
Environmental Asthma Reduction Potential Estimates for Selected Mitigation Actions in Finland Using a Life Table Approach

Abstract
:1. Introduction
2. Material and Methods
2.1. Asthma Statistics
2.2. Identification of Risk and Protective Factors
2.3. Exposure Trend and Population Attributable Fractions (PAF) for Risk and Protective Factors

{kind=link}
{kind=link}
{kind=link}
| Scenario | Factor | Exposure in 2011 | Ref. | Relative Risk (RR) | Ref. | Population Attributable Fraction (PAF) a |
|---|---|---|---|---|---|---|
| 1 | Active smoking | 17% | [17] | 1.03 | [8] | 0.3% |
| Second Hand Smoke (<14 y) | 4% | [18] | 1.32 | [9] | 0.6% | |
| Second Hand Smoke (≥21 y) | 10% | [10] | 1.97 | [10] | 4.4% | |
| 2 | Fine particles (PM2.5) | 100% b | [19] | 1.015 c | [12] | 11.6% |
| 3 | Dampness | 15% | [21] | 1.34 | [11] | 4.8% |
| 4 | Cat | 18.5% d | [22] | 0.47 | [13] | 3.4% |
| Cat | 1.5% e | 1.67 | [14] | 0.3% | ||
| Dog | 22.2% d | 0.37 | [13] | 5.2% | ||
| Dog | 1.8% e | 2.78 | [14] | 0.8% |
2.4. Attributable Asthma Burden
2.5. Selection of Mitigation Actions
3. Results and Discussion
3.1. Historical Records of Asthma Entitlements (1986–2011) and Future Projection (to 2040)
3.2. Environmental Burden of Disease (EBD) of Asthma
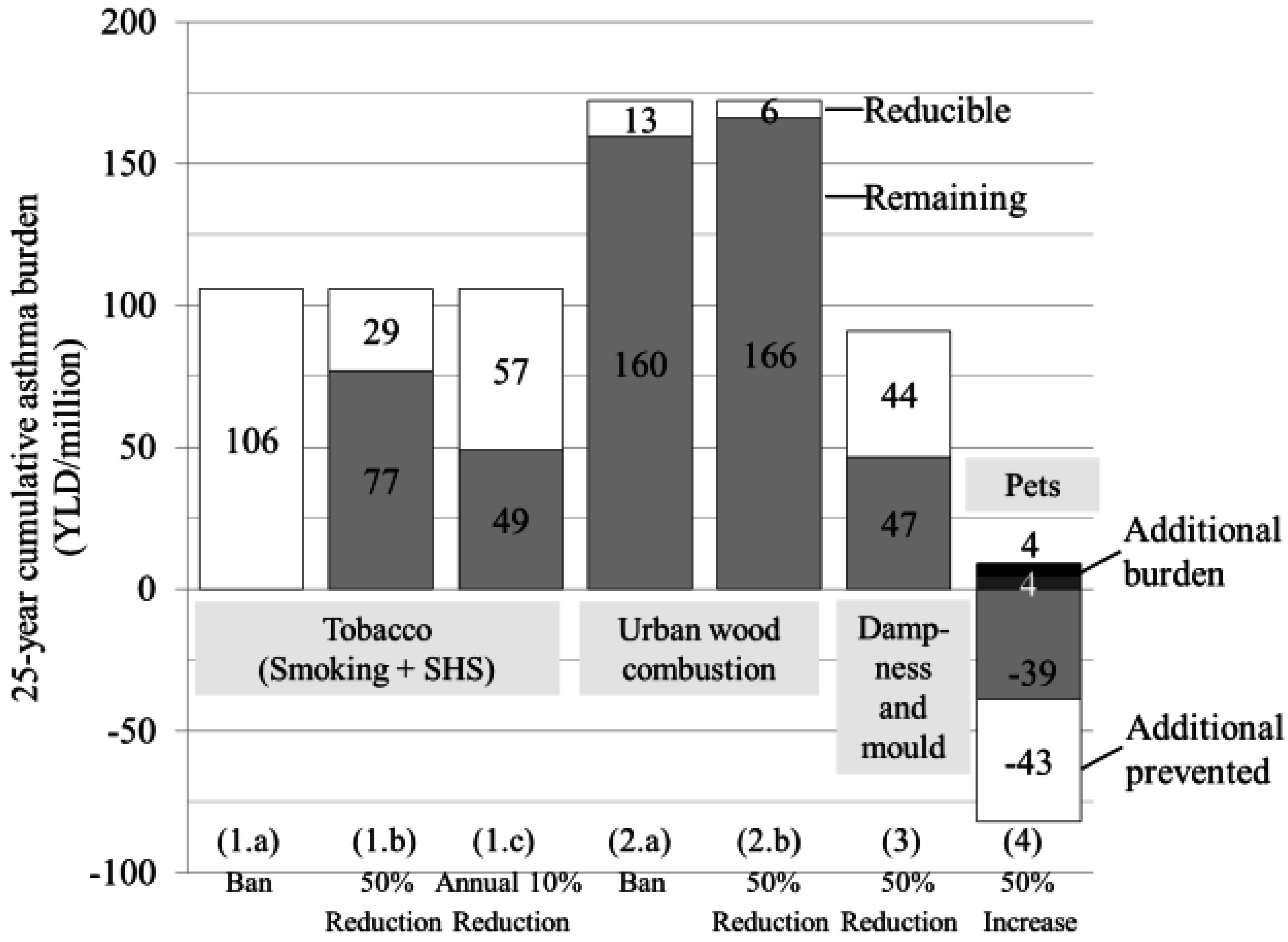
3.3. Asthma Reduction Potential
| Scenario | Exposure change | Action | 25-Year Cumulative Patient Years | |||
|---|---|---|---|---|---|---|
| Attributable | % | Reducible | % | |||
| Total asthma burden | 6,796,162 | 100 | ||||
| Attributable to risk factors studied here * | 1,208,902 | 17.8 | 726,441 # | |||
| Tobacco a | 383,209 | 5.6 | ||||
| 1a | Ban | 100% reduction in 2015 | 383,209 | 5.6 | ||
| 1b | 50% Reduction | 50% reduction in 2015 | 103,642 | 1.5 | ||
| 1c | Smoke Free Finland | 10% annual reduction in 2015–2040 | 205,930 | 3.0 | ||
| Fine particle (PM2.5) | 624,512 | 9.2 | ||||
| 2a | Ban Wood Combustion b | 100% reduction of PM2.5 fraction due to residential wood combustion in 2015 | 45,971 | 0.7 | ||
| 2b | 50 % Reduction Wood Combustion b | 50% reduction of PM2.5 fraction due to residential wood combustion in 2015 | 22,943 | 0.3 | ||
| Dampness c | 329,785 | 4.9 | ||||
| 3 | 50 % Reduction | 50% reduction in 2015 | 160,792 | 2.3 | ||
| Pets d | −128,604 | −1.8 | ||||
| 4 | 50 % Increase | 50% increase leading to exposure of 3.5% of atopic population and 46.5% exposure of non-atopic population | 136,469 | 2.0 | ||
| Feasible | Combination of actions 1.c, 2.b, 3, 4 | 526,134 | 7.7 | |||
| Most efficient | Combination of actions 1.a, 2.a, 3, 4 | 726,441 | 10.7 | |||

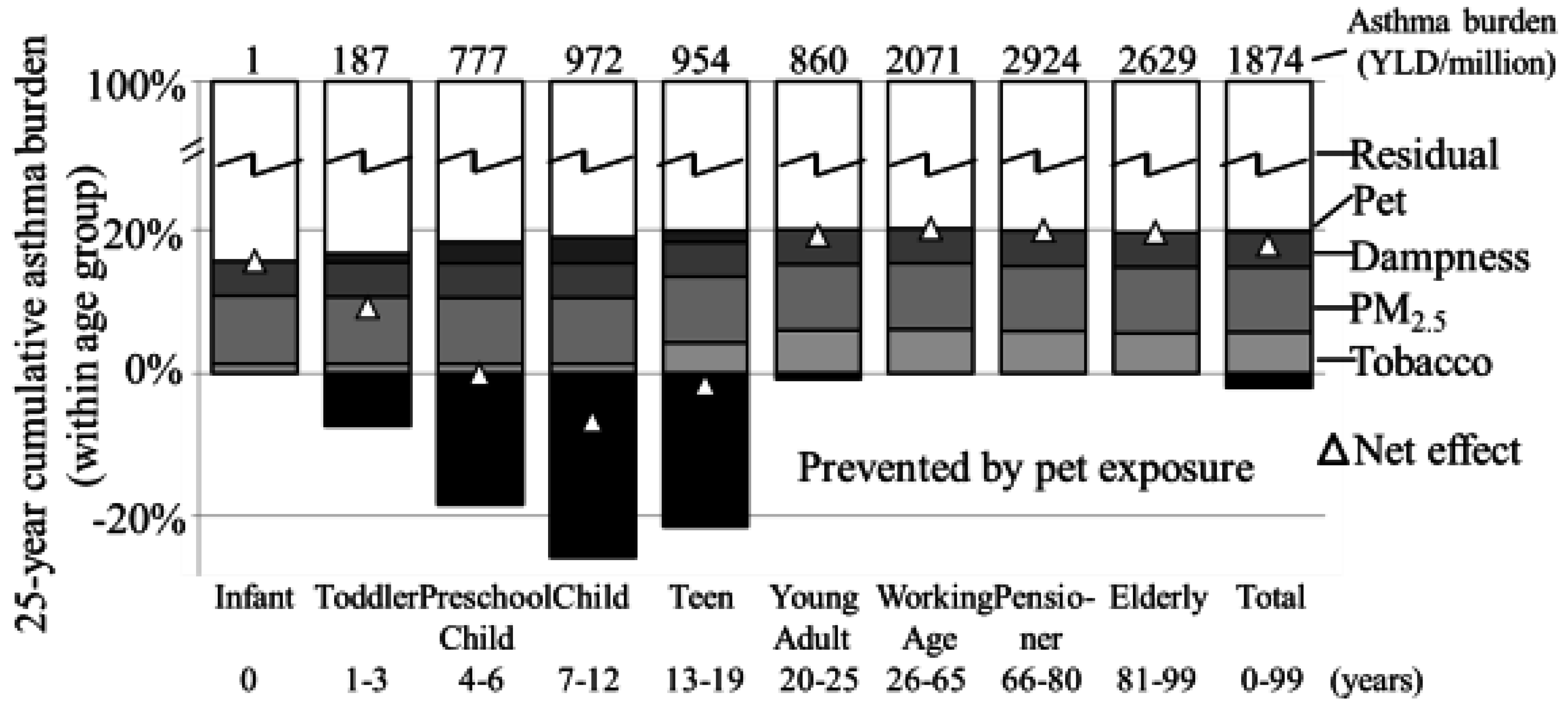
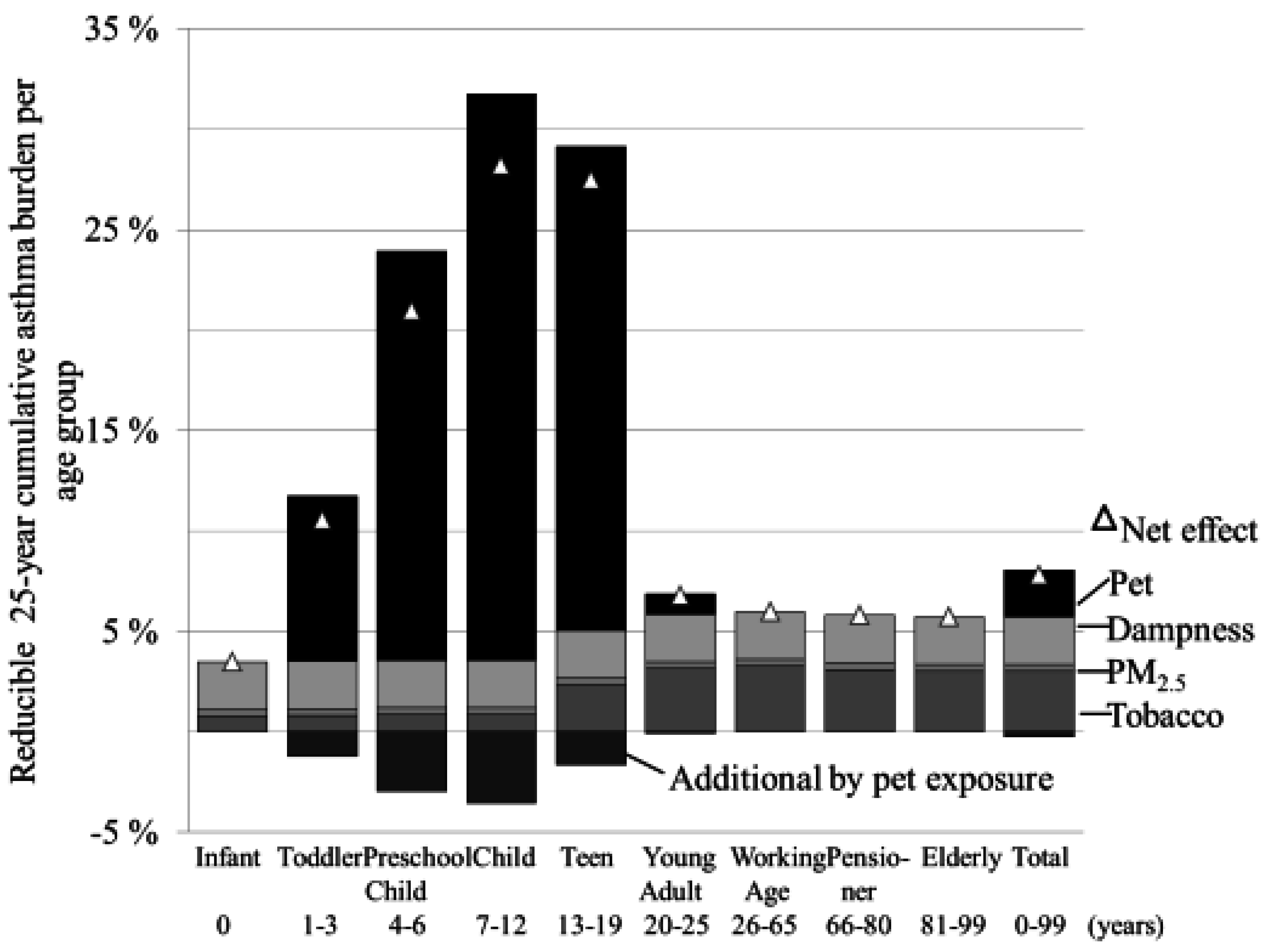
3.4. Burden of Asthma by Age Groups


4. Discussion
4.1. Model Uncertainties
4.2. Parameter Uncertainties
4.3. Scenario Uncertainties
4.4. Validity of the Burden of Disease Approach
4.5. Asthma Reduction Potential and Economic Considerations
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zeliger, H.I. Children in Human Toxicology of Chemical Mixtures: Toxic Consequences Beyond the Impact of One-Component Product and Environmental Exposures, 2nd ed.; Elsevier: Oxford, UK, 2011. [Google Scholar]
- Global Initiative for Asthma (GINA). Global Burden of Asthma. Available online: http://www.ginasthma.org/local/uploads/files/GINABurdenReport_1.pdf (accessed on 4 September 2014).
- Pallasaho, P.; Juusela, M.; Lindqvist, A.; Sovijärvi, A.; Lundbäck, B.; Rönmark, E. Allergic rhinoconjunctivitis doubles the risk for incident asthma—Results from a population study in Helsinki, Finland. Respir. Med. 2011, 105, 1449–1456. [Google Scholar] [CrossRef] [PubMed]
- Kauppi, P.; Linna, M.; Martikainen, J.; Mäkelä, M.J.; Haahtela, T. Follow-up of the Finnish Asthma Programme 2000–2010: Reduction of hospital burden needs risk group rethinking. Thorax 2012. [Google Scholar] [CrossRef] [PubMed]
- Ober, C.; Yao, T.C. The genetics of asthma and allergic disease: A 21st century perspective. Immunol. Rev. 2001, 242, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Haahtela, T.; Tuomisto, L.E.; Klaukka, T.; Pietinalho, A.; Erhola, M.; Kaila, M.; Nieminen, M.M.; Kontula, E.; Laitinen, L.A. A 10 year asthma programme in Finland: Major change for the better. Thorax 2006, 61, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Boyd, D.R.; Genius, S.J. The environmental burden of disease in Canada: Respiratory disease, cardiovascular disease, cancer and congenital affliction. Environ. Res. 2008, 106, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Langhammer, A.; Johnsen, R.; Holmen, J.; Gulsvik, A.; Bjermer, L. Cigarette smoking gives more respiratory symptoms among women than men—The Nord-trøndelag health study (HUNT). J. Epidemiol. Community Health 2000, 54, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Proposed Identification of Environmental Tobacco Smoke as a Toxic Contaminant—Part B: Health Effect Assessment for Environmental Tobacco Smoke; California Environmental Protection Agency: Sacramento, CA, USA.
- Jaakkola, M.S.; Piipari, R.; Jaakkola, N.; Jaakkola, J.J. Environmental tobacco smoke and adult-onset asthma: A population-based incident case-control study. Am. J. Public Health 2003, 93, 2055–2060. [Google Scholar] [CrossRef] [PubMed]
- Fisk, W.J.; Lei-Gomez, Q.; Mendell, M.J. Meta-analyses of the associations of respiratory health effects with dampness and mold in homes. Indoor Air 2007, 17, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.R.; Favarato, G.; Atkinson, R.W. Long-term exposure to air pollution and the incidence of asthma: Meta-analysis of cohort studies. Air Qual. Atmos. Health 2013, 6, 47–56. [Google Scholar] [CrossRef]
- Hugg, T.T.; Jaakkola, M.S.; Ruotsalainen, R.; Pushkarev, V.; Jaakkola, J.J. Exposure to animals and the risk of allergic asthma: A population-based cross-sectional study in Finnish and Russian children. Environ. Health 2008, 7, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Olmedo, O.; Goldstein, I.F.; Acosta, L.; Divjan, A.; Rundle, A.G.; Chew, G.L.; Mellins, R.B.; Hoepner, L.; Andrews, H.; Lopez-Pintado, S. Neighborhood differences in exposure and sensitization to cockroach, mouse, dust mite, cat, and dog allergens in New York City. J. Allergy Clin. Immunol. 2011, 128, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Rumrich, I. Environmental Burden of Asthma. Impact of control options and protection factors. Master’s thesis, University of Eastern Finland, Kuopio, Finland, 2014. Available online: http://urn.fi/urn:nbn:fi:uef-20141227 (accessed on 25 February 2015). [Google Scholar]
- Finnish Social Security Institution (KELA). Reimbursement for Medicine Expenses. Available online: http://www.kela.fi/web/en/reimbursement-for-medical-expenses (accessed on 14 May 2015).
- National Institute for Health and Welfare (THL). Tupakkatilasto 2012. Statistical Report 27/2013. Available online: http://www.julkari.fi/bitstream/handle/10024/110551/Tr27_13.pdf?sequence=4 (accessed on 15 July 2014).
- Hänninen, O.; Knol, A. European Perspectives on Environmental Burden of Disease: Estimates for Nine Stressors in Six European Countries; National Institute for Health and Welfare: Helsinki, Finland, 2011. [Google Scholar]
- World Health Organization (WHO). Metrics: Population Attributable Fraction (PAF). Available online: http://www.who.int/healthinfo/global_burden_disease/metrics_paf/en/ (accessed on 15 May 2014).
- Laaksonen, M. Population attributable fraction (PAF) in epidemiological follow-up studies. Ph.D. Thesis, University of Tampere, Tampere, Finland, 2010. [Google Scholar]
- Turunen, M.; Paanala, A.; Villman, J.; Nevalainen, A.; Haverinen-Shaughnessy, U. Evaluating housing quality, health and safety using an Internet-based data collection and response system: A cross-sectional study. Environ. Health 2010, 9, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Haahtela, T.; von Hertzen, L.; Mäkelä, M.; Hannuksela, M.; Allergy Programme Working Group. Finnish allergy progamme 2008–2018—Time to act and change the course. Allergy 2008, 63, 634–645. [Google Scholar]
- World Health Organization (WHO). Global Burden of Disease 2004 Update: Disability Weights for Diseases and Conditions. Available online: http://www.who.int/healthinfo/global_burden_disease/GBD2004_DisabilityWeights.pdf (accessed on 4 September 2014).
- Kutvonen, J. Ympäristöriskien torjuntatoimenpiteiden terveyshyötyjen, kustannsten ja koettujen arvojen vertailu. Master’s Thesis, University of Eastern Finland, Kuopio, Finland, 2014. Available online: http://urn.fi/urn:nbn:fi:uef-20140442 (accessed on 25 February 2015). [Google Scholar]
- Tobacco Act; Ministry of Social Affairs and Health: Helsinki, Finland, 2010.
- Hänninen, O.; Asikainen, A. Efficient Reduction of Indoor Exposures: Health Benefits from Optimizing Ventilation, Filtration and Indoor Source Controls; Report 2/2013; National Institute for Health and Welfare: Helsinki, Finland, 2013. [Google Scholar]
- Azalim, S.; Camargos, P.; Aves, A.L.; Senna, M.I.; Sakurai, E.; Schwabe Keller, W. Exposure to environmental factors and relationship to allergic rhinitis and/or asthma. Ann. Agric. Environ. Med. 2014, 21, 59–63. [Google Scholar] [PubMed]
- Schäfer, T.; Bauer, C.P.; Beyer, K.; Bufe, A.; Friedrichs, F.; Gieler, U.; Gronke, G.; Hamelmann, E.; Hellerman, M.; Kleinheins, A.; et al. S3-Leitlinie Allergieprävention—Update 2014. Allergo J. 2014, 23, 32–47. [Google Scholar]
- Collin, M.S.; Westgarth, C.; Murray, J.; Paul, E.; Sterne, J.A.C.; John Henderson, A. Pet ownership is associated with increased risk of non-atopic asthma and reduced risk of atopy in childhood: Findings from a UK birth cohort. Clin. Exp. Allergy 2015, 45, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Lødrup Carlsen, A.; Roll, S.; Carlsen, K.-H.; Mowinckel, P.; Wijga, A.H.; Brunekreed, B.; Torrent, M.; Roberts, G.; Arshad, S.A.; Kull, I.; et al. Does pet ownership in infancy lead to asthma or allergy at school age? Pooled analysis of individual participant data from 11 European birth cohorts. PLoS ONE 2012. [Google Scholar] [CrossRef] [Green Version]
- Briggs, D. Environmental pollution and the global burden of disease. Br. Med. Bull. 2003, 68, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Kainu, A.; Pallasaho, P.; Lindqvist, A.; Sovijärvi, A.; Pietinalho, A. Increase in prevalence of physician-diagnosed asthma in Helsinki during the Finnish Asthma Programme: Improved recognition of asthma in primary care? A cross-sectional cohort study. Prim. Care Respir. J. 2013, 22, 64–71. [Google Scholar]
- Haahtela, T.; Laatikainen, T.; Alenius, H.; Fyhrquist, N.; Hanski, I.; von Hertzen, L.; Jousilahti, P.; Kosunen, T.U.; Markelove, O.; Mäkelä, M.J.; et al. Hunt for the origin of allergy—Comparing the Finnish and Russian Karelia. Clin. Exp. Allergy 2015, 45, 891–901. [Google Scholar]
- Statistics Finland. Causes of Death. Appendix Tables 1a in 2012, 2011, 2010 and 2009. Available online: http://www.stat.fi/til/ksyyt/tau_en.html (accessed on 15 July 2014).
- Moisture and Mould Programme. Programme Information. Available online: http://uutiset.hometalkoot.fi/en/programme-information.html (accessed on 24 June 2014).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rumrich, I.K.; Hänninen, O. Environmental Asthma Reduction Potential Estimates for Selected Mitigation Actions in Finland Using a Life Table Approach. Int. J. Environ. Res. Public Health 2015, 12, 6506-6522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120606506
Rumrich IK, Hänninen O. Environmental Asthma Reduction Potential Estimates for Selected Mitigation Actions in Finland Using a Life Table Approach. International Journal of Environmental Research and Public Health. 2015; 12(6):6506-6522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120606506
Chicago/Turabian StyleRumrich, Isabell Katharina, and Otto Hänninen. 2015. "Environmental Asthma Reduction Potential Estimates for Selected Mitigation Actions in Finland Using a Life Table Approach" International Journal of Environmental Research and Public Health 12, no. 6: 6506-6522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120606506