
Parity and Risk of Death from Gallbladder Cancer among a Cohort of Premenopausal Parous Women in Taiwan

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
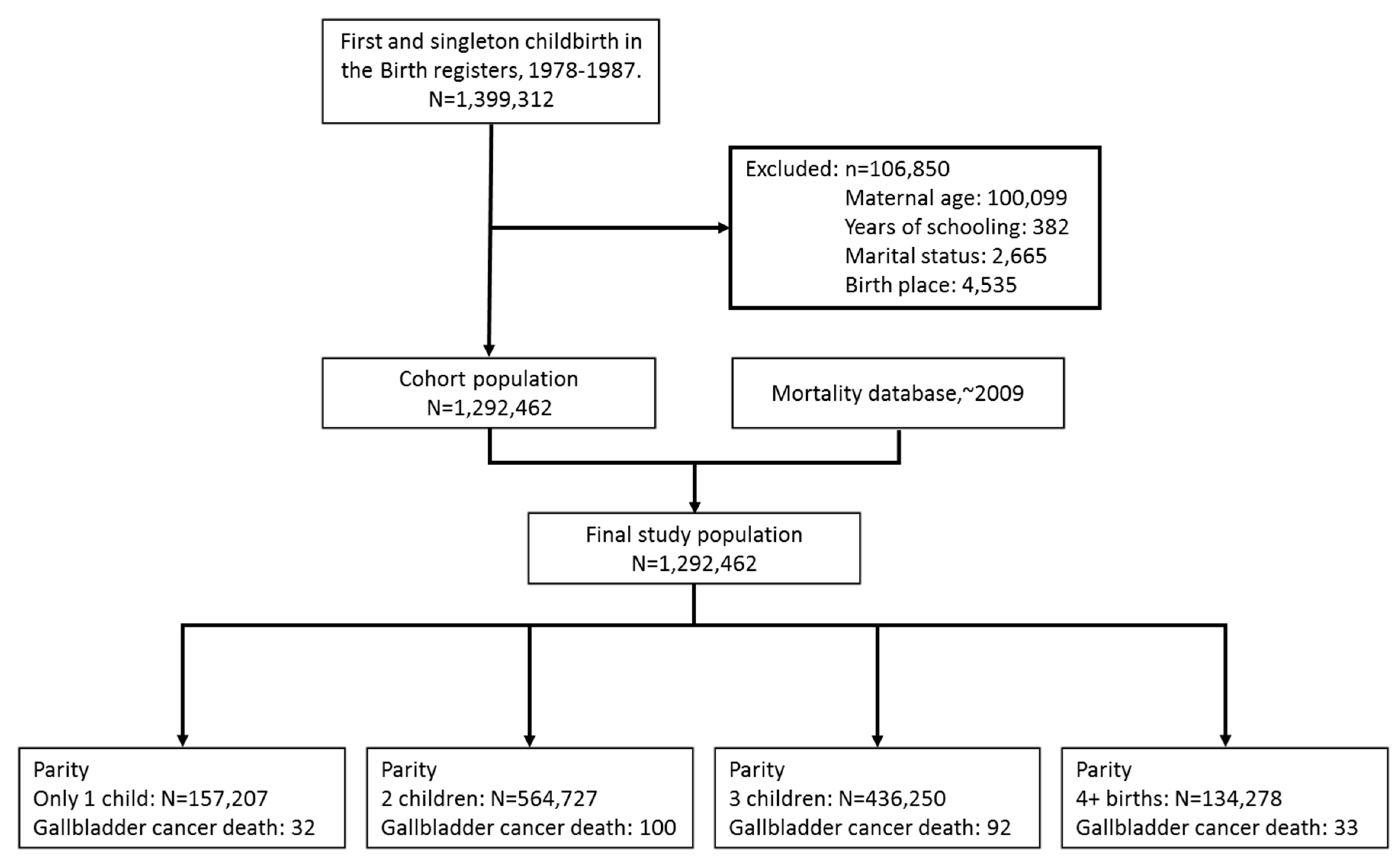
2.2. Study Population

2.3. Follow-Up
2.4. Statistics
3. Results

{kind=link}
| Parameters | Parity | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 (n = 157,207) | 2 (n = 564,727) | 3 (n = 436,250) | 4+ (n = 134,278) | ||||||
| Age at recruitment (1st birth) | 26.38 ± 4.43 | 24.86 ± 3.30 | 23.49 ± 2.95 | 22.44 ± 2.95 | <0.0001 | ||||
| Marital status | |||||||||
| Married | 146,022 | (92.89) | 554,810 | (98.24) | 429,239 | (98.39) | 130,544 | (97.22) | <0.0001 |
| Not married | 11,185 | (7.11) | 9917 | (1.76) | 7011 | (1.61) | 3734 | (2.78) | |
| Years of schooling | |||||||||
| ≤9 year | 72,090 | (45.86) | 258,361 | (45.75) | 285,737 | (65.50) | 106,330 | (79.19) | <0.0001 |
| >9 year | 85,117 | (54.14) | 306,366 | (54.25) | 150,513 | (34.50) | 27,948 | (20.81) | |
| Birth place | |||||||||
| Hospital/clinic | 153,167 | (97.43) | 553,930 | (98.09) | 416,492 | (95.47) | 122,336 | (91.11) | <0.0001 |
| Home/other | 4040 | (2.57) | 10,797 | (1.91) | 19,758 | (4.53) | 11,942 | (8.89) | |
| Parity | No. of Subjects | No. of Death from Gallbladder Cancer | Follow-Up Person-Years | Mortality Rate (Per 100,000 Person-Years) | Age-Adjusted Hazard Ratio (95% CI) | Multivariate-Adjusted Hazard Ratio * (95% CI) |
|---|---|---|---|---|---|---|
| 1 | 157207 | 32 | 4170772.33 | 0.77 | 1.00 | 1.00 |
| 2 | 564727 | 100 | 15124112.33 | 0.66 | 1.12 (0.75~1.69) | 1.20 (0.79~1.83) |
| 3 | 436250 | 92 | 11925297.25 | 0.77 | 1.53 (0.99~2.35) | 1.47 (0.95~2.29) |
| 4+ | 134278 | 33 | 3760064.08 | 0.88 | 1.90 (1.13~3.20) | 1.68 (0.99~2.85) |
| p = 0.0023 for linear trend | p = 0.0246 for linear trend |
4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Department of Health, Taiwan (ROC). Statistics of Causes of Death; Department of Health: Taipei, Taiwan, 2012. [Google Scholar]
- Hsing, A.W.; Rashid, A.; Devesa, S.S.; Fraumeni, J.F. Biliary tract cancer. In Cancer Epidemiology and Prevention; Schottenfeld, D., Fraumeni, J.F., Eds.; Oxford University Press: New York, NY, USA, 2006; pp. 787–800. [Google Scholar]
- Misra, S.; Chaturvedi, A.; Misra, N.C.; Sharma, I.D. Carcinoma of the gallbladder. Lancet Oncol. 2003, 4, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Randi, G.; Franceschi, S.; La Vecchia, C. Gallbladder cancer worldwide: Geographical distribution and risk factors. Int. J. Cancer 2006, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Lazcano-Ponce, E.C.; Miquel, J.F.; Munoz, N.; Herrero, R.; Ferrecio, C.; Wistuba, II. Epidemiology and molecular pathology of gallbladder cancer. CA Cancer J. Clin. 2001, 51, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Gourgiotis, S.; Kocher, H.M.; Solaini, L.; Yarollahi, A.; Tsiambas, E.; Salemis, N.S. Gallbladder cancer. Amer. J. Surg. 2008, 196, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, G.; Hou, L.; Gao, Y.T.; Brinton, L.A.; Rashid, A.; Chen, J. Reproductive factors and risks of biliary tract cancers and stones: A population-based study in Shanghai, China. Brit. J. Cancer 2010, 102, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Best, S.P.; Sali, A. Single and multiple cholesterol gallstones and the influence of bacteria. Med. Hypotheses 2000, 55, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Yen, S.S. Endocrinology of pregnancy. In Maternal-Fetal Medicine: Principles and Practice, 3rd ed.; Creasy, R.K., Resnik, R., Eds.; Saunders: Philadelphia, PA, USA, 1994; pp. 382–412. [Google Scholar]
- La Vecchia, C.; Negri, E.; Franceschi, S.; Parazzini, F. Long-term impact of reproductive factors on cancer risk. Int. J. Cancer 1993, 53, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Lambe, M.; Trichopoulos, D.; Hsieh, C.C.; Ekbom, A.; Adami, H.O.; Pavia, M. Parity and cancer of the gall bladder and the extrahepatic bile ducts. Int. J. Cancer 1993, 54, 941–944. [Google Scholar] [CrossRef] [PubMed]
- Moerman, C.J.; Berns, M.P.; Bueno de Mesquita, H.B.; Runia, S. Reproductive history and cancer of the biliary tract in women. Int. J. Cancer 1994, 57, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Pandey, M.; Shukla, V.K. Lifestyle, parity, menstrual and reproductive factors and risk of gallbladder cancer. Eur. J. Cancer Prev. 2003, 12, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Tavani, A.; Negri, E.; La Vecchia, C. Menstrual and reproductive factors and biliary tract cancer. Eur. J. Cancer Prev. 1996, 5, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Zatonski, W.A.; Lowenfels, A.B.; Boyle, P.; Maisonneuve, P.; de Mesquita, H.B.; Ghadirian, P. Epidemiologic aspects of gallbladder cancer: A case-control study of SEARCH program of the International Agency for Research on Cancer. J. Natl. Cancer Inst. 1997, 89, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Alvi, A.R.; Siddiqui, N.A.; Zafar, H. Risk factors of gallbladder cancer in Karachi-a case-control study. World J. Surg. Oncol. 2011, 9. [Google Scholar] [CrossRef]
- Wu, S.C.; Young, C.L. Study of the birth reporting system. J. Natl. Public Health Assoc. (ROC) 1986, 6, 15–27. [Google Scholar]
- Yang, C.Y.; Chang, C.C.; Kuo, H.W.; Chiu, H.F. Parity and risk of death from subarachnoid hemorrhage in women: Evidence from a cohort in Taiwan. Neurology 2006, 67, 514–515. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Kuo, H.W.; Chiu, H.F. Age at first birth, parity, and risk of death from ovarian cancer in Taiwan: A country of low incidence of ovarian cancer. Int. J. Gynecol. Cancer 2007, 17, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Chan, T.F.; Chien, C.C.; Yang, C.Y. Parity, age at first birth, and risk of death from liver cancer: Evidence from a cohort in Taiwan. J. Gastroenterol. Hepatol. 2011, 26, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.H.; Tsai, S.S.; Chen, C.C.; Ho, S.C.; Chiu, H.F.; Wu, T.N. Parity and risk of death from lung cancer among a cohort of premenopausal parous women in Taiwan. J. Epidemiol. 2012, 22, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S. Modern Epidemiology, 2nd ed.; Lippincott-Raven: Philadelphia, PA, USA, 1998. [Google Scholar]
- Kritz-Silverstein, D.; Barrett-Connor, E.; Wingard, D.L. The relation between reproductive history and cholecystectomy in older women. J. Clin. Epidemiol. 1990, 43, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Beral, V.; Balkwill, A. Childbearing, breastfeeding, other reproductive factors and the subsequent risk of hospitalization for gallbladder disease. Int. J. Epidemiol. 2009, 38, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Everson, G.T.; McKinley, C.; Lawson, M.; Johnson, M.; Kern, F. Gallbladder function in the human females: Effect of the ovulatory cycle, pregnancy, and contraceptive steroids. Gastroenterology 1982, 2, 711–719. [Google Scholar]
- Sanders, G.; Kingsnorth, A. Gallstones. Br. Med. J. 2007, 335, 295–299. [Google Scholar] [CrossRef]
- Ko, C.W.; Beresford, S.A.; Schulte, S.J.; Matsumoto, A.M.; Lee, S.P. Incidence, natural history, and risk factors for biliary sludges and stones during pregnancy. Hepatology 2005, 41, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Hould, F.S.; Fried, G.M.; Fazekas, A.G.; Tremblay, S.; Mersereau, W.A. Progesterone receptors regulate gallbladder motility. J. Surg. Res. 1988, 45, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.J. Chronic bacterial infection and subsequent human carcinogenesis. Eur. J. Cancer Prev. 1995, 4, 127–128. [Google Scholar] [PubMed]
- Ekbom, A.; Hsieh, C.C.; Yuen, J.; Trichopoulos, D.; McLaughlin, J.K.; Lan, S.J. Risk of extrahepatic bile duct cancer after cholecystectomy. Lancet 1993, 342, 1262–1265. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Combined oral contraceptives and gallbladder cancer. Int. J. Cancer 1989, 18, 309–314.
- Chow, W.H.; McLaughlin, J.K.; Menck, H.R.; Mack, T.M. Risk factor for extrahepatic bile duct cancers: Los Angeles County, California (USA). Cancer Cause Controls 1994, 5, 267–272. [Google Scholar] [CrossRef]
- Milne, R.; Vessey, M. The association of oral contraception with kidney cancer, colon cancer, gallbladder cancer (including extrahepatic bile duct cancer) and pituitary tumors. Contraception 1991, 43, 667–693. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, E.; Gallus, S.; Bosetti, C.; Franceschi, S.; Negri, E.; la Vecchia, C. Hormone replacement therapy and cancer risk: A systematic analysis from a network of case-control studies. Int. J. Cancer 2003, 105, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Gallus, S.; Negri, E.; Chatenoud, L.; Bosetti, C.; Franceschi, S.; La Vecchia, C. Post-menopausal hormonal therapy and gallbladder cancer risk. Int. J. Cancer 2002, 99, 762–763. [Google Scholar] [CrossRef] [PubMed]
- Chie, W.C.; Chung, Y.L.; Huang, C.S.; Chang, K.J.; Yen, M.L.; Lin, R.S. Oral contraceptives and breast cancer risk in Taiwan, a country of low incidence of breast cancer and low use of oral contraceptives. Int. J. Cancer 1998, 77, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Yen, M.L.; Yen, B.L.; Bai, C.H.; Lin, R.S. Risk factors for ovarian cancer in Taiwan: A case-control study in a low-incidence population. Gynecol. Oncol. 2003, 89, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospective studied cohort of US adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef] [PubMed]
- Samanic, C.; Gridley, G.; Chow, W.H.; Lubin, J.; Hoover, R.N.; Fraumeni, J.F. Obesity and cancer risk among white and black United States veterans. Cancer Causes Control 2004, 15, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Calle, E.E.; Kaaks, R. Overweight, obesity, and cancer: Epidemiological evidence and proposed mechanisms. Nat. Rev. Cancer 2004, 4, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Rossner, S. Weight gain in pregnancy. Hum. Reprod. 1997, 12, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Hinkula, M.; Pukkala, E.; Kyyronen, P.; Kauppila, A. Grand multiparity and incidence of endometrial cancer: A population-based study in Finland. Int. J. Cancer 2002, 98, 912–915. [Google Scholar] [CrossRef] [PubMed]
- Juntunen, K.; Kirkinen, P.; Kauppila, A. The clinical outcome in pregnancies of grand multiparous women. Acta Obstet. Gynecol. Scand. 1997, 76, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Chow, W.H.; Johansen, C.; Gridley, G.; Mellemkjaer, L.; Fraumeni, J.F. Gallstones, Cholecystectomy and risk of cancers of the liver, biliary tract and pancreas. Brit. J. Cancer 1999, 79, 640–644. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, T.-F.; Wu, C.-H.; Chiu, H.-F.; Yang, C.-Y. Parity and Risk of Death from Gallbladder Cancer among a Cohort of Premenopausal Parous Women in Taiwan. Int. J. Environ. Res. Public Health 2015, 12, 1864-1873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120201864
Chan T-F, Wu C-H, Chiu H-F, Yang C-Y. Parity and Risk of Death from Gallbladder Cancer among a Cohort of Premenopausal Parous Women in Taiwan. International Journal of Environmental Research and Public Health. 2015; 12(2):1864-1873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120201864
Chicago/Turabian StyleChan, Te-Fu, Chen-Hsuan Wu, Hui-Fen Chiu, and Chun-Yuh Yang. 2015. "Parity and Risk of Death from Gallbladder Cancer among a Cohort of Premenopausal Parous Women in Taiwan" International Journal of Environmental Research and Public Health 12, no. 2: 1864-1873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120201864