
Emergency Hospital Visits in Association with Volcanic Ash, Dust Storms and Other Sources of Ambient Particles: A Time-Series Study in Reykjavík, Iceland

Abstract
:1. Introduction
2. Experimental Section
2.1. Health Outcomes
2.2. Pollution Data
2.3. Statistical Methods
2.4. Reporting
3. Results and Discussion
3.1. Results
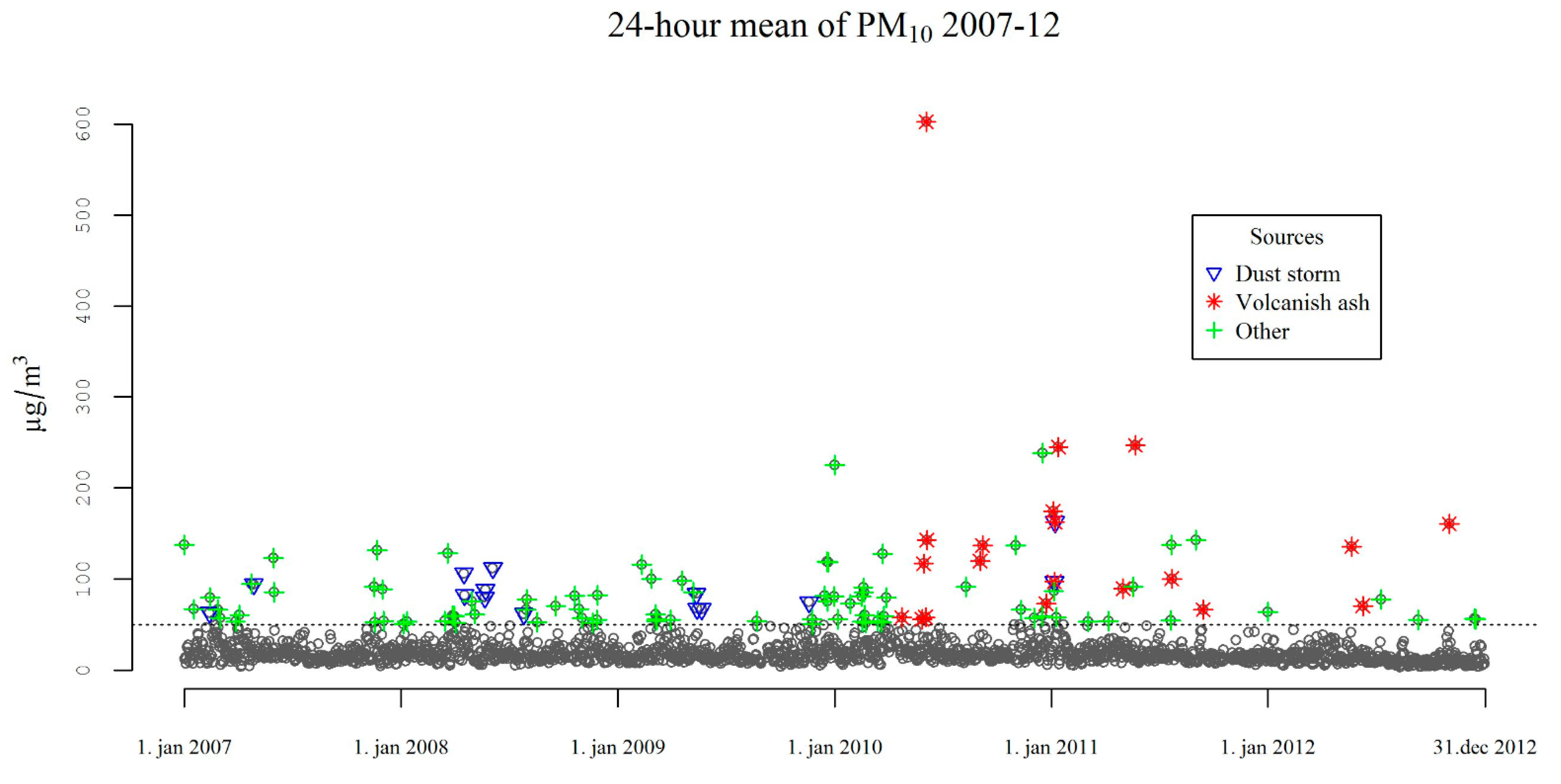
3.1.1. Descriptive Results


{kind=link}
{kind=link}
{kind=link}
| Emergency Hospital Visits | 2007–2012 | |||||||
|---|---|---|---|---|---|---|---|---|
| Number of admissions and ER visits | 22,892 | |||||||
| Individuals (n) | 11,567 | |||||||
| Age at first admission, mean (sd) | 68.1 (16.1) | |||||||
| Percentage female (n) | 46.3 (5351) | |||||||
| Daily Pollutant Levels | 2007–2012 n = 2192 | Volcanic Ash n = 20 | Dust Storm n = 14 | Other Sources n = 83 | ||||
| Mean | sd | Mean | sd | Mean | sd | Mean | sd | |
| PM10 (µg/m3) | 21.8 | 23.9 | 145.5 | 121.5 | 88.5 | 26.3 | 78.8 | 35.0 |
| H2S (µg/m3) | 3.2 | 5.7 | 3.4 | 3.4 | 2.5 | 5.0 | 4.0 | 8.3 |
| NO2 (µg/m3) | 18.2 | 13.2 | 8.3 | 8.1 | 10.5 | 8.1 | 25.2 | 19.5 |
| Temperature (°C) | 6.0 | 5.3 | 6.4 | 7.1 | 6.9 | 6.4 | 5.7 | 6.4 |
| Relative humidity (%) | 76.6 | 11.0 | 66.3 | 7.0 | 65.7 | 5.3 | 67.4 | 10.6 |
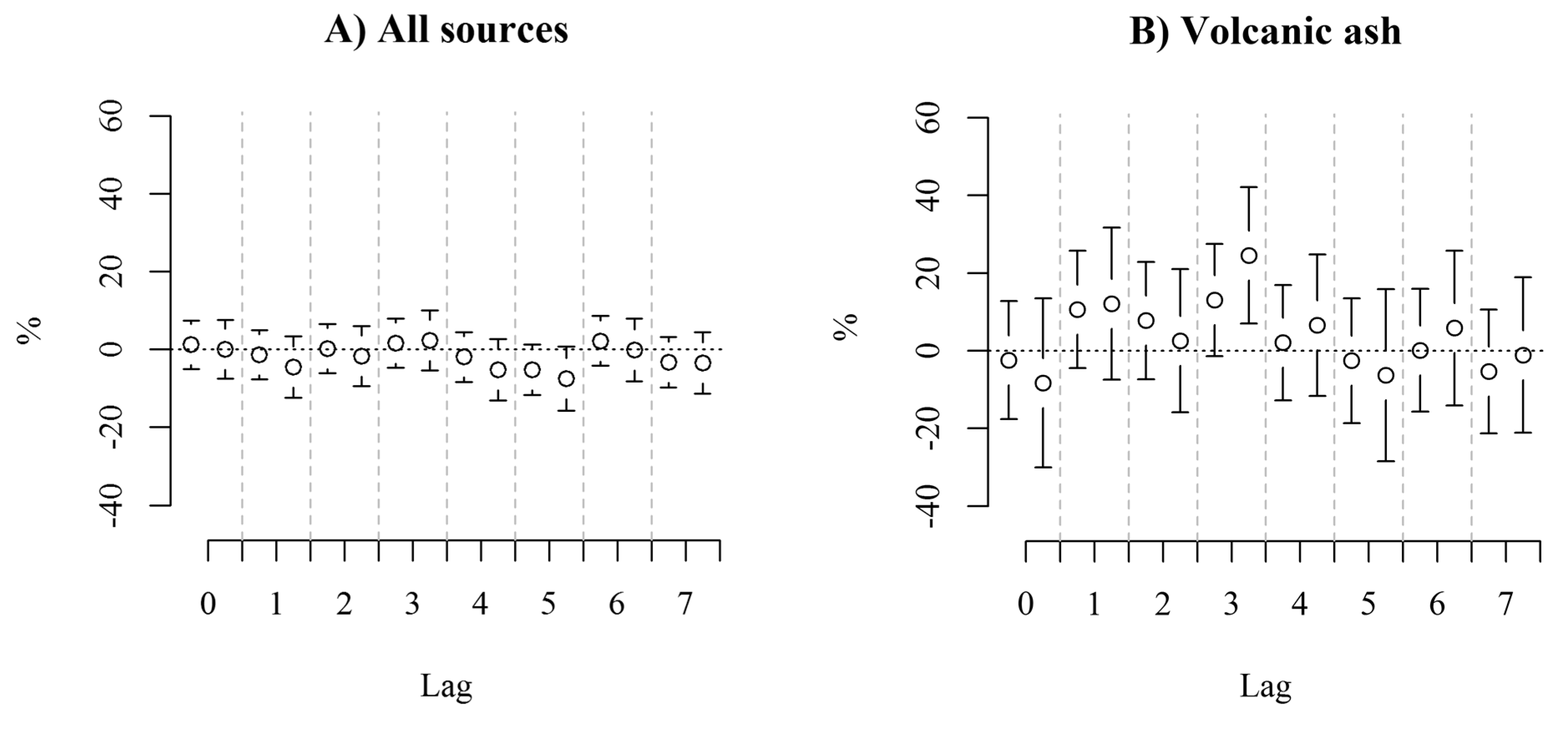
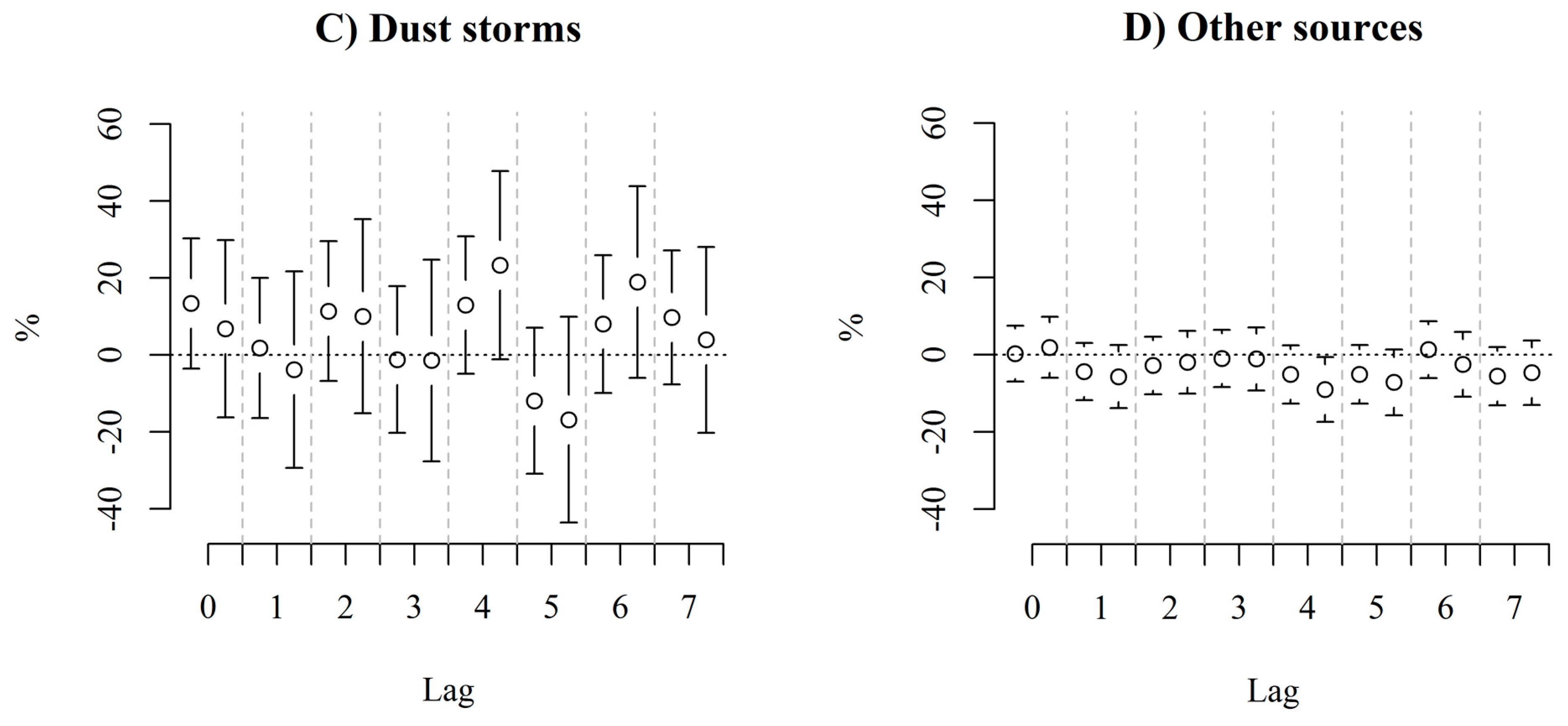
3.1.2. Results of the Analysis
| Indicator of PM10 Source | Percent Change in Emergency Hospital Visits * | Model | |
|---|---|---|---|
| % (95% CI) | p | R2 | |
| All sources | −0.7 (−2.6, 1.4) | 0.519 | 0.23 |
| -adjusted ** for PM10 | −2.4 (−5.6, 0.8) | 0.144 | 0.22 |
| -adjusted for NO2 and H2S | 0.2 (−2.2, 2.5) | 0.892 | 0.24 |
| -adjusted for NO2 H2S and PM10 | −2.8 (−6.6, 1.2) | 0.162 | 0.25 |
| Volcanic ash | 4.8 (0.6, 9.2) | 0.024 | 0.23 |
| -adjusted for PM10 | 6.1 (0.0, 12.7) | 0.052 | 0.22 |
| -adjusted for NO2 and H2S | 6.2 (2.6, 12.5) | 0.041 | 0.25 |
| -adjusted for NO2 H2S and PM10 | 7.3 (−0.4, 15.5) | 0.064 | 0.25 |
| Dust storm | 5.1 (0.5, 9.9) | 0.028 | 0.23 |
| -adjusted for PM10 | 5.8 (0.9, 19.9) | 0.019 | 0.22 |
| -adjusted for NO2 and H2S | 2.1 (−3.3, 8.0) | 0.444 | 0.25 |
| -adjusted for NO2 H2S and PM10 | 1.2 (−4.6, 7.4) | 0.692 | 0.25 |
| Other sources | −3.3 (−5.6, −1.0) | 0.007 | 0.23 |
| -adjusted for PM10 | −4.4 (−7.1, −1.7) | 0.002 | 0.22 |
| -adjusted for NO2 and H2S | −1.2 (−3.8, 1.5) | 0.375 | 0.25 |
| -adjusted for NO2 H2S and PM10 | −3.6 (−6.9, −0.2) | 0.036 | 0.25 |
3.2. Discussion


3.2.1. Strengths and Limitations
3.2.2. Statistical Power
3.2.3. Missing Pollution Data
3.2.4. Interpretation
4. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Anderson, H.R.; Atkinson, R.W.; Bremner, S.; Carrington, J.; Peacock, J. Quantitative Systematic Review of Short Term Associations between Ambient Air Pollution (Particulate Matter, Ozone, Nitrogen Dioxide, Sulphur Dioxide and Carbon Monoxide), and Mortality and Morbidity. 2007. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/215975/dh_121202.pdf (accessed on 10 March 2015).
- Andersen, Z.J.; Wahlin, P.; Raaschou-Nielsen, O.; Scheike, T.; Loft, S. Ambient particle source apportionment and daily hospital admissions among children and elderly in Copenhagen. J. Expos. Sci. Environ. Epidemiol. 2007, 17, 625–636. [Google Scholar]
- Schwarze, P.E.; Øvrevik, J.; Låg, M.; Refsnes, M.; Nafstad, P.; Hetland, R.B.; Dybing, E. Particulate matter properties and health effects: Consistency of epidemiological and toxicological studies. Hum. Exp. Toxicol. 2006, 25, 559–579. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.T.; Pope, C.A.; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [PubMed]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Meister, K.; Forsberg, B. Short-term associations between coarse PM levels and emergency department visits for asthma in Stockholm. Epidemiology 2009, 20. [Google Scholar] [CrossRef] [PubMed]
- Malig, B.J.; Ostro, B.D. Coarse particles and mortality: evidence from a multi-city study in California. Occup. Environ. Med. 2009, 66, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Forsberg, B. Epidemiological evidence of effects of coarse airborne particles on health. Eur. Respir. J. 2005, 26, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Sandstrom, T.; Forsberg, B. Desert dust: An unrecognized source of dangerous air pollution? Epidemiology 2008, 19, 808–809. [Google Scholar] [CrossRef] [PubMed]
- Thorsteinsson, T.; Gísladóttir, G.; Bullard, J.; McTainsh, G. Dust storm contributions to airborne particulate matter in Reykjavík, Iceland. Atmos. Environ. 2011, 45, 5924–5933. [Google Scholar] [CrossRef]
- Dagsson-Waldhauserova, P.; Arnalds, O.; Olafsson, H. Long term dust aerosol production from natural sources in Iceland. J. Air Waste Manage. Assn. 2013. [Google Scholar] [CrossRef]
- Arnalds, Ó. Dust sources and deposition of aeolian materials in Iceland. Icel. Agric. Sci. 2010, 23, 3–21. [Google Scholar]
- Arnalds, O.; Thorarinsdottir, E.F.; Thorsson, J.; Waldhauserova, P.D.; Agustsdottir, A.M. An extreme wind erosion event of the fresh Eyjafjallajokull 2010 volcanic ash. Sci. Rep. 2013, 3. [Google Scholar] [CrossRef] [PubMed]
- Thorsteinsson, T.; Jóhannsson, T.; Stohl, A.; Kristiansen, N.I. High levels of particulate matter in Iceland due to direct ash emissions by the Eyjafjallajökull eruption and resuspension of deposited ash. J. Geophys. Res. 2012, 117. [Google Scholar] [CrossRef]
- Carlsen, H.K.; Hauksdottir, A.; Valdimarsdottir, U.A.; Gíslason, T.; Einarsdottir, G.; Runolfsson, H.; Briem, H.; Finnbjornsdottir, R.G.; Gudmunsson, S.; Kolbeinsson, T.B.; Thorsteinsson, T.; Pétursdóttir, G. Health effects following the Eyjafjallajökull volcanic eruption: A cohort study. BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Newnham, R.; Dirks, K.; Samaranayake, D. An investigation into long-distance health impacts of the 1996 eruption of Mt Ruapehu, New Zealand. Atmos. Environ. 2010, 44, 1568–1578. [Google Scholar] [CrossRef]
- Horwell, C.; Baxter, P. The respiratory health hazards of volcanic ash: A review for volcanic risk mitigation. Bull. Volcanol. 2006, 69, 1–24. [Google Scholar] [CrossRef]
- Baxter, P.J.; Ing, R.; Falk, H.; Plikaytis, B. Mount St. Helens Eruptions: The acute respiratory effects of volcanic ash in a north American community. Arch. Environ. Health 1983, 38, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Cadelis, G.; Tourres, R.; Molinie, J.; Petit, R.H. Exacerbations d’asthme en Guadeloupe et éruption volcanique à Montserrat (70 km de la Guadeloupe). Rev. Mal. Respir. 2013, 30, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Oudin, A.; Carlsen, H.K.; Forsberg, B.; Johansson, C. Volcanic ash and daily mortality in Sweden after the icelandic volcano eruption of May 2011. Int. J. Environ. Res. Public Health 2013, 10, 6909–6919. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Lim, Y.H.; Kyung, S.Y.; An, C.H.; Lee, S.P.; Jeong, S.H.; Ju, Y.-S. Effects of ambient particulate matter on peak expiratory flow rates and respiratory symptoms of asthmatics during Asian dust periods in Korea. Respirology 2005, 10, 470–476. [Google Scholar] [CrossRef]
- Lee, H.; Kim, H.; Honda, Y.; Lim, Y.-H.; Yi, S. Effect of Asian dust storms on daily mortality in seven metropolitan cities of Korea. Atmos. Environ. 2013, 79, 510–517. [Google Scholar] [CrossRef]
- Chan, C.-C.; Ng, H.-C. A case-crossover analysis of Asian dust storms and mortality in the downwind areas using 14-year data in Taipei. Sci. Tot. Env. 2011, 410–411, 47–52. [Google Scholar] [CrossRef]
- Perez, L.; Tobias, A.; Querol, X.; Künzli, N.; Pey, J.; Alastuey, A.; Viana, M.; Valero, N.; González-Cabré, M.; Sunyer, J. Coarse particles from Saharan dust and daily mortality. Epidemiology 2008, 19, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, H.K.; Forsberg, B.; Meister, K.; Gíslason, T.; Oudin, A. Ozone is associated with cardiopulmonary and stroke emergency hospital visits in Reykjavík, Iceland 2003–2009. Environ. Health 2013, 12. [Google Scholar] [CrossRef] [Green Version]
- Carlsen, H.K.; Zoëga, H.; Valdimarsdóttir, U.; Gíslason, T.; Hrafnkelsson, B. Hydrogen sulfide and particle matter levels associated with increased dispensing of anti-asthma drugs in Iceland’s capital. Environ. Res. 2012, 113, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Finnbjornsdottir, R.G.; Zoëga, H.; Olafsson, O.; Thorsteinsson, T.; Rafnsson, V. Association of air pollution and use of glyceryl trinitrate against angina pectoris: A population-based case-crossover study. Environ. Health 2013, 12. [Google Scholar] [CrossRef]
- Infectious Diseases by Month 1997–2011. Available online: http://www.landlaeknir.is/servlet/file/store93/item17624/Skr%C3%A1ningarskyldir_1997_2011.xls (accessed on 25 January 2014).
- Influenza Statistics 2012. Available online: http://www.landlaeknir.is/influensa/tolur-um-influensu/ (accessed on 25 January 2014).
- Air Quality Guidelines—Global Update 2005; World Health Organization: Geneva, Switzerland.
- Boogaard, H.; Kos, G.P.A.; Weijers, E.P.; Janssen, N.A.H.; Fischer, P.H.; van der Zee, S.C.; de Hartog, J.J.; Hoek, G. Contrast in air pollution components between major streets and background locations: Particulate matter mass, black carbon, elemental composition, nitrogen oxide and ultrafine particle number. Atmos. Env. 2011, 45, 650–658. [Google Scholar] [CrossRef]
- Arnalds, Ó.; Thorarinsdottir, E.F.; Metusalemsson, S.; Jónsson, Á.; Gretarsson, E.; Arnason, A. Soil Erosion in Iceland; Soil Conservation Service, Agricultural Research Institute: Hella, Iceland, 2001. [Google Scholar]
- Arnalds, O; Gisladottir, F.O.; Sigurjonsson, H. Sandy deserts of Iceland: An overview. J. Arid Environ. 2001, 47, 359–371. [Google Scholar] [CrossRef]
- Dr., Thorsteinsson, Throstur; University of Iceland, Reykjavík, Iceland. Personal communication, 26 October 2013.
- Goldberg, M.S.; Burnett, R.T.; Stieb, D.M.; Brophy, J.M.; Daskalopoulou, S.S.; Valois, M.-F.; Brook, J.R. Associations between ambient air pollution and daily mortality among elderly persons in Montreal, Quebec. Sci. Tot. Environ. 2013, 463–464, 931–942. [Google Scholar] [CrossRef]
- Monick, M.M.; Baltrusaitis, J.; Powers, L.S.; Borcherding, J.A.; Caraballo, J.C.; Mudunkotuwa, I.; Peate, D.W.; Walters, K.; Thompson, J.M.; Grassian, V.H.; et al. Effects of Eyjafjallajökull volcanic ash on innate immune system responses and bacterial growth in vitro. Environ. Health Perspect. 2013, 121, 691–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alessandrini, E.R.; Stafoggia, M.; Faustini, A.; Gobbi, G.P.; Forastiere, F. Saharan dust and the association between particulate matter and daily hospitalisations in Rome, Italy. Occup. Environ. Med. 2013, 70, 432–434. [Google Scholar] [CrossRef] [PubMed]
- R Development Core. R: A Language and Environment for Statistical Computing (Version 3.0.1); The R Foundation for Statistical Computing: Vienna, Austria, 2013. Available online: http://www.R-project.org/ (accessed on 29 December 2013).
- Pérez, L.; Tobías, A.; Pey, J.; Pérez, N.; Alastuey, A.; Sunyer, J.; Querol, X. Effects of local and saharan particles on cardiovascular disease mortality. Epidemiology 2012, 23, 768–769. [Google Scholar] [CrossRef] [PubMed]
- Horwell, C.J.; Baxter, P.J.; Hillman, S.E.; Calkins, J.A.; Damby, D.E.; Delmelle, P.; Donaldson, K.; Dunster, C.; Fubini, B.; Kelly, F.J.; et al. Physicochemical and toxicological profiling of ash from the 2010 and 2011 eruptions of Eyjafjallajökull and Grímsvötn volcanoes, Iceland using a rapid respiratory hazard assessment protocol. Environ. Res. 2013, 127, 63–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Icelandic Road Administration. The Composition of Particle Matter in Reykjavík. Available online: http://www.vegagerdin.is/Vefur2.nsf/Files/Samsetning_svifryks_Rvk/$file/Samsetning%20svifryks%20%C3%AD%20Reykjav%C3%ADk.pdf (accessed on 5 February 2014).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlsen, H.K.; Gislason, T.; Forsberg, B.; Meister, K.; Thorsteinsson, T.; Jóhannsson, T.; Finnbjornsdottir, R.; Oudin, A. Emergency Hospital Visits in Association with Volcanic Ash, Dust Storms and Other Sources of Ambient Particles: A Time-Series Study in Reykjavík, Iceland. Int. J. Environ. Res. Public Health 2015, 12, 4047-4059. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404047
Carlsen HK, Gislason T, Forsberg B, Meister K, Thorsteinsson T, Jóhannsson T, Finnbjornsdottir R, Oudin A. Emergency Hospital Visits in Association with Volcanic Ash, Dust Storms and Other Sources of Ambient Particles: A Time-Series Study in Reykjavík, Iceland. International Journal of Environmental Research and Public Health. 2015; 12(4):4047-4059. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404047
Chicago/Turabian StyleCarlsen, Hanne Krage, Thorarinn Gislason, Bertil Forsberg, Kadri Meister, Throstur Thorsteinsson, Thorsteinn Jóhannsson, Ragnhildur Finnbjornsdottir, and Anna Oudin. 2015. "Emergency Hospital Visits in Association with Volcanic Ash, Dust Storms and Other Sources of Ambient Particles: A Time-Series Study in Reykjavík, Iceland" International Journal of Environmental Research and Public Health 12, no. 4: 4047-4059. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404047