
Healthy versus Unhealthy Suppliers in Food Desert Neighborhoods: A Network Analysis of Corner Stores’ Food Supplier Networks

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Setting
2.2. Study Sample
2.3. Defining Corner Stores’ Healthy versus Unhealthy Suppliers
2.4. Defining Corner Stores’ Healthy versus Unhealthy Supplier Networks
2.5. Supplier Network Analysis
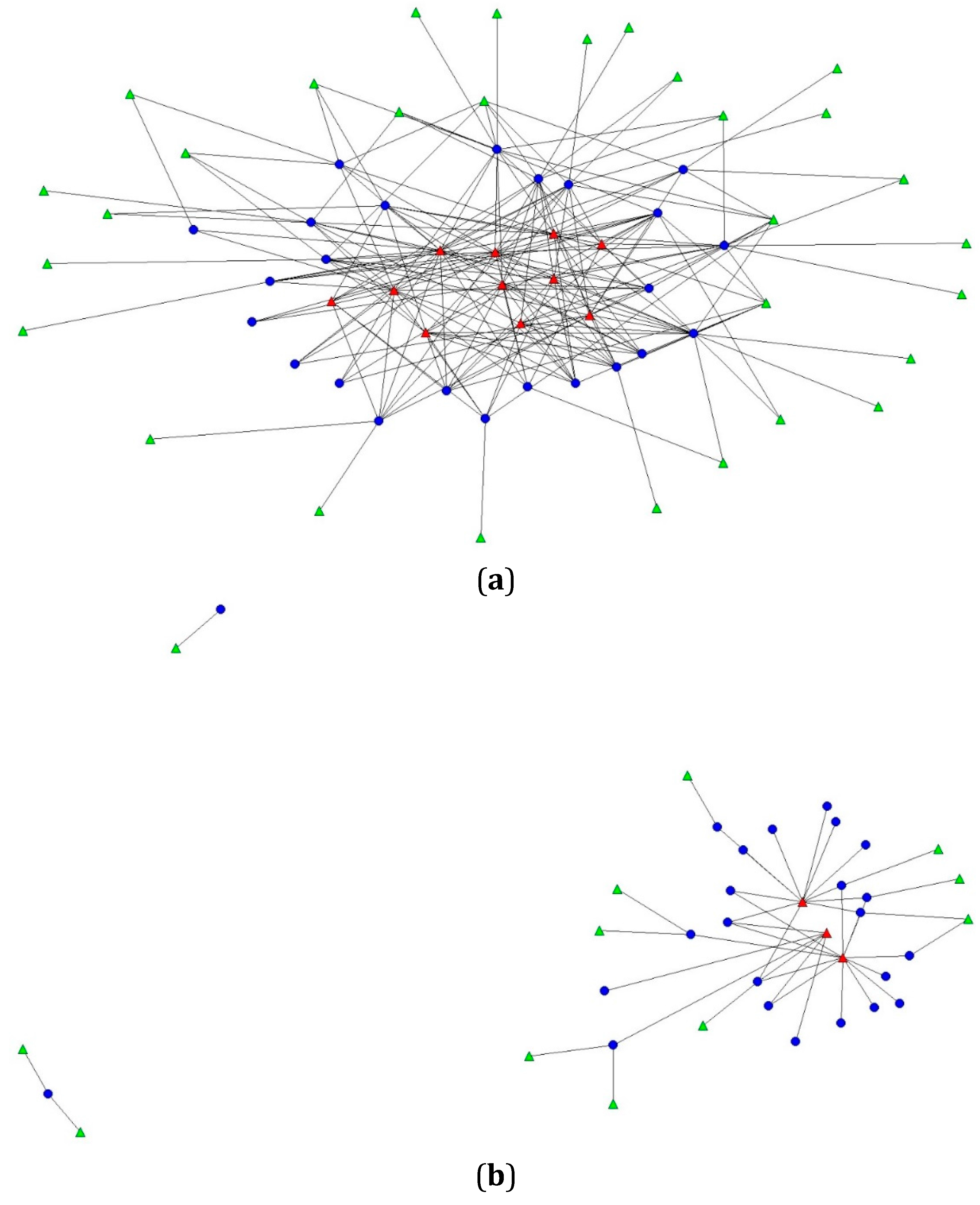
- Network core (two-mode sociogram): Set of suppliers that are central to each network, encompassing at least 80% of possible connections, or edges, between corner stores and suppliers [42]. Suppliers in the core indicate higher connectivity and importance in the network.
- Diversity (two-mode sociogram): Number of different types of suppliers connected to each corner store in the network; type of supplier was classified based on the U.S. Department of Labor, Standard Industrial Classification food store categories [32].
- Degree centrality (two-mode sociogram): Corner store’s number of existing connections with suppliers, expressed as a normalized percentage (number of existing connections divided by all possible connections with suppliers in the network). Higher degree centrality indicates greater connectedness between suppliers and corner stores in the network, and highly connected suppliers to corner stores may have greater influence, whereas relatively isolated suppliers with less connectedness may have little influence.
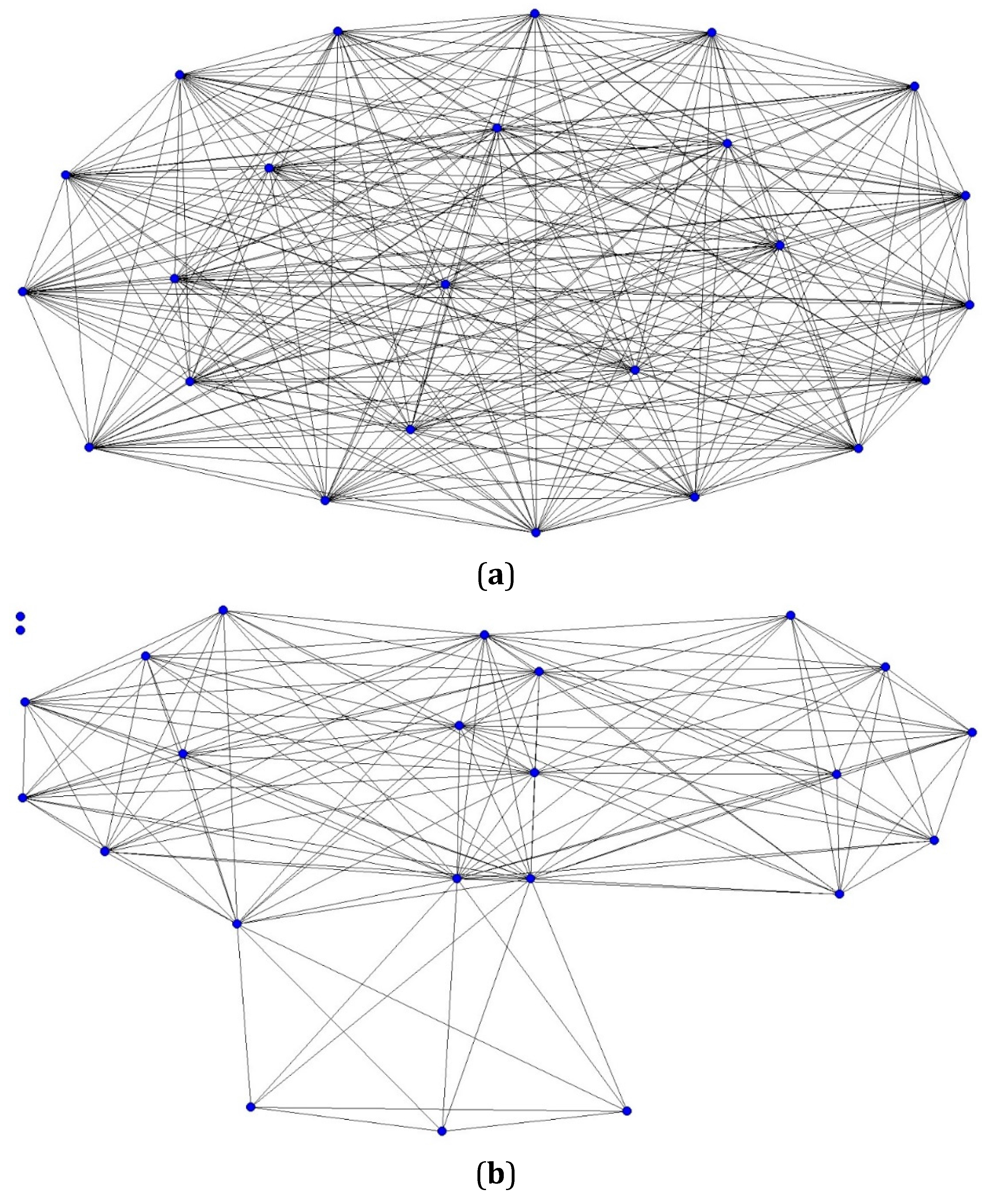
- Density (one-mode sociogram): Number of corner stores sharing at least one supplier, expressed as a percentage. Density can be interpreted as representing cohesion or the extent to which corner stores in a network are linked together through shared suppliers.
2.6. Statistical Analyses
2.7. Bivariate Regression Analysis
2.7.1. Dependent Variable
2.7.2. Independent Variables
3. Results and Discussion
3.1. Network Core Suppliers and Diversity of Suppliers

{kind=link}
{kind=link}
| Corner Stores (n = 24) | Overall (mean ± SD) |
|---|---|
| Average distance to suppliers, km | 34.0 ± 29.2 |
| Accept WIC, yes | 45.8% |
| Accept SNAP, yes | 91.7% |
| Storeowner ethnicity | |
| African American | 21.0% |
| Asian or Hispanic | 79.0% |
| # years operating current store | 9.5 ± 7.7 |
| # years operating any food store | 15.6 ± 9.1 |
| # customers on an average day | 165.0 ± 145.2 |
| # non-family paid employees | 0.75 ± 1.0 |
| # family member employees | 1.96 ± 1.3 |
| Unhealthy Supplier Network | Healthy Supplier Network |
|---|---|
| Wholesale club | |
| B. Green Wholesale East | B. Green Wholesale East |
| B. Green Wholesale West | B. Green Wholesale West |
| BJ’s Wholesale Club | BJ’s Wholesale Club |
| Costco Wholesale | Costco Wholesale |
| Eastern Food Services | Jetro Cash & Carry |
| George J. Falter Co. | Maryland Cash & Carry (2) |
| Jetro Cash & Carry | Sam’s Club |
| LG Wholesale | |
| Maryland Cash & Carry | |
| Restaurant Depot | |
| Sam’s Club | |
| Snacks | |
| Berliner Specialty Distributors (ice cream) | McKee Foods |
| Blue Bunny (ice cream) | Utz Quality Foods |
| Brigg’s Ice Cream Co. | |
| Frito Lay | |
| Herr’s Snacks | |
| McKee Foods | |
| Raylicious | |
| Stone Creek Countrywide Snacks | |
| Tastykake | |
| Utz Quality Foods | |
| Other Specialty Foods | |
| Farmer’s market | |
| Hauswald Bakery | |
| Sponseller’s Egg Co. | |
| Zeke’s Coffee | |
| Beverages | |
| Arizona Beverages USA | |
| Canada Dry | |
| Coca-Cola Company | |
| Everfresh Beverages | |
| PepsiCo | |
| Supermarket/Grocery | |
| Food Depot | Giant Food Stores |
| Giant Food Stores | Wegmans |
| Mars Supermarkets | Safeway |
| Martin’s Food Markets | Save-A-Lot |
| Safeway | |
| Save-A-Lot | |
| Shoppers Foods and Pharmacy | |
| Stop Shop and Save | |
| Discount Department Store | |
| Dollar Mark | Walmart |
| Walmart | |
| Meat Market | |
| Manger Packing Corporation | |
3.2. Degree Centrality

3.3. Corner Store Characteristics Associated with Degree Centrality
| Unhealthy Supplier Network (n = 41) | Healthy Supplier Network (n = 15) | |||
|---|---|---|---|---|
| b (95% CI) | P | b (95% CI) | P | |
| Average distance to suppliers (km) | 0.018 (−0.008, 0.044) | 0.156 | 0.041 (−0.047, 0.128) | 0.345 |
| Accept WIC, yes | 1.315 (−1.656, 4.286) | 0.369 | −0.287 (−1.086, 0.513) | 0.465 |
| Accept SNAP, yes | −0.182 (−5.639, 5.275) | 0.946 | −1.864 (−3.067, −0.660) | 0.004 |
| Storeowner ethnicity | ||||
| African American | ref | ref | ref | ref |
| Asian/Hispanic | 0.295 (−3.417, 4.007) | 0.871 | −1.526 (−2.255, −0.798) | <0.001 |
| # years operating current store | 0.169 (−0.017, 0.355) | 0.072 | −0.006 (−0.060, 0.048) | 0.818 |
| # years operating any food store | 0.104 (−0.059, 0.267) | 0.198 | −0.028 (−0.016, 0.071) | 0.196 |
| # customers on an average day | 0.004 (−0.006, 0.015) | 0.431 | 0.000 (−0.003, 0.002) | 0.777 |
| # non-family paid employees | 0.311 (−1.241,1.863) | 0.682 | 0.077 (−0.337, 0.493) | 0.701 |
| # family member employees | 0.582 (−0.544, 1.708) | 0.295 | 0.019 (−0.289, 0.328) | 0.898 |
3.4. Sensitivity Analysis
3.5. Supplier Network Density

4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
| Food | Standard Unit |
|---|---|
| Phase 1: Healthy Beverages | |
| 1% Milk, Rutters | Half Gallon |
| 1% Milk, Rutters | Gallon |
| 1% Milk, Rutters | Quart |
| Bottled Water, Deer Park | 16.9 fl oz bottle |
| Bottled Water, Deer Park | 23.7 fl oz bottle |
| Pepsi Next | 1 bottle (24 fl oz) |
| Coke Zero | 1 bottle (24 fl oz) |
| Phase 2: Healthy Essentials | |
| Solid White Albacore Tuna in water, Bumblebee | 1 can (5 oz) |
| Solid White Albacore Tuna in water, Starkist | 1 can (5 oz) |
| Chunk Light Tuna in water, Bumblebee | 1 can (5 oz) |
| Chunk Light Tuna in water, Starkist | 1 can (5 oz) |
| 100% Whole Wheat Bread, “Schmidt Old Tyme” | 1 Loaf |
| Frozen Stir-Fry Vegetables, Bird’s Eye | 1 bag (12 oz) |
| Frozen Collards, Bird’s Eye | 1 bag (12 oz) |
| Frozen Broccoli, Bird’s Eye | 1 bag (12 oz) |
| Frozen Vegetables Type: | |
| Frozen Vegetables Type: | |
| Frozen Vegetables Type: | |
| Frozen Vegetables Type: | |
| Frozen Vegetables Type: | |
| Frozen Vegetables Type: | |
| Phase 3: Healthy Snacks | |
| Apples, Gala | 1 fruit |
| Bananas | 1 fruit |
| Oranges, Navel | 1 fruit |
| Fresh Fruit Type: | 1 fruit |
| Fresh Fruit Type: | 1 fruit |
| Fresh Fruit Type: | 1 fruit |
| Fresh Fruit Type: | 1 fruit |
| Baked Potato Chips, Assorted Utz | 1 oz bag |
| Baked Potato Chips List: | |
| Baked Potato Chips List: | |
| Granola Bar, Quaker Oats 90 calorie, Assorted | 1 bar |
| Granola Bar, Other Type: | 1 bar |
| Unhealthy Supplier Network (n = 41) | ||||
| All Suppliers | All Suppliers—Deliverers | |||
| b (95% CI) | P | b (95% CI) | P | |
| Mean distance (km) | 0.018 (−0.008, 0.044) | 0.156 | 0.134 (−0.206, 0.474) | 0.422 |
| Accept WIC, yes | 1.315 (−1.656, 4.286) | 0.369 | 0.622 (−0.628, 1.873) | 0.313 |
| Accept SNAP, yes | −0.182 (−5.639, 5.275) | 0.946 | −0.864 (−3.140, 1.413) | 0.440 |
| Storeowner ethnicity | ||||
| African American | ref | ref | ref | ref |
| Asian/Hispanic | 0.295 (−3.417, 4.007) | 0.871 | 0.011 (−1.560, 1.581) | 0.989 |
| Time operating current store (years) | 0.169 (−0.017, 0.355) | 0.072 | 0.039 (−0.044, 0.122) | 0.339 |
| Time operating food stores (years) | 0.104 (−0.059, 0.267) | 0.198 | 0.002 (−0.069, 0.074) | 0.945 |
| No. of customers on average day | 0.004 (−0.006, 0.015) | 0.431 | 0.003 (−0.001, 0.007) | 0.148 |
| No. of non-family paid employees | 0.311 (−1.241,1.863) | 0.682 | 0.189 (−0.465, 0.842) | 0.555 |
| Healthy Supplier Network (n = 15) | ||||
| All Suppliers | All Suppliers—Deliverers | |||
| b (95% CI) | P | b (95% CI) | P | |
| No. of family member employees | 0.582 (−0.544, 1.708) | 0.295 | 0.078 (−0.409, 0.565) | 0.742 |
| Mean distance (km) | 0.041 (−0.047, 0.128) | 0.345 | −0.048 (−0.161, 0.065) | 0.391 |
| Accept WIC, yes | −0.287 (−1.086, 0.513) | 0.465 | −0.224 (−0.926, 0.479) | 0.516 |
| Accept SNAP, yes | −1.864 (−3.067, −0.660) | 0.004 | −1.455 (−2.560, −0.349) | 0.012 |
| Storeowner ethnicity | ||||
| African American | ref | ref | ref | ref |
| Asian/Hispanic | −1.526 (−2.255, −0.798) | <0.001 | −1.432 (−2.029, −0.834) | <0.001 |
| Time operating current store (years) | −0.006 (−0.060, 0.048) | 0.818 | −0.023 (−0.069, 0.022) | 0.302 |
| Time operating food stores (years) | −0.028 (−0.016, 0.071) | 0.196 | 0.015 (−0.024, 0.054) | 0.426 |
| No. of customers on average day | 0.000 (−0.003, 0.002) | 0.777 | 0.000 (−0.003, 0.002) | 0.645 |
| No. of non-family paid employees | 0.077 (−0.337, 0.493) | 0.701 | 0.044 (−0.320, 0.409) | 0.803 |
| No. of family member employees | 0.019 (−0.289, 0.328) | 0.898 | 0.041 (−0.229, 0.311) | 0.758 |
References
- Drewnowski, A.; Rehm, C.D. Energy intakes of US children and adults by food purchase location and by specific food source. Nutr. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Adjoian, T.; Dannefer, R.; Sacks, R.; van Wye, G. Comparing sugary drinks in the food retail environment in six NYC neighborhoods. J. Community Health 2013, 39, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Laska, M.N.; Borradaile, K.E.; Tester, J.; Foster, G.D.; Gittelsohn, J. Healthy food availability in small urban food stores: A comparison of four US cities. Public Health Nutr. 2010, 13, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, H.; Suratkar, S.; Song, H.J.; Stauffer, E.; Gittelsohn, J. Access to food source and food source use are associated with healthy and unhealthy food-purchasing behaviours among low-income African-American adults in Baltimore City. Public Health Nutr. 2011, 14, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Auld, M.C.; Chaloupka, F.J.; O’Malley, P.M.; Johnston, L.D. Associations between access to food stores and adolescent body mass index. Am. J. Prev. Med. 2007, 33, S301–S307. [Google Scholar] [CrossRef] [PubMed]
- Cummins, S. Food environments and obesity—Neighbourhood or nation? Int. J. Epidemiol. 2005, 35, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 2012, 307, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vinicor, F.; Bales, V.S.; Marks, J.S. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Must, A.; Spadano, J.; Coakley, E.H.; Field, A.E.; Colditz, G.; Dietz, W.H. The disease burden associated with overweight and obesity. JAMA 1999, 282, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Heuer, C.A. Obesity stigma: Important considerations for public health. Am. J. Public Health 2010, 100, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Odoms-Young, A.M.; Dallas, C.; Hardy, E.; Watkins, A.; Hoskins-Wroten, J.; Holland, L. “You have to hunt for the fruits, the vegetables”: Environmental barriers and adaptive strategies to acquire food in a low-income African American neighborhood. Health Educ. Behav. 2011, 38, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Obesity and the food environment: Dietary energy density and diet costs. Am. J. Prev. Med. 2004, 27, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Diez Roux, A.V.; Nettleton, J.A.; Lazo, M.; Brancati, F.; Caballero, B.; Glass, T.; Moore, L.V. Availability of healthy foods and dietary patterns: The multi-ethnic study of atherosclerosis. Am. J. Clin. Nutr. 2009, 89, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood environments: Disparities in access to healthy foods in the US. Am. J. Prev. Med. 2009, 36, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Song, H.J.; Suratkar, S.; Kumar, M.B.; Henry, E.G.; Sharma, S.; Mattingly, M.; Anliker, J.A. An urban food store intervention positively affects food-related psychosocial variables and food behaviors. Health Educ. Behav. 2010, 37, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Suratkar, S.; Song, H.J.; Sacher, S.; Rajan, R.; Rasooly, I.R.; Bednarek, E.; Sharma, S.; Anliker, J.A. Process evaluation of Baltimore healthy stores: A pilot health intervention program with supermarkets and corner stores in Baltimore City. Health Promot. Pract. 2010, 11, 723–732. [Google Scholar] [CrossRef] [PubMed]
- LiveWell Colorado 2009 Annual Report. Available online: https://livewellcolorado.org/uploads/files/2013_04_01_21_42_31_lwc_annualreport2009_0.pdf (accessed on 23 January 2015).
- Healthy Bodegas Initiative: A Program of the Department of Health and Mental Hygiene. Available online: http://www.nyc.gov/html/ceo/downloads/pdf/BH_PRR.pdf (accessed on 23 January 2015).
- Samuels, S.E.; Craypo, L.; Boyle, M.; Crawford, P.B.; Yancey, A.; Flores, G. The California endowment’s healthy eating, active communities program: A midpoint review. Am. J. Public Health 2010, 100, 2114–2123. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Anderson Steeves, E.; Mui, Y.; Kharmats, A.Y.; Hopkins, L.C.; Dennis, D. B’More healthy communities for kids: Design of a multi-level intervention for obesity prevention for low-income African American children. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Baquero, B.; Laraia, B.A.; Ji, M.; Linnan, L. Efficacy of a store-based environmental change intervention compared with a delayed treatment control condition on store customers’ intake of fruits and vegetables. Public Health Nutr. 2013, 16, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Rowan, M.; Gadhoke, P. Interventions in small food stores to change the food environment, improve diet, and reduce risk of chronic disease. Prev. Chronic Dis. 2012, 9. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Mui, Y.; Adam, A.; Lin, S.; Kharmats, A.; Igusa, T.; Lee, B.Y. Incorporating systems science principles into the development of obesity prevention interventions: Principles, benefits, and challenges. Curr. Obes. Rep. 2015, 4, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Luke, D.A.; Stamatakis, K.A. Systems science methods in public health: Dynamics, networks, and agents. Annu. Rev. Public Health 2012, 33, 357–376. [Google Scholar] [CrossRef] [PubMed]
- Andreyeva, T.; Middleton, A.E.; Long, M.W.; Luedicke, J.; Schwartz, M.B. Food retailer practices, attitudes and beliefs about the supply of healthy foods. Public Health Nutr. 2011, 14, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Budd, N.; Cuccia, A.; Jeffries, J.K.; Prasad, D.; Frick, K.D.; Powell, L.; Katz, F.A.; Gittelsohn, J. B’More healthy: Retail rewards—Design of a multi-level communications and pricing intervention to improve the food environment in Baltimore City. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. State & County Quickfacts: Baltimore, MD, USA. Available online: http://quickfacts.census.gov/qfd/states/24/24510.html (accessed on 7 April 2015).
- Office of Epidemiology and Planning, Baltimore City Health Department. Baltimore City Health Disparities Report Card, 2010; Baltimore City Health Department: Baltimore, MD, USA, 2010.
- Franco, M.; Diez Roux, A.V.; Glass, T.A.; Caballero, B.; Brancati, F.L. Neighborhood characteristics and availability of healthy foods in Baltimore. Am. J. Prev. Med. 2008, 35, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Dennisuk, L.A.; Christiansen, K.; Bhimani, R.; Johnson, A.; Alexander, E.; Lee, M.; Lee, S.H.; Rowan, M.; Coutinho, A.J. Development and implementation of Baltimore healthy eating zones: A youth-targeted intervention to improve the urban food environment. Health Educ. Res. 2013, 28, 732–744. [Google Scholar] [CrossRef] [PubMed]
- Occupational Safety and Health Administration, United States Department of Labor. Standard Industrial Classification Division Structure: Food Stores. Available online: https://www.osha.gov/pls/imis/sic_manual.html (accessed on 3 March 2014).
- Borgatti, S.P.; Mehra, A.; Brass, D.J.; Labianca, G. Network analysis in the social sciences. Science 2009, 323, 892–895. [Google Scholar] [CrossRef] [PubMed]
- Luke, D.A.; Harris, J.K. Network analysis in public health: History, methods, and applications. Annu. Rev. Public Health 2007, 28, 69–93. [Google Scholar] [CrossRef] [PubMed]
- Bettinger, J.A.; Adler, N.E.; Curriero, F.C.; Ellen, J.M. Risk perceptions, condom use, and sexually transmitted diseases among adolescent females according to social network position. Sex. Transm. Dis. 2004, 31, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F. Assessing the physical health effects of social networks and social support. Annu. Rev. Public Health 1984, 5, 413–432. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Price, R.H.; Wortman, C.B. Social-factors in psychopathology—Stress, social support, and coping processes. Annu. Rev. Psychol. 1985, 36, 531–572. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.Y.; McGlone, S.M.; Song, Y.; Avery, T.R.; Eubank, S.; Chang, C.C.; Bailey, R.R.; Wagener, D.K.; Burke, D.S.; Platt, R.; et al. Social network analysis of patient sharing among hospitals in Orange County, California. Am. J. Public Health 2011, 101, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Lurie, S.J.; Fogg, T.T.; Dozier, A.M. Social network analysis as a method of assessing institutional culture: Three case studies. Acad. Med. 2009, 84, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Kapucu, N. Interorganizational coordination in dynamic context: Networks in emergency response management. Connections 2005, 26, 33–48. [Google Scholar]
- Krauss, M.; Mueller, N.; Luke, D. Interorganizational Relationships within State Tobacco Control Networks: A Social Network Analysis. Available online: http://www.cdc.gov/pcd/issues/2004/oct/04_0041.htm (accessed on 25 November 2015).
- De Nooy, W.; Mrvar, A.; Batagelj, V. Exploratory Social Network Analysis with Pajek, 2nd ed.; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Leung, C.W.; Ding, E.L.; Catalano, P.J.; Villamor, E.; Rimm, E.B.; Willett, W.C. Dietary intake and dietary quality of low-income adults in the Supplemental Nutrition Assistance Program. Am. J. Clin. Nutr. 2012, 96, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Whaley, S.E.; Ritchie, L.D.; Spector, P.; Gomez, J. Revised WIC food package improves diets of WIC families. J. Nutr. Educ. Behav. 2012, 44, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Franceschini, M.C.T.; Rasooly, I.R.; Ries, A.V.; Ho, L.S.; Pavlovich, W.; Santos, V.T.; Jennings, S.M.; Frick, K.D. Understanding the food environment in a low-income urban setting: Implications for food store interventions. J. Hunger Environ. Nutr. 2008, 2, 33–50. [Google Scholar] [CrossRef]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Hendrickson, D.; Smith, C.; Eikenberry, N. Fruit and vegetable access in four low-income food deserts communities in Minnesota. Agric. Hum. Values 2006, 23, 371–383. [Google Scholar] [CrossRef]
- Bassuk, E.L.; Buckner, J.C.; Weinreb, L.F.; Browne, A.; Bassuk, S.S.; Dawson, R.; Perloff, J.N. Homelessness in female-headed families: Childhood and adult risk and protective factors. Am. J. Public Health 1997, 87, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Pirog, R.; Harper, A.; Gerencer, M.; Lelle, M.; Gerencer, C. The Michigan Food Hub Network: A Case Study in Building Effective Networks for Food Systems Change; MSU Center for Regional Food Systems: Cambridge, UK, 2014. [Google Scholar]
- The Food Trust for the Healthy Corner Stores Network. Healthy Corner Stores Issue Brief: The Supplier-Retailer Gap: Connecting Corner Stores with Local Foods. Available online: http://thefoodtrust.org/uploads/media_items/winter2012issuebrief.original.pdf (accessed on 12 March 2014).
- Song, H.J.; Gittelsohn, J.; Kim, M.; Suratkar, S.; Sharma, S.; Anliker, J. Korean American storeowners’ perceived barriers and motivators for implementing a corner store-based program. Health Promot. Pract. 2011, 12, 472–482. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mui, Y.; Lee, B.Y.; Adam, A.; Kharmats, A.Y.; Budd, N.; Nau, C.; Gittelsohn, J. Healthy versus Unhealthy Suppliers in Food Desert Neighborhoods: A Network Analysis of Corner Stores’ Food Supplier Networks. Int. J. Environ. Res. Public Health 2015, 12, 15058-15074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph121214965
Mui Y, Lee BY, Adam A, Kharmats AY, Budd N, Nau C, Gittelsohn J. Healthy versus Unhealthy Suppliers in Food Desert Neighborhoods: A Network Analysis of Corner Stores’ Food Supplier Networks. International Journal of Environmental Research and Public Health. 2015; 12(12):15058-15074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph121214965
Chicago/Turabian StyleMui, Yeeli, Bruce Y. Lee, Atif Adam, Anna Y. Kharmats, Nadine Budd, Claudia Nau, and Joel Gittelsohn. 2015. "Healthy versus Unhealthy Suppliers in Food Desert Neighborhoods: A Network Analysis of Corner Stores’ Food Supplier Networks" International Journal of Environmental Research and Public Health 12, no. 12: 15058-15074. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph121214965