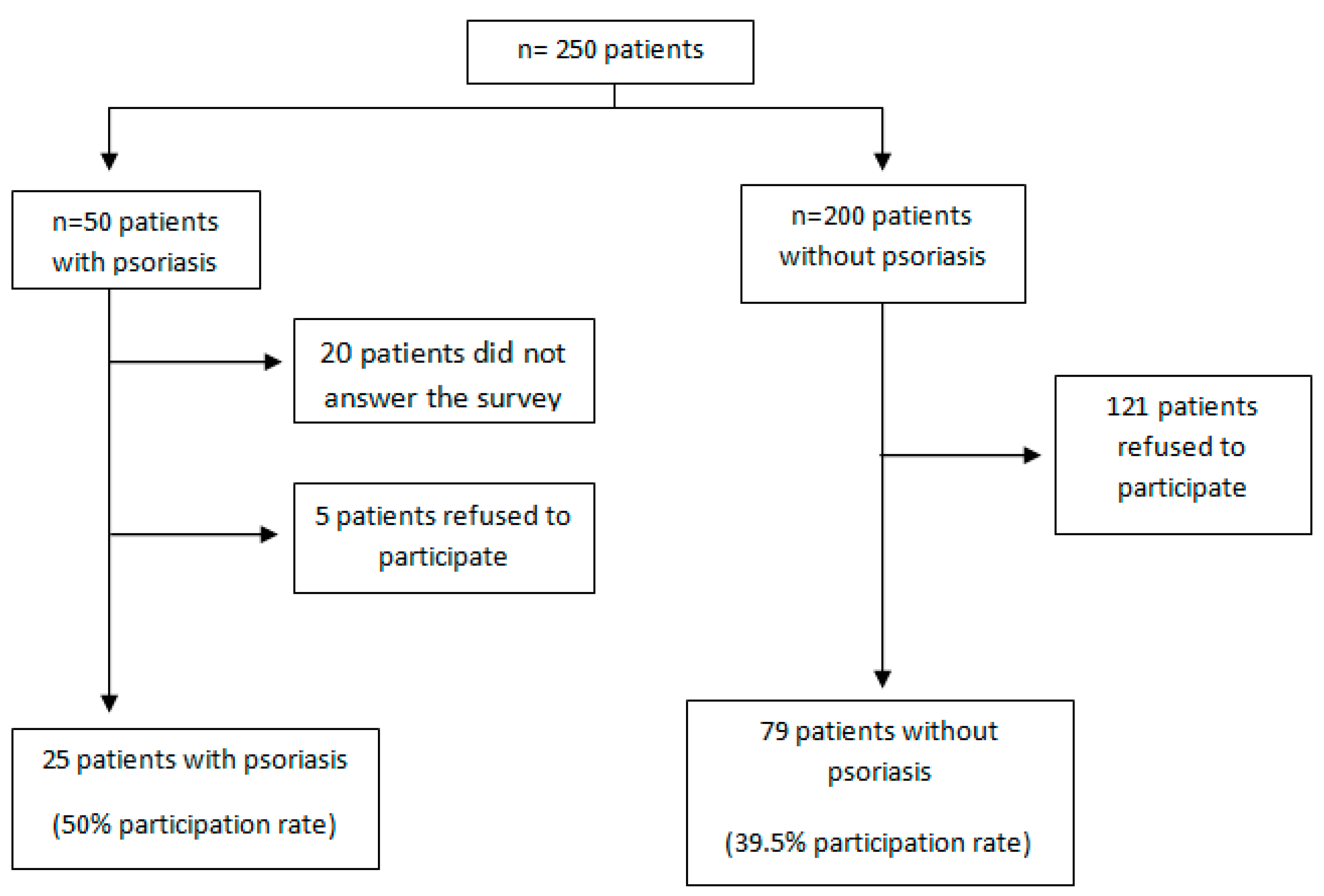
2.1. Cases and Controls
2.2. Statistical Analysis
3. Results


{kind=link}
| Baseline Characteristics and Comorbidity | Cases (n = 25) | Controls (n = 79) | p Value | Odds Ratio (95% CI) |
|---|---|---|---|---|
| Fr (%)/Mean (SD) | Fr (%)/Mean (SD) | |||
| Male gender | 11 (44) | 32 (40) | 0.700 | |
| Mean age ± SD, years | 38 ± 15 | 42 ± 16 | 0.200 | |
| Mean weight ± SD, kg | 78 ± 26 | 64 ± 2 | 0.010 | |
| Mean BMI ± SD | 27 ± 8 | 23 ± 8 | 0.010 | |
| Normal weight | 6 (24) | 46 (58) | - | 1 |
| Overweight | 10 (40) | 22 (28) | 0.004 | 3.5 [1.1–10.8] |
| Obesity | 9 (36) | 11 (14) | 0.003 | 6.3 [1.8–21.3] |
| Hypertension | 3 (12) | 6 (8) | 0.004 | 1.6 [0.4–7.2 ] |
| Dyslipidaemia | 4 (16) | 4 (5) | 0.001 | 3.6 [0.8–15.5] |
| Diabetes | 1 (4) | 3 (4) | 0.700 | 1.1 [0.10–10.6] |
| Metabolic syndrome | 1 (4) | 1 (1) | 0.001 | 3.2 [0.2–53.9] |
| Bone pathology | 2 (8) | 2 (2) | 0.001 | 1.6 [0.3–9.5] |
| Macronutrient | Cases (n = 25) | Controls (n = 79) | Total (n = 104) | p Value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Energy (kilocalories) | 1900 ± 1000 | 1940 ± 570 | 1930 ± 704 | 0.700 |
| Carbohydrates (grams) | 190 ± 100 | 190 ± 27 | 190 ± 72 | 0.800 |
| Lipids (grams) | 78 ± 41 | 85 ± 30 | 84 ± 33 | 0.300 |
| Proteins (grams) | 78 ± 41 | 86 ± 27 | 84 ± 33 | 0.400 |
| Water (mL) | 190 ± 1200 | 2100 ± 645 | 2055 ± 807 | 0.400 |
| Intake | Cases | R_Cases | p Value | Controls | R_Controls | p Value | |
|---|---|---|---|---|---|---|---|
| Vitamin D (UI/day) | 230 ± 190 | 620 ± 330 | 0.030 | 290 ± 280 | 540 ± 220 | 0.001 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Langley, R.G.; Krueger, G.G.; Griffiths, C.E. Psoriasis: Epidemiology, clinical features, and quality of life. Ann. Rheum. Dis. 2005, 64, ii18–ii23. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, S.L.; Gilleaudeau, P.; Johnson, R.; Estes, L.; Woodworth, T.G.; Gottlieb, A.B.; Krueger, J.G. Response of psoriasis to a lymphocyte-selective toxin (DAB389IL-2) suggests a primary immune, but not keratinocyte, pathogenic basis. Nat. Med. 1995, 1, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Krueger, G.; Ellis, C.N. Psoriasis-recent advances in understanding its pathogenesis and treatment. J. Am. Acad. Dermatol. 2005, 53, S94–S100. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, G.J.; Hutchinson, P.E. Psoriasis in the community: Prevalence, severity and patients beliefs and titudes towards the disease. Br. J. Dermatol. 1996, 135, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Weinstein, R.; Porter, S.B.; Neimann, A.L.; Berlin, J.A.; Margolis, D.J. Prevalence and treatment of psoriasis in the United Kingdom: A population-based study. Arch. Dermatol. 2005, 141, 1537–1541. [Google Scholar] [CrossRef] [PubMed]
- Koo, J. Population-based epidemiologic study of psoriasis with emphasis on quality of life assessment. Dermatol. Clin. 1996, 14, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Naldi, L.; Chatenoud, L.; Linder, D.; Belloni Fortina, A.; Peserico, A.; Virgili, A.R.; Bruni, P.L.; Ingordo, V.; Lo Scocco, G.; Solaroli, C.; et al. Cigarette smoking, body mass index, and stress full if events as risk factors for psoriasis: Results from an Italian case control study. J. Invest. Dermatol. 2005, 125, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Płudowski, P.; Karczmarewicz, E.; Bayer, M.; Carter, G.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dębski, R.; Decsi, T.; Dobrzańska, A.; Franek, E.; et al. Practical guidelines for the supplementation of vitamin D and the treatment of deficits in Central Europe—Recommended vitamin D intakes in the general population and groups at risk of vitamin D deficiency. Endokrvnol. Pol. 2013, 64, 319–327. [Google Scholar] [CrossRef]
- Pludowski, P.; Holick, M.F.; Pilz, S.; Wagner, C.L.; Hollis, B.W.; Grant, W.B.; Shoenfeld, Y.; Lerchbaum, E.; Llewellyn, D.J.; Kienreich, K.; et al. Vitamin D effects on musculoskeletal health, immunity, autoimmunity, cardiovascular disease, cancer, fertility, pregnancy, dementia and mortality-a review of recent evidence. Autoimmun. Rev. 2013, 12, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Agmon-Levin, N.; Theodor, E.; Segal, R.M.; Shoenfeld, Y. Vitamin D in systemic and organ-specific autoimmune diseases. Clin. Rev. Allergy Immunol. 2013, 45, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-hydroxyvitamin D and risk of myocardial infarction in men: A rospective study. Arch. Intern. Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, E.A.; Monson, R.R.; MacMahon, B. Reduction in mortality from coronary heart disease in men residing at high altitude. N. Engl. J. Med. 1977, 296, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, L.L.; Shoenfeld, Y.; Sartori, A. Immunomodulation in human and experimental arthritis: including vitamin D, helminths and heat-shock proteins. Lupus 2014, 23, 577–587. [Google Scholar] [CrossRef] [PubMed]
- LoPiccolo, M.C.; Lim, H.W. Vitamin D in health disease. Photodermatol. Photoinmunol. Photomed. 2010, 26, 224–229. [Google Scholar] [CrossRef]
- Gniadecki, R.; Gajkowska, B.; Hansen, M. 1,25-dihydroxyvitamin D3 Stimulates the assembly of adherensjinctions in keratinocytes: Involvement of protein kinase C. Endocrinology 1997, 138, 2241–2248. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Leung, P.S.; Adamopoulos, I.E.; Gershwin, M.E. The Implication of Vitamin D and autoimmunity: A comprehensive review. Clin. Rev. Allergy Immunol. 2013, 45, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Khalili, H.; Higuchi, L.M.; Bao, Y.; Korzenik, J.R.; Giovannucci, E.L.; Richter, J.M.; Fuchs, C.S.; Chan, A.T. Higher predicted vitamin D status is associated with reduced risk of Crohn’s disease. Gastroenterology 2012, 142, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Haga, H.J.; Schmedes, A.; Naderi, Y.; Moreno, A.M.; Peen, E. Severe deficiency of 25-Hydroxyvitamin D(3) (25-OH-D (3)) is associated with high disease activity of rheumatoid arthritis. Clin. Rheumatol. 2013, 32, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Borella, E.; Nesher, G.; Israeli, E.; Shoenfeld, Y. Vitamin D: A new anti-infective agent? Ann. N Y Acad. Sci. 2014, 1317, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Requejo, A.M.; López-Sobaler, A.M. Modelos de cuestionarios para realización de estudios dietéticos en la valoración del estado nutricional. In Manual de Nutrición Clínica en Atención Primaria; Requejo, A.M., Ortega, R.M., Eds.; Nutriguia: Madrid, Spain, 2006; pp. 456–459. [Google Scholar]
- Ortega, R.M.; Lopez, A.M.; Andrés, P.; Requejo, A.M.; Aparicio, A.; Molinero, L.M. DIAL programa para la evaluación de dietas y gestión de datos de alimentación; Versión 2.16; Alce ingeniería: Madrid, Spain, 2012. [Google Scholar]
- Biesalski, H.K.; Aggett, P.J.; Anton, R.; Bernstein, P.S.; Blumberg, J.; Heaney, R.P.; Henry, J.; Nolan, J.M.; Richardson, D.P.; van Ommen, B.; et al. 26th Hohenheim Consensus Conference, September 11, 2010 Scientific substantiation of health claims: Evidence-based nutrition. Nutrition 2011, 27, S1–S20. [Google Scholar] [CrossRef] [PubMed]
- Gilaberte, Y.; Aguilera, J.; Carrascosa, J.M.; Figueroa, F.L.; Romaní de Gabriel, J.; Nagore, E. Vitamin D: Evidence and controversies. Actas Dermosifiliogr. 2011, 102, 572–588. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, S.; Kumahara, Y. A patient with psoriasis cured by 1 alpha-hydroxyvitamin D3. Med. J. Osaka Univ. 1985, 35, 51–54. [Google Scholar] [PubMed]
- Wu-wong, J.R.; Tian, J.; Golzman, D. Vitamin D analogs as therapeutic agents: A clinical study update. Curr. Opin. Investing Drugs 2004, 5, 320–326. [Google Scholar]
- Morimoto, S.; Yoshikawa, K.; Fukuo, K.; Shiraishi, T.; Koh, E.; Imanaka, S.; Kitano, S.; Ogihara, T. Inverse relation between severity of psoriasis and serum 1,25-dihydroxy-vitamin D level. J. Dermatol. Sci. 1990, 1, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Orgaz-Molina, J.; Magro-Checa, C.; Arrabal-Polo, M.A.; Raya-Álvarez, E.; Naranjo, R.; Buendía-Eisman, A.; Arias-Santiago, S. Association of 25-hydroxyvitamin D with metabolic syndrome in patients with psoriasis: A case-control study. Acta Derm. Venereol. 2014, 94, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Okita, H.; Ohtsuka, T.; Yamakage, A.; Yamazaki, S. Polymorphism of the vitamin D(3) receptor in patients with psoriasis. Arch. Dermatol. Res. 2002, 294, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Svensson, J.; Lyngaae-Jørgensen, A.; Carstensen, B.; Simonsen, L.B.; Mortensen, H.B.; Danish Childhood Diabetes Registry. Long-term trends in the incidence of type 1 diabetes in Denmark: The seasonal variation changes over time. Pediatr. Diabetes 2009, 10, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Mohr, S.B.; Garland, C.F.; Gorham, E.D.; Garland, F.C. The association between ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide. Diabetologia 2008, 51, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Gorham, E.D.; Garland, C.F.; Burgi, A.A.; Mohr, S.B.; Zeng, K.; Hofflich, H.; Kimm, J.J.; Ricordi, C. Lower prediagnostic serum 25-hydroxyvitamin D concentration is associated with higher risk of insulin-requiring diabetes: A nested case-control study. Diabetologia 2012, 55, 3224–3227. [Google Scholar] [CrossRef] [PubMed]
- Yamshchikov, A.; Desai, N.S.; Blumberg, H.M.; Ziegler, T.R.; Tangpricha, V. Vitamin D for the treatment and prevention of infectious diseases: A systematic review of randomized controlled trials. Endocr. Pract. 2009, 15, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C. Vitamin D regulation of the renin-angiotensin system. J. Cell. Biochem. 2003, 88, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Opländer, C.; Volkmar, C.M.; Paunel-Görgülü, A.; van Faassen, E.E.; Heiss, C.; Kelm, M.; Halmer, D.; Mürtz, M.; Pallua, N.; Suschek, C.V. Whole body UVA irradiation lowers systemic blood pressure by release of nitric oxide from intracutaneous photolabile nitric oxide derivates. Circ. Res. 2009, 105, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Grimble, R.F.; Tappia, P.S. Modulation of pro-inflammatory cytokine biology by unsaturated fatty acids. Z Ernahrungswiss. 1998, 37, 57–65. [Google Scholar] [PubMed]
- Gerdes, S.; Rostami-Yazdi, M.; Mrowietz, U. Adipokines and psoriasis. Exp. Dermatol. 2011, 20, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Katz, U.; Shoenfeld, Y.; Zakin, V.; Sherer, Y.; Sukenik, S. Scientific evidence of the therapeutic effects of dead sea treatments: A systematic review. Semin. Arthritis Rheum. 2012, 42, 186–200. [Google Scholar] [CrossRef] [PubMed]
- Kudish, A.I.; Harari, M.; Evseev, E.G. The measurement and analysis of normal incidence solar UVB radiation and its application to the photoclimatherapy protocol for psoriasis at the Dead Sea, Israel. Photochem. Photobiol. 2011, 87, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Love, T.J.; Qureshi, A.A.; Karlson, E.W.; Gelfand, J.M.; Choi, H.K. Prevalence of metabolic syndrome in psoriasis: Results from the national health and nutrition examination survey 2003–2006. Arch. Dermatol. 2011, 147, 419–424. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suárez-Varela, M.M.; Reguera-Leal, P.; Grant, W.B.; Rubio-López, N.; Llopis-González, A. Vitamin D and Psoriasis Pathology in the Mediterranean Region, Valencia (Spain). Int. J. Environ. Res. Public Health 2014, 11, 12108-12117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111212108
Suárez-Varela MM, Reguera-Leal P, Grant WB, Rubio-López N, Llopis-González A. Vitamin D and Psoriasis Pathology in the Mediterranean Region, Valencia (Spain). International Journal of Environmental Research and Public Health. 2014; 11(12):12108-12117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111212108
Chicago/Turabian StyleSuárez-Varela, Maria Morales, Paloma Reguera-Leal, William B. Grant, Nuria Rubio-López, and Agustín Llopis-González. 2014. "Vitamin D and Psoriasis Pathology in the Mediterranean Region, Valencia (Spain)" International Journal of Environmental Research and Public Health 11, no. 12: 12108-12117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111212108