
BMI, Overweight Status and Obesity Adjusted by Various Factors in All Age Groups in the Population of a City in Northeastern Brazil


Abstract
:1. Introduction
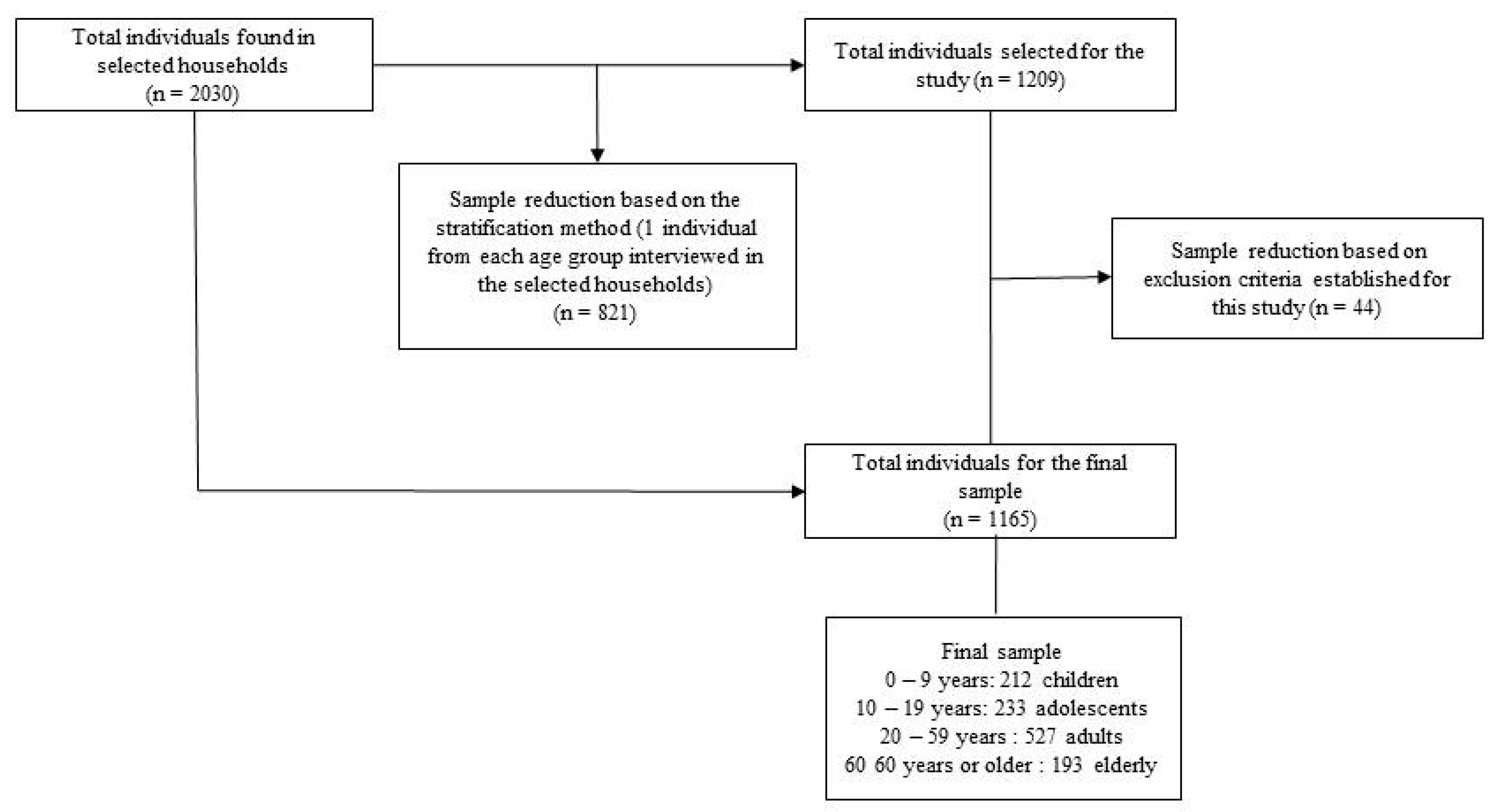
2. Participants and Methods
2.1. Study Design and Population

2.2. Body Measurements
2.3. Statistical Analyses
3. Results

{kind=link}
| Mean | SD | Amplitude | N | % | ||
|---|---|---|---|---|---|---|
| Demographic, socioeconomic and lifestyle characteristics | ||||||
| Sex | males | - | - | - | 420 | 36 |
| females | - | - | - | 745 | 64 | |
| Age (years) | 0–9 years | 4.52 | 2.94 | 9.00 | 212 | 18.1 |
| 10–19 years | 14.36 | 2.84 | 9.00 | 233 | 20.1 | |
| 20–59 years | 38.64 | 11.41 | 39.00 | 527 | 45.3 | |
| ≥60 years | 69.34 | 7.60 | 37.00 | 192 | 16.5 | |
| 32.63 | 22.84 | 97.00 | 1164 | 100.00 | ||
| Schooling 1 | Up to elementary school | - | - | - | 553 | 47.5 |
| ≥incomplete high school | - | - | - | 612 | 52.5 | |
| 1165 | 100.00 | |||||
| Family income (R$) 2 | 1843.30 | 2159.54 | 18,000.00 | 1126 | 100.00 | |
| Smoking | yes | - | - | - | 107 | 9.2 |
| no | - | - | - | 1058 | 90.8 | |
| 1165 | 100.00 | |||||
| Alcohol consumption 3 | yes | 0.29 | 0.37 | 2.5 | 158 | 13.6 |
| no | - | - | - | 1006 | 86.4 | |
| 1164 | 100.00 | |||||
| Practice of phys. Activity 4 | yes | - | - | - | 111 | 9.5 |
| (5 times / week) | days/week | 5.32 | 0.67 | 2.00 | - | - |
| Duration activity/min | 70.53 | 43.90 | 245 | - | - | |
| no | - | - | - | 1054 | 90.5 | |
| 1165 | 100.00 | |||||
| Anthropometric characteristics | ||||||
| Weight(kg) | 52.38 | 25.21 | 126 | 1095 | - | |
| Height(m) | 1.40 | 0.42 | 1.85 | 1089 | - | |
| BMI (kg/m2) | 23.57 | 6.31 | 49.83 | 1086 | - | |
| BMI classification * | ||||||
| Low weight/normal weight | 19.41 | 3.24 | 13.24 | 572 | 52.7 | |
| Overweight | 27.16 | 1.43 | 5.03 | 305 | 28 | |
| Obesity | 33.85 | 3.56 | 21.30 | 209 | 19.2 | |
| Variables | Low weight/normal weight | Overweight | Obesity | Total | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | N | |||
| Age group | 0–9 | 139 | 68.47 | 40 | 19.7 | 24 | 11.82 | 203 | 0.0000 * |
| 10–19 | 158 | 72.81 | 42 | 19.35 | 17 | 7.83 | 217 | ||
| 20–59 | 211 | 43.78 | 160 | 43.19 | 111 | 23.03 | 482 | ||
| ≥60 years | 64 | 34.78 | 63 | 34.24 | 57 | 30.98 | 184 | ||
| Sex | Males | 224 | 60.4 | 97 | 26.14 | 50 | 13.5 | 371 | 0.0000 * |
| Females | 351 | 48.89 | 208 | 28.97 | 159 | 22.14 | 718 | ||
| Sex: male (According to age group) | 0–9 | 75 | 68.18 | 21 | 19.09 | 14 | 12.73 | 110 | 0.0000 * |
| 10–19 | 72 | 72.00 | 22 | 22 | 06 | 6.00 | 100 | ||
| 20–59 | 47 | 48.96 | 32 | 33.33 | 17 | 17.71 | 96 | ||
| ≥60 years | 25 | 41.67 | 22 | 36.67 | 13 | 21.66 | 60 | ||
| Sex: female (According to age group) | 0–9 | 64 | 68.82 | 19 | 20.43 | 10 | 10.75 | 93 | 0.0000 * |
| 10–19 | 85 | 73.28 | 20 | 17.24 | 11 | 9.48 | 116 | ||
| 20–59 | 164 | 42.49 | 128 | 33.16 | 94 | 24.35 | 386 | ||
| ≥60 years | 38 | 30.90 | 41 | 33.33 | 44 | 35.77 | 123 | ||
| Schooling 1 | Up to elementary school | 281 | 53.12 | 133 | 25.14 | 115 | 21.74 | 529 | * 0.0025 |
| ≥incomplete high school | 290 | 52.16 | 172 | 30.93 | 94 | 16.91 | 556 | 0.0000 * | |
| Schooling according to age group | |||||||||
| Up to elementary school | 0–9 | 84 | 74.34 | 16 | 14.16 | 13 | 11.50 | 113 | 0.0000 * |
| 10–19 | 80 | 74.07 | 19 | 17.59 | 9 | 8.33 | 108 | ||
| 20–59 | 81 | 42.86 | 54 | 28.57 | 54 | 28.57 | 189 | ||
| ≥60 years | 36 | 30.25 | 44 | 36.98 | 39 | 32.77 | 119 | ||
| ≥incomplete high school | 0–9 | 55 | 61.11 | 24 | 26.67 | 11 | 12.22 | 90 | 0.5515 |
| 10–19 | 78 | 71.56 | 23 | 21.10 | 8 | 7.34 | 109 | ||
| 20–59 | 130 | 44.37 | 106 | 36.18 | 57 | 19.45 | 293 | ||
| ≥60 years | 27 | 42.19 | 19 | 29.69 | 18 | 28.12 | 64 | ||
| Family income (R$)2 | ≤1000 | 304 | 54.19 | 110 | 19.61 | 147 | 26.20 | 561 | 0.0000 * |
| >1000 | 252 | 51.01 | 153 | 30.97 | 89 | 18.02 | 494 | ||
| Family income according to age group | |||||||||
| <Median | 0–9 | 86 | 70.5 | 21 | 17.2 | 15 | 12.3 | 122 | 0.0000 * |
| 10–19 | 89 | 72.35 | 26 | 21.13 | 8 | 6.50 | 123 | ||
| 20–59 | 103 | 33.1 | 70 | 29.3 | 66 | 27.6 | 239 | ||
| ≥60 years | 24 | 32.87 | 28 | 38.5 | 21 | 28.76 | 73 | ||
| ≥Median | 0–9 | 47 | 46.4 | 18 | 26.08 | 5 | 7.24 | 69 | >0.0000 * |
| 10–19 | 63 | 71.6 | 16 | 18.18 | 9 | 10.22 | 88 | ||
| 20–59 | 105 | 45.06 | 87 | 37.33 | 41 | 17.60 | 233 | ||
| ≥60 years | 36 | 35.3 | 32 | 31.37 | 34 | 33.33 | 102 | ||
| Smoking | no | 523 | 52.88 | 281 | 28.41 | 185 | 18.71 | 989 | 0.0471 * |
| yes | 49 | 50.52 | 24 | 24.74 | 24 | 24.71 | 97 | ||
| Alcohol consumption | no | 498 | 53.72 | 257 | 27.72 | 172 | 18.56 | 927 | 0.1785 |
| yes | 73 | 46.20 | 48 | 30.38 | 37 | 23.42 | 158 | ||
| Pract. physical activity | no | 526 | 53.24 | 273 | 27.63 | 189 | 19.13 | 988 | 0.4611 |
| (5 times/week) | yes | 46 | 46.94 | 32 | 32.65 | 20 | 20.41 | 98 | |
| Multiple Regression | ||||
|---|---|---|---|---|
| Adjustment 1: all age groups | ||||
| Coefficient | CI95% | Statisticst | p-Value | |
| Intercept | 16.41 | 16.41 ± 0.71 | 22.95 | >0.0000 * |
| Schooling | 3.21 | 3.21 ± 0.36 | 8.83 | >0.0000 * |
| Income | 0.25 × 10−3 | 0.25 × 10−3 ± 0.09× 10−3 | 2.95 | 0.0032 * |
| Sex | 2.96 | 2.96 ± 0.38 | 7.69 | >0.0000 * |
| Physical activity | 0.92 | 0.92 ± 0.43 | 2.12 | 0.0344 * |
| Adjustment 2: 0 to 9 years | ||||
| Coefficient | CI95% | Statisticst | p-Value | |
| Intercept | 17.4 | 17.4 ± 0.7 | 24.65 | >0.0000 * |
| Schooling | −0.09 | −0.09 ± 0.44 | −0.20 | 0.8410 |
| Income | 0.03 × 10−3 | 0.03 × 10−3 ± 0.13 × 10−3 | 0.24 | 0.8140 |
| Sex | −0.58 | −0.58 ± 0.41 | −1.39 | 0.1660 |
| Physical activity | 0.03 | 0.03 ± 0.71 | 0.04 | 0.9650 |
| Adjustment 3: 10 to 19 years | ||||
| Coefficient | CI95% | Statisticst | p-Value | |
| Intercept | 18.33 | 18.33 ± 1.18 | 15.52 | >0.0000 * |
| Schooling | 0.9 | 0.9 ± 0.64 | 1.39 | 0.1650 |
| Income | 0.17 × 10−3 | 0.17 × 10−3 ± 0.15 × 10−3 | 1.13 | 0.2590 |
| Sex | 0.91 | 0.91 ± 0.65 | 1.39 | 0.1670 |
| Physical activity | 1.11 | 1.11 ± 0.71 | 1.57 | 0.1118 |
| Adjustment 4: 20 to 59 years | ||||
| Coefficient | CI95% | Statisticst | p-Value | |
| Intercept | 22.91 | 22.91 ± 1.30 | 17.56 | >0.0000 * |
| Schooling | 2.48 | 2.48 ± 0.51 | 4.89 | >0.0000 * |
| Income | 0.00 | 0.00 ± 0.12 × 10−3 | 0.01 | 0.9946 |
| Sex | 1.10 | 1.10 ± 0.64 | 1.72 | 0.0866 |
| Physical activity | −0.42 | −0.42 ± 0.61 | −0.70 | 0.4857 |
| Smoking | −0.29 | 0.29 ± 0.7 | −0.43 | 0.6662 |
| Alcohol consumption | 1.02 | 1.02 ± 1.89 | 0.54 | 0.5897 |
| Adjustment 5: 60 years or older | ||||
| Coefficient | CI95% | Statisticst | p-Value | |
| Intercept | 23.81 | 23.81 ± 1.61 | 14.75 | >0.0000 * |
| Schooling | 1.51 | 1.51 ± 0.78 | 1.93 | 0.0552 |
| Income | 0.13 × 10−3 | 0.13 × 10−3 ± 0.16 × 10−3 | 0.00 | 0.3962 |
| Sex | 1.72 | 1.72 ± 0.81 | 2.11 | 0.0362 * |
| Physical activity | −0.35 | −0.35 ± 0.80 | −0.45 | 0.6569 |
| Smoking | −1.35 | −1.35 ± 1.26 | −1.07 | 0.2880 |
| Alcohol consumption | −0.91 | −0.91 ± 1.29 | −0.71 | 0.4807 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mendonça, M.R.T.; Silva, M.A.M.; Rivera, I.R.; Moura, A.A. Prevalência de sobrepeso e obesidade em crianças e adolescentes da cidade de Maceió. Rev. Assoc. Med. Bras. 2010, 56, 192–196. [Google Scholar] [CrossRef] [PubMed]
- WHO—World Health Organization. New WHO Statistics Report Includes Good News for Women’s and Children’s Health. Available online: http://www.who.int/pmnch/media/news/2012/20120516_who_statistics/en/ (accessed on 25 June 2012).
- Monteiro, C.A.; Moura, E.C.; Conde, W.L.; Popkin, B.M. Socioeconomic status and obesity in adult populations of developing countries: A review. Bull. World Health Organ. 2004, 82, 940–946. [Google Scholar] [PubMed]
- McLaren, L. Socioeconomic status and obesity. Epidemiol. Rev. 2007, 29, 29–48. [Google Scholar] [CrossRef] [PubMed]
- NCHS—National Center for Health Statistics, United States, 2010. Available online: www. cdc.gov/nchs/data/hus/hus06.pdf#07 (accessed on 14 June 2012).
- Popkin, B.M. The World Is Fat: The Fads, Trends, Policies, and Products That Are Fattening the Human Race; Avery: New York, NY, USA, 2008. [Google Scholar]
- VIGITEL - Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas por Inquérito Telefônico; Ministério da Saúde: Brasília, Brasil, 2011.
- IBGE (Instituto Brasileiro de Geografia e Estatística). Pesquisa de Orçamentos Familiares—POF,2008–2009: Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil; IBGE: Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Dal Grande, E.; Gill, T.; Wyatt, L.; Chittleborough, C.R.; Phillips, P.J.; Taylor, A.W. Population attributable risk (PAR) of overweight and obesity on chronic diseases: South Australian representative, cross-sectional data, 2004–2006. Obes. Res. Clin. Pract. 2009, 3, 59–68. [Google Scholar]
- Tavassoli, A.A.; Gharipour, M.; Khosravi, A.; Kelishadi, R.; Siadat, Z.D.; Bahonar, A.; Sadri, G.H.; Sadeghi, M.; Rabiei, K.; Sajjadi, F.; et al. Gender differences in obesogenic behaviour, socioeconomic and metabolic factors in a population-based sample of Iranians: The IHHP study. J. Health Popul. Nutr. 2010, 28, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Kristjansson, E.A.; Russel, K.; Billette, M.; Sawada, M.C.; Ali, A.; Tremblay, M.S.; Prud’homme, D. Relationships between neighborhoods, physical activity, and obesity: A multilevel analysis of a Large Canadian City. Obesity 2012, 20, 2093–2100. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.A.; Kremer, P.J.; Swinburn, B.A.; Silva-Sanigorski, A.M. Multilevel analysis of the be active Eat well intervention: Environmental and behavioural influences on reductions in child obesity risk. Int. J. Obes. 2012, 36, 901–907. [Google Scholar] [CrossRef]
- Lee, S.T.; Wong, J.E.; Shanita, N.S.; Ismail, M.N.; Deurenberg, P.; Poh, B.K. Daily physical activity and screen time, but not other sedentary activities, are associated with measures of obesity during childhood. Int. J. Environ. Res. Public Health 2014, 12, 141–161. [Google Scholar] [CrossRef]
- R Development Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2009. Available online: http://www.R- project.org (accessed on 16 April 2010).
- Luna, R.C.P.; Nascimento, C.C.C.; Asciutti, L.S.R.; Franceschini, S.C.C.; Filizola, R.G.; Diniz, A.S.; de Moraes, R.M.; Rivera, M.A.; Gonçalves Mda, C.; Costa, M.J. Relation between glucose levels, high-sensitivity C-reactive protein (hs-CRP), body mass index (BMI) and serum and dietary retinol in elderly in population-based study. Arch. Gerontol. Geriatr. 2012, 54, 462–468. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Expert Committee. Physical Status: The Use and Interpretation of Anthropometry; Technical Report Series, No 854; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- Asciutti, L.S.R.; Rivera, M.A.A.; Costa, M.J.C.; Imperiano, E.; Arruda, M.S.; Bandeira, M.G.; Arruda, N.S. Manual de Porções Média em Tamanho real Baseado No Programa Dietsys Para estudo de Base Populacional; UFPB: João Pessoa, Paraíba, 2005. [Google Scholar]
- Block, G. Health Habits and History Questionnaire: Diet History and Other Risk Factors; National Cancer Institute: Bethesda, MA, USA, 1988. [Google Scholar]
- Lima, L.P.; Sampaio, H.A.C. Caracterização socioeconômica, antropométrica e alimentar de obesos graves. Ciênc. Saúde Colet. 2007, 12, 1011–1020. [Google Scholar] [CrossRef]
- Lahti-Koski, M.; Pietinen, P.; Heliövaara, M.; Vartiainen, E. Associations of body mass index and obesity with physical activity, food choices, alcohol intake, and smoking in the 1982–1997 FINRISK Studies. Am. J. Clin. Nutr. 2002, 75, 809–817. [Google Scholar] [PubMed]
- American College of Sports Medicine (2011). Available online: http://www.acsm.org/about-acsm/media-room/news-releases/2011/08/01/acsm-issues-new-recommendations-on-quantity-and-quality-of-exercise (accessed on 3 September 2012).
- Siegel, S. Estatística não Paramétrica Para as Ciências do Comportamento; McGraw-Hill do Brasil: São Paulo, Brazil, 1977. [Google Scholar]
- Sabanayagam, C.; Shankar, A.; Saw, S.M.; Tai, S.T.; Wong, T.Y. The association between socioeconomic status and overweight/obesity in a Malay population in Singapore. Asia Pac. J. Public Health 2009, 21, 487–496. [Google Scholar] [PubMed]
- Dinsa, G.D.; Goryakin, Y.; Fumagalli, E.; Suhrcke, M. Obesity and socioeconomic status in developing countries: A systematic review. Obes. Rev. 2012, 13, 1067–1079. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity in the United States, 2009–2010. NCHS Data Briefs 2012, 82, 1–8. [Google Scholar]
- Biro, F.M.; Wien, M. Childhood obesity and adult morbidities. Am. J. Clin. Nutr. 2010, 91, 1499–1505. [Google Scholar] [CrossRef]
- Marinos, E. Obesity in the elderly. Obes. Res. 2001, 9, 244–248. [Google Scholar] [CrossRef]
- Bae, J.; Joung, H.; Kim, J.Y.; Kwon, K.N.; Kim, Y.; Park, S.W. Validity of self-reported height, weight, and body mass index of the Korea Youth Risk Behavior Web-based Survey questionnaire. J. Prev. Med. Public Health 2010, 43, 340–396. [Google Scholar]
- Villareal, D.T.; Apovian, C.M.; Kushner, R.F.; Klein, S.; American Society for Nutrition; NAASO. The Obesity Society. Obesity in older adults: Technical review and position statement of the American Society for Nutrition and NAASO, The Obesity Society. Obes. Res. 2005, 13, 1849–1863. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.L.; Hollingsworth, K.G.; Aribisala, B.S.; Chen, M.J.; Mathers, J.C.; Taylor, R. Reversal of type 2 diabetes: Normalization of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 2011, 54, 2506–2514. [Google Scholar] [CrossRef] [PubMed]
- Drummer, T.J.B.; Kirk, S.F.L.; Penney, T.L.; Dodds, L.; Parker, L. Targeting policy for obesity prevention: Identifying the critical age for weight gain in women. J. Obes. 2012, 934895, 1–7. [Google Scholar] [CrossRef]
- Yoo, S.; Cho, H.J.; Khang, Y.H. General and abdominal obesity in South Korea, 1998–2007: gender and socioeconomic differences. Prev. Med. 2010, 51, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Zang, Q.; Wang, Y. Socioeconomic inequality of obesity in the United States: Do gender, age, and ethnicity matter? BMC Med. 2004, 58, 1171–1180. [Google Scholar]
- Brambilla, P.; Bedogni, G.; Moreno, L.A.; Goran, M.I.; Gutin, B.; Fox, K.R.; Peters, D.M.; Barbeau, P.; de Simone, M.; Pietrobelli, A. Cross validation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int. J. Obes. 2006, 30, 23–30. [Google Scholar] [CrossRef]
- Jones-Smith, J.C.; Gordon-Larsen, P.; Siddiqi, A.; Popkin, B.M. Is the burden of overweight shifting to the poor across the globe? Time trends among women in 39 low- and middle-income countries (1991–2008). Int. J. Obes. 2011, 36, 1114–1120. [Google Scholar] [CrossRef]
- Neuman, N.; Finlay, J.E.; Smith, G.D.; Subramanian, S.V. The poor stay thinner: Stable socioeconomic gradients in BMI among women in lower- and middle-income countries. Am. J. Clin. Nutr. 2011, 94, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Clark, K.; Coleman, E.; Donnelly, J.E.; Foreyt, J.; Melanson, E.; Volek, J.; Volpe, S.L.; American College of Sports Medicine. American College of Sports Medicine position stand. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2001, 33, 2145–2156. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, J.; Wyatt, K. The Healthy Lifestyles Programme (HeLP)—An overview of and recommendations arising from the conceptualisation and development of an innovative approach to promoting healthy lifestyles for children and their families. Int. J. Environ. Res. Public Health 2015, 20, 1003–1019. [Google Scholar] [CrossRef] [Green Version]
- Fraser, L.K.; Edwards, K.L.; Cade, J.; Clarke, G.P. The geography of fast food outlets: A review. Int. J. Environ. Res. Public Health 2010, 7, 2290–2308. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.I.; So, W.Y. Relationship between obesity in Korean adolescents and the frequency of alcohol consumption, the amount of alcohol consumed, and the frequency of severe alcohol intoxication. Obes. Res. Clin. Pract. 2011, 6, 159–166. [Google Scholar] [CrossRef]
- Guilland, J.C.; Costa, M.J.C.; Moreau, D.; Boggio, V.; Lhuissier, M.; Fuchs, F. Interrelations of alcool intake with blood vitamin status in nonalco holic subjects. Nutr. Res. 2006, 14, 1317–1330. [Google Scholar] [CrossRef]
- Wadden, T.A.; Stunkard, J.A. Handbok of Obesity Treatment; Guilford Press: New York, NY, USA, 2002; p. 624. [Google Scholar]
- Shavers, V.L. Measurement of socioeconomic status in health disparities research. J. Natl. Med. Assoc. 2007, 99, 1013–1023. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ataíde Lima, R.P.; De Carvalho Pereira, D.; Pordeus Luna, R.C.; Gonçalves, M.D.C.R.; De Lima, R.T.; Filho, M.B.; Filizola, R.G.; De Moraes, R.M.; Asciutti, L.S.R.; Costa, M.J.d.C. BMI, Overweight Status and Obesity Adjusted by Various Factors in All Age Groups in the Population of a City in Northeastern Brazil. Int. J. Environ. Res. Public Health 2015, 12, 4422-4438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404422
Ataíde Lima RP, De Carvalho Pereira D, Pordeus Luna RC, Gonçalves MDCR, De Lima RT, Filho MB, Filizola RG, De Moraes RM, Asciutti LSR, Costa MJdC. BMI, Overweight Status and Obesity Adjusted by Various Factors in All Age Groups in the Population of a City in Northeastern Brazil. International Journal of Environmental Research and Public Health. 2015; 12(4):4422-4438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404422
Chicago/Turabian StyleAtaíde Lima, Raquel Patrícia, Danielle De Carvalho Pereira, Rafaella Cristhine Pordeus Luna, Maria Da Conceição Rodrigues Gonçalves, Roberto Teixeira De Lima, Malaquias Batista Filho, Rosália Gouveia Filizola, Ronei Marcos De Moraes, Luiza Sonia Rios Asciutti, and Maria José de Carvalho Costa. 2015. "BMI, Overweight Status and Obesity Adjusted by Various Factors in All Age Groups in the Population of a City in Northeastern Brazil" International Journal of Environmental Research and Public Health 12, no. 4: 4422-4438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404422