
A Scoping Review of Maternal and Child Health Clinicians Attitudes, Beliefs, Practice, Training and Perceived Self-Competence in Environmental Health

Abstract
:1. Introduction
Purpose of Review
- The attitudes and beliefs of maternal and child health clinicians in environmental health
- The state of environmental health assessment by these clinicians in their routine practice
- Maternal and child health clinicians’ perspectives about their self-competence in managing environmental hazard(s) associated with health problems
- Maternal and child health clinicians’ challenges to the inclusion of environmental health in routine clinical practice.
2. Methods
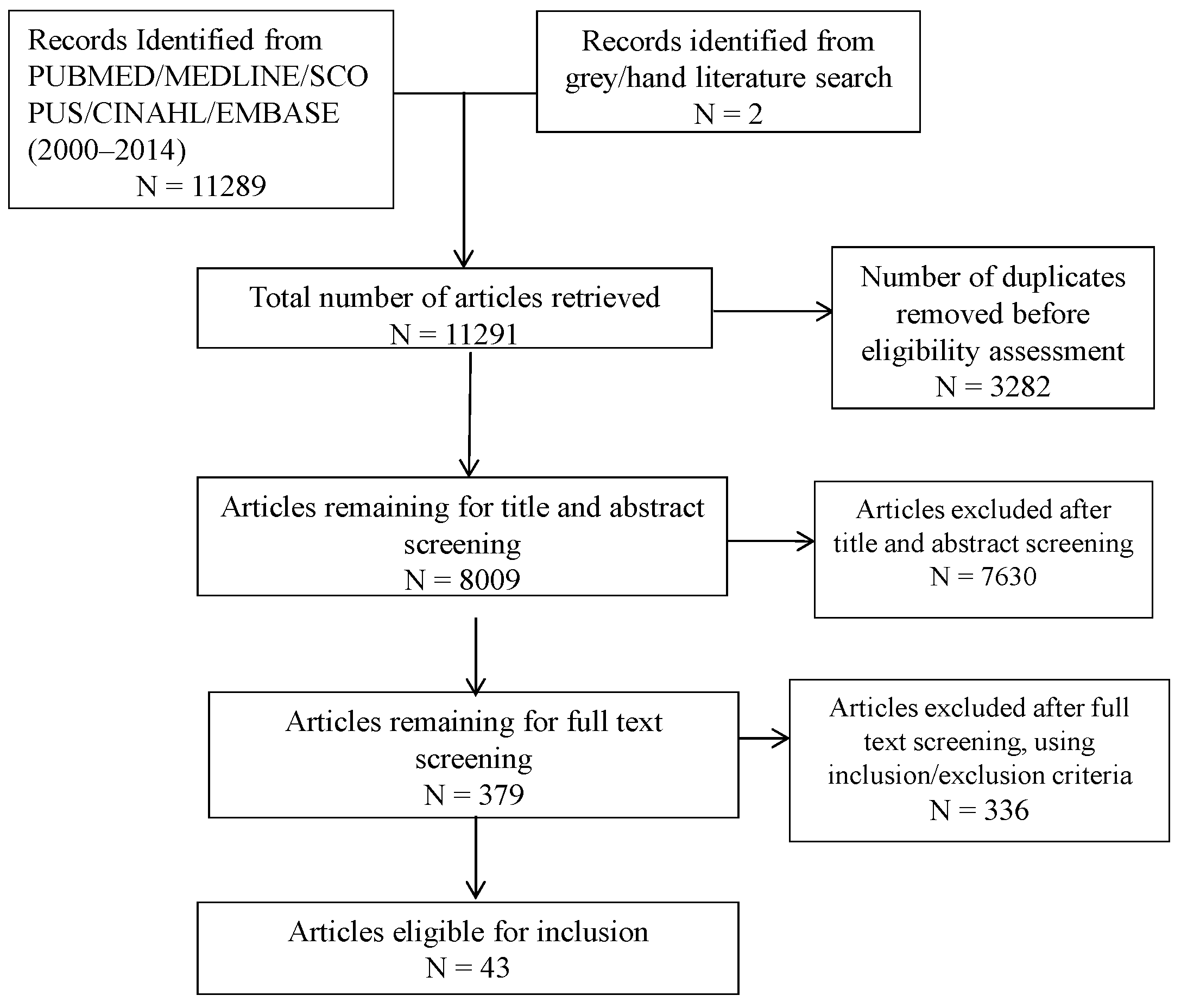
2.1. Search Strategies
2.2. Study Selection
- English articles published between 2000 and 2014.
- Any geographic location.
- Empirical study conducted on trained and practicing clinicians including general, family and primary care physicians, obstetricians, pediatricians, midwives and nurses.
- Clinicians must be primarily attending to clients in a clinical setting.
- Studies assessing competence, attitude, belief, opinions, practice, education and/or training in environmental health and/or in environmental exposures.
- Examines at least one environmental health hazard exposure.
- Studies that only describe clinicians’ non-clinical practice personal behavior to reduce risk of environmental exposure (e.g., personal smoking behavior).
- Opinions, commentaries, editorials, viewpoints, letters and notes.
- Studies describing only specialist occupational health clinicians and/or public health workers whose practice is not in a clinical setting.
2.3. Data Extraction, Collation and Reporting
Attitudes and beliefs of clinicians
|
Clinician practice patterns
|
Clinician self-rated competence
|
Clinician training
|
| Challenges towards the inclusion of environmental health assessment in routine clinical practice |
3. Results


{kind=link}
| Study Author (s) | Author(s) Number | Study Location | Pediatrician | Nurses | More than 1 Type of Clinician | Others |
|---|---|---|---|---|---|---|
| [19] | 1 | U. S. A | √ | |||
| [20] | 2 | Tanzania | √ | |||
| [21] | 3 | U. S. A | √ | |||
| [22] | 4 | U. S. A | √ | |||
| [23] | 5 | Thailand | √ a | |||
| [24] | 6 | U. S. A | √ | |||
| [25] | 7 | U. S. A | √ | |||
| [26] | 8 | U. S. A | √ | |||
| [27] | 9 | Germany | √ | |||
| [28] | 10 | Bangladesh | √ | |||
| [29] | 11 | U. S. A | √ | |||
| [30] | 12 | U. K | √ | |||
| [31] | 13 | U. S. A | √ a | |||
| [32] | 14 | U. S. A | √ a | |||
| [33] | 15 | Germany | √ b | |||
| [34] | 16 | U. S. A | √ | |||
| [35] | 17 | Canada | √ | |||
| [36] | 18 | U. S. A | √ | |||
| [37] | 19 | U. S. A | √ | |||
| [38] | 20 | Italy | √ a | |||
| [39] | 21 | U. S. A | √ | |||
| [40] | 22 | U. S. A | √ | |||
| [41] | 23 | U. S. A | √ b | |||
| [42] | 24 | U. S. A | √ | |||
| [43] | 25 | U. S. A | √ | |||
| [44] | 26 | Canada | √ | |||
| [45] | 27 | New Zealand | √ | |||
| [46] | 28 | Pakistan | √ a | |||
| [47] | 29 | U. S. A | √ | |||
| [48] | 30 | Sweden | √ | |||
| [49] | 31 | U. S. A | √ | |||
| [50] | 32 | Bahrain | √ a | |||
| [51] | 33 | Germany | √ a | |||
| [52] | 34 | Argentina | √ | |||
| [17] | 35 | U. A. E | √ | |||
| [18] | 36 | U. S. A | √ | |||
| [53] | 37 | Egypt | √ | |||
| [54] | 38 | China | √ a | |||
| [55] | 39 | U. S. A | √ | |||
| [56] | 40 | U. S. A | √ | |||
| [15] | 41 | U. S. A | √ | |||
| [16] | 42 | U. S. A | √ c | |||
| [57] | 43 | China | √ | |||
| Total | 12 | 6 | 14 | 11 |
| Author # | Type of Environmental Hazard Assessed | |||||
|---|---|---|---|---|---|---|
| Tobacco | Pesticides | Lead | Mold | Other Metal(s) | Other Hazard(s) | |
| 1 | √ | √ | √ | |||
| 2 | √ a | |||||
| 3 | √ | √ | √ | |||
| 4 | √ a | |||||
| 5 | √ | |||||
| 6 | √ | |||||
| 7 | √ | √ | √ | √ | ||
| 8 | √ a | |||||
| 9 | √ a | |||||
| 10 | √ a | |||||
| 11 | √ a | |||||
| 12 | √ a | |||||
| 13 | √ | √ | √ | √ | √ | |
| 14 | √ a | |||||
| 15 | √ a | |||||
| 16 | √ a | |||||
| 17 | √ | √ | √ | √ | √ | |
| 18 | √ | √ | ||||
| 19 | √ a | |||||
| 20 | √ | √ | √ | |||
| 21 | √ | √ | √ | |||
| 22 | √ | √ | √ | √ | √ | √ |
| 23 | √ a | |||||
| 24 | √ a | |||||
| 25 | √ a | |||||
| 26 | √ | √ | √ | √ | √ | |
| 27 | √ a | |||||
| 28 | √ a | |||||
| 29 | √ | √ | √ | |||
| 30 | √ a | |||||
| 31 | √ a | |||||
| 32 | √ a | |||||
| 33 | √ a | |||||
| 34 | √ a | |||||
| 35 | √ a | |||||
| 36 | √ | √ | √ | √ | √ | √ |
| 37 | √ | √ | √ | √ | ||
| 38 | √ a | |||||
| 39 | √ a | |||||
| 40 | √ | √ | √ | |||
| 41 | √ a | |||||
| 42 | √ | √ | √ | √ | √ | √ |
| 43 | √ | √ | √ | √ | √ | √ |
| Total # of Studies # of studies on single hazard | 30 17 | 12 3 | 10 0 | 10 0 | 12 2 | 20 3 |
3.1. Clinicians’ Attitudes and Beliefs
3.2. Practices
3.3. Self-Assessed Competencies and Training
3.4. Challenges to Practice
| Categories | # of Articles | Hazard Exposure | ||
|---|---|---|---|---|
| Tobacco Smoke # of Articles a | Tobacco Smoke + Other Exposures a | Other Exposures (Not Including Tobacco Smoke) a | ||
| Attitudes and Beliefs | 25 | |||
| Environmental exposure(s) affect(s) human health | 20 | 3 (3) | 9 (9) | 8 (7) |
| Environmental health history taking should be part of routine practice | 11 | 0 (0) | 8 (8) | 3 (1) |
| Counselling of patients on Environmental exposures can help reduce exposures | 15 | 6 (5) | 6 (4) | 3 (3) |
| Practices | 30 | |||
| Clinician takes routine environmental exposure history | 24 | 12 (8) | 9 (6) | 3 (0) |
| Includes environmental exposure counselling in routine practice | 21 | 14 (10) | 5 (4) | 2 (0) |
| Refers/would refer cases associated with environmental exposures to specialists | 8 | 3 (0) | 4 (4) | 1 (1) |
| Competence/Training | 35 | |||
| Sufficiently informed on environmental exposures | 21 | 6 (2) | 9 (5) | 6 (1) |
| Prior training in environmental health history taking | 21 | 8 (2) | 6 (0) | 7 (1) |
| Requires/interested in more training | 16 | 6 (6) | 4 (4) | 6 (5) |
4. Discussion
4.1. Study Limitations
4.2. Future Studies
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO. Children’s Environmental Health Units; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Trasande, L.; Liu, Y. Reducing the staggering costs of environmental disease in children, estimated at $76.6 billion in 2008. Health Aff. 2011, 30, 863–870. [Google Scholar]
- CDC. Protecting Kids from Environmental Exposure. Available online: http://www.cdc.gov/features/pehsu/ (accessed on 3 December 2015).
- Reed, M.S. Stakeholder participation for environmental management: A literature review. Biol. Conserv. 2008, 141, 2417–2431. [Google Scholar] [CrossRef]
- Brown, P.; Morello-Frosch, R.; Zavestoski, S. Contested Illnesses: Citizens, Science, and Health Social Movements; University of California Press: Berkeley, CA, USA, 2012. [Google Scholar]
- World Medical Association. WMA Statement on Environmental Degradation and Sound Management of Chemicals; World Medical Association: Ferney-Voltaire, France, 2010. [Google Scholar]
- ICN. Reducing Environmental and Lifestyle Related Health Risks; ICN: Geneva, Switzerland, 2011. [Google Scholar]
- World Federation of Public Health Associations. The Kolkata Call to Action; World Federation of Public Health Associations: Geneva, Switzerland, 2011. [Google Scholar]
- Institute of Medicine (US) Committee on Enhancing Environmental Health Content in Nursing Practice. Nursing, Health, the Environment: Strengthening the Relationship to Improve the Public’s Health; National Academies Press: Washington, DC, USA, 1996. [Google Scholar]
- Centers for Disease Control and Prevention. Environmental Health Competency Project: Recommendations for Core Competencies for Local Environmental Health Practitioners; Centers for Disease Control and Prevention: DeKalb County, GA, USA, 2001. [Google Scholar]
- Institut National De Santé Publique Du Québec. Environmental Health Competency Framework for Public Health in Quebec; Institut National De Santé Publique Du Québec: Québec, Canada, 2013. [Google Scholar]
- Gehle, K.S.; Crawford, J.L.; Hatcher, M.T. Integrating environmental health into medical education. Am. J. Prev. Med. 2011, 41, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Casas, M.; Bergstrom, A.; Carmichael, A.; Cordier, S.; Eggesbo, M.; Eller, E.; Fantini, M.P.; Fernandez, M.F.; Fernandez-Somoano, A.; et al. European birth cohorts for environmental health research. Environ. Health Perspect. 2012, 120, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centre for Addiction and Mental Health. Canadian Action Network for the Advancement, Dissemination and Adoption of Practice-informed Tobacco Treatment; Centre for Addiction and Mental Health: Toronto, Canada, 2011. [Google Scholar]
- Blaine, K.; Rogers, J.; Winickoff, J.P.; Oppenheimer, S.C.; Timm, A.; Ozonoff, A.; Geller, A.C. Engaging in secondhand smoke reduction discussions with parents of hospitalized pediatric patients: A national survey of pediatric nurses in the United States. Prev. Med. 2014, 62, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Stotland, N.E.; Sutton, P.; Trowbridge, J.; Atchley, D.S.; Conry, J.; Trasande, L.; Gerbert, B.; Charlesworth, A.; Woodruff, T.J. Counseling patients on preventing prenatal environmental exposures—A mixed-methods study of obstetricians. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Sreedharan, J.; Muttappallymyalil, J.; Venkatramana, M. Nurses’ attitude and practice in providing tobacco cessation care to patients. J. Prev. Med. Hyg. 2010, 51, 57–61. [Google Scholar] [PubMed]
- Trasande, L.; Newman, N.; Long, L.; Howe, G.; Kerwin, B.J.; Martin, R.J.; Gahagan, S.A.; Weil, W.B. Translating knowledge about environmental health to practitioners: Are we doing enough? Mt. Sinai. J. Med. 2010, 77, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Chai, S.K.; Robertson, W.O.; Takaro, T.; Hagopian, A.; Beaudet, N.; Sechena, R.; Martin, T.; Simpson, L.; Barnhart, S. Pediatric environmental health: Perceptions from a survey questionnaire. Int. J. Occup. Environ. Health 2001, 7, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Ngowi, A.V.; Maeda, D.N.; Partanen, T.J. Assessment of the ability of health care providers to treat and prevent adverse health effects of pesticides in agricultural areas of Tanzania. Int. J. Occup. Med. Environ. Health 2001, 14, 349–356. [Google Scholar] [PubMed]
- Woolf, A.; Cimino, S. Environmental illness: Educational needs of pediatric care providers. Ambul. Child Health 2001, 7, 43–51. [Google Scholar] [CrossRef]
- Perez-Stable, E.J.; Juarez-Reyes, M.; Kaplan, C.; Fuentes-Afflick, E.; Gildengorin, V.; Millstein, S. Counseling smoking parents of young children: Comparison of pediatricians and family physicians. Arch. Pediatr. Adolesc. Med. 2001, 155, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Aekplakorn, W.; Suriyawongpaisal, P.; Methawikul, T. The diagnosis and reporting of occupational diseases: The performance of physicians in Thailand. Southeast Asian J. Trop. Med. Public Health 2002, 33, 188–192. [Google Scholar] [PubMed]
- Van Dongen, C.J. Environmental health and nursing practice: A survey of registered nurses. Appl. Nurs. Res. 2002, 15, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, N.; Frumkin, H.; Trowbridge, J.; Escoffery, C.; Geller, R.; Rubin, L.; Teague, G.; Nodvin, J. The environmental history in pediatric practice: A study of pediatricians’ attitudes, beliefs, and practices. Environ. Health Perspect. 2002, 110, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Cabana, M.D.; Rand, C.; Slish, K.; Nan, B.; Davis, M.M.; Clark, N. Pediatrician self-efficacy for counseling parents of asthmatic children to quit smoking. Pediatrics 2004, 113, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Hannöver, W.; Thyrian, J.R.; John, U. Short report: Paediatricians’ attitude towards counselling parents postpartum about their smoking behaviour. Eur. J. Public Health 2004, 14, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Murshed, R.; Douglas, R.M.; Ranmuthugala, G.; Caldwell, B. Clinicians’ roles in management of arsenicosis in Bangladesh: Interview study. BMJ 2004, 328, 493–494. [Google Scholar] [CrossRef] [PubMed]
- Balk, S.J.; O’Connor, K.G.; Saraiya, M. Counseling parents and children on sun protection: A national survey of pediatricians. Pediatrics 2004, 114, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Stevens, E.; Cullinan, P.; Colvile, R. Urban air pollution and children’s asthma: What do parents and health professionals think? Pediatr. Pulmonol. 2004, 37, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, W.J.; Ryder, D.J.; Cooper, H.P.; Williams, D.M.; Weinberg, A.D. Environmental health: A survey of Texas primary care physicians. Tex. Med. 2005, 101, 62–70. [Google Scholar] [PubMed]
- Soto, M.F.G.; Papenfuss, R.L.; Jacobson, H.E.; Hsu, C.E.; Urrutia-Rojas, X.; Kane, W.M. Hispanic physicians’ tobacco intervention practices: A cross-sectional survey study. BMC Public Health 2005, 5. [Google Scholar] [CrossRef]
- Thyrian, J.R.; Hannöver, W.; Röske, K.; Scherbarth, S.; Hapke, U.; John, U. Midwives’ attitudes to counselling women about their smoking behaviour during pregnancy and postpartum. Midwifery 2006, 22, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Balbus, J.M.; Harvey, C.E.; McCurdy, L.E. Educational needs assessment for pediatric health care providers on pesticide toxicity. J. Agromedicine 2006, 11, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Buka, I.; Rogers, W.T.; Osornio-Vargas, A.R.; Hoffman, H.; Pearce, M.; Li, Y.Y. An urban survey of paediatric environmental health concerns: Perceptions of parents, guardians and health care professionals. Paediatr. Child Health 2006, 11, 235–238. [Google Scholar] [PubMed]
- Hu, Y.Y.; Adams, R.E.; Boscarino, J.A.; Laraque, D. Training needs of pediatricians facing the environmental health and bioterrorism consequences of September 11th. Mt. Sinai. J. Med. 2006, 73, 1156–1164. [Google Scholar] [PubMed]
- Karr, C.; Murphy, H.; Glew, G.; Keifer, M.C.; Fenske, R.A. Pacific Northwest health professionals survey on pesticides and children. J. Agromedicine 2006, 11, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Nicotera, G.; Nobile, C.G.; Bianco, A.; Pavia, M. Environmental history-taking in clinical practice: Knowledge, attitudes, and practice of primary care physicians in Italy. J. Occup. Environ. Med. 2006, 48, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Trasande, L.; Schapiro, M.L.; Falk, R.; Haynes, K.A.; Behrmann, A.; Vohmann, M.; Stremski, E.S.; Eisenberg, C.; Evenstad, C.; Anderson, H.A.; et al. Pediatrician attitudes, clinical activities, and knowledge of environmental health in Wisconsin. WMJ 2006, 105, 45–49. [Google Scholar] [PubMed]
- Trasande, L.; Boscarino, J.; Graber, N.; Falk, R.; Schechter, C.; Galvez, M.; Dunkel, G.; Geslani, J.; Moline, J.; Kaplan-Liss, E.; et al. The environment in pediatric practice: A study of New York pediatricians’ attitudes, beliefs, and practices towards children’s environmental health. J. Urban Health 2006, 83, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Abatemarco, D.J.; Steinberg, M.B.; Delnevo, C.D. Midwives’ knowledge, perceptions, beliefs, and practice supports regarding tobacco dependence treatment. J. Midwifery Women Health 2007, 52, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.N.; Levin, K.P.; Bryant-Stephens, T. Pediatricians’ practices and attitudes about environmental tobacco smoke and parental smoking. J. Pediatr. 2007, 150, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Serwint, J.R.; Higman, S.; Kanof, A.; Schell, D.; Colon, I.; Butz, A.M. Self-efficacy for smoking cessation counseling parents in primary care: An office-based intervention for pediatricians and family physicians. Clin. Pediatr. 2007, 46, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Canadian Nurses Association. Nurses and Environmental Health: Survey Results; Canadian Nurses Association: Ottawa, Canada, 2008. [Google Scholar]
- Glover, M.; Paynter, J.; Bullen, C.; Kristensen, K. Supporting pregnant women to quit smoking: Postal survey of New Zealand general practitioners and midwives’ smoking cessation knowledge and practices. N. Z. Med. J. 2008, 121, 53–65. [Google Scholar] [PubMed]
- Rafique, M.; Jabeen, S.; Shahzad, M.I. General public’s and physicians’ perception of health risk associated with radon exposure in the state of Azad Jammu and Kashmir. Public Health Nurs. 2008, 25, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Trasande, L.; Ziebold, C.; Schiff, J.S.; Wallinga, D.; McGovern, P.; Oberg, C.N. The role of the environment in pediatric practice in Minnesota: Attitudes, beliefs, and practices. Minn. Med. 2008, 91, 36–39. [Google Scholar] [PubMed]
- Carlsson, N.; Johansson, A.; Hermansson, G.; Andersson-Gare, B. Child health nurses’ roles and attitudes in reducing children’s tobacco smoke exposure. J. Clin. Nurs. 2010, 19, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Deckter, L.; Mahabee-Gittens, E.M.; Gordon, J.S. Are pediatric ED nurses delivering tobacco cessation advice to parents? J. Emerg. Nurs. 2009, 35, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Fadhil, I. Tobacco education in medical schools: Survey among primary care physicians in Bahrain. East Mediterr. Health J. 2009, 15, 969–975. [Google Scholar] [PubMed]
- Kowall, B.; Breckenkamp, J.; Heyer, K.; Berg-Beckhoff, G. German wide cross sectional survey on health impacts of electromagnetic fields in the view of general practitioners. Int. J. Public Health 2010, 55, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Mejia, R.; Martinez, V.G.; Gregorich, S.E.; Perez-Stable, E.J. Physician counseling of pregnant women about active and secondhand smoking in Argentina. Acta. Obstet. Gynecol. Scand. 2010, 89, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Abbas, R.A.; Alghobashy, A.A. Effect of an environmental health educational programme for paediatricians in an Egyptian university hospital: Before and after study. JRSM Short Rep. 2012, 3. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Guo, C.; Yu, S.; Feng, Y.; Song, J.; Erikson, M.; Redmon, P.; Koplan, J. Smoking behaviours and cessation services among male physicians in China: Evidence from a structural equation model. Tob. Control 2013, 22, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Kruger, J.; Trosclair, A.; Rosenthal, A.; Babb, S.; Rodes, R. Physician advice on avoiding secondhand smoke exposure and referrals for smoking cessation services. Tob. Induc. Dis. 2012, 10. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.R.; Karr, C.J.; de Ybarrondo, L.; McCurdy, L.E.; Freeland, K.D.; Hulsey, T.C.; Forman, J. Improving pediatrician knowledge about environmental triggers of asthma. Clin. Pediatr. 2013, 52, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Trasande, L.; Niu, J.; Li, J.; Liu, X.; Zhang, B.; Li, Z.; Ding, G.; Sun, Y.; Chen, M.; Hu, X.; et al. The environment and children’s health care in Northwest China. BMC Pediatr. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Agaku, I.T.; King, B.A.; Dube, S.R. Current cigarette smoking among adults—United States, 2005–2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 29–34. [Google Scholar] [PubMed]
- Bradshaw, M.J.; Lowenstein, A.J. Innovative Teaching Strategies in Nursing and Related Health Professions; Jones and Bartlett Publishers: Boston, MA, USA, 2011. [Google Scholar]
- Denny, B.; Chester, A.; Butler, M.; Brown, J. Australian GP registrars; use of e-resources. Educ. Prim. Care. 2015, 26, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Lindson-Hawley, N.; Thompson, T.P.; Begh, R. Motivational Interviewing for Smoking Cessation; Wiley: Malden, MA, USA, 2015. [Google Scholar]
- Edwards, N.; Semenic, S.; Premji, S.; Montgomery, P.; Williams, B.; Olson, J.; Mansi, O. Provincial prenatal record revision: A multiple case study of evidence-based decision-making at the population-policy level. BMC 2008, 8. [Google Scholar] [CrossRef] [PubMed]
- Semenic, S.; Edwards, N.; Premji, S.; Olson, J.; Williams, B.; Montgomery, P. Decision-making and evidence use during the process of prenatal record review in Canada: A multiphase qualitative study. BMC 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Eccles, M.; Grimshaw, J.; Shekelle, P.; Schünemann, H.J.; Woolf, S. Developing clinical practice guidelines: Target audiences, identifying topics for guidelines, guideline group composition and functioning and conflicts of interest. Implement. Sci. 2012, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Joas, R.; Casteleyn, L.; Biot, P.; Kolossa-Gehring, M.; Castano, A.; Angerer, J.; Schoeters, G.; Sepai, O.; Knudsen, L.E.; Joas, A.; et al. Harmonised human biomonitoring in Europe: Activities towards an EU HBM framework. Int. J. Hyg. Environ. Health 2012, 215, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Rochester, J.R. Bisphenol A and human health: A review of the literature. Reprod. Toxicol. 2013, 42, 132–155. [Google Scholar] [CrossRef] [PubMed]
- Lyche, J.L.; Rosseland, C.; Berge, G.; Polder, A. Human health risk associated with brominated flame-retardants (BFRs). Environ. Int. 2015, 74, 170–180. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massaquoi, L.D.; Edwards, N.C. A Scoping Review of Maternal and Child Health Clinicians Attitudes, Beliefs, Practice, Training and Perceived Self-Competence in Environmental Health. Int. J. Environ. Res. Public Health 2015, 12, 15769-15781. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph121215018
Massaquoi LD, Edwards NC. A Scoping Review of Maternal and Child Health Clinicians Attitudes, Beliefs, Practice, Training and Perceived Self-Competence in Environmental Health. International Journal of Environmental Research and Public Health. 2015; 12(12):15769-15781. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph121215018
Chicago/Turabian StyleMassaquoi, Lamin Daddy, and Nancy Christine Edwards. 2015. "A Scoping Review of Maternal and Child Health Clinicians Attitudes, Beliefs, Practice, Training and Perceived Self-Competence in Environmental Health" International Journal of Environmental Research and Public Health 12, no. 12: 15769-15781. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph121215018