
Monetary Valuation of PM10-Related Health Risks in Beijing China: The Necessity for PM10 Pollution Indemnity

Abstract
:1. Introduction
1.1. PM10-Related Health Impacts and Risks
1.2. Economic Evaluation of PM10-Related Health Impacts

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Economic Evaluation Method | Advantages | Limitation | Scope of Application |
|---|---|---|---|
| AHC |
|
|
|
| COI |
|
|
|
2. Materials and Methodology
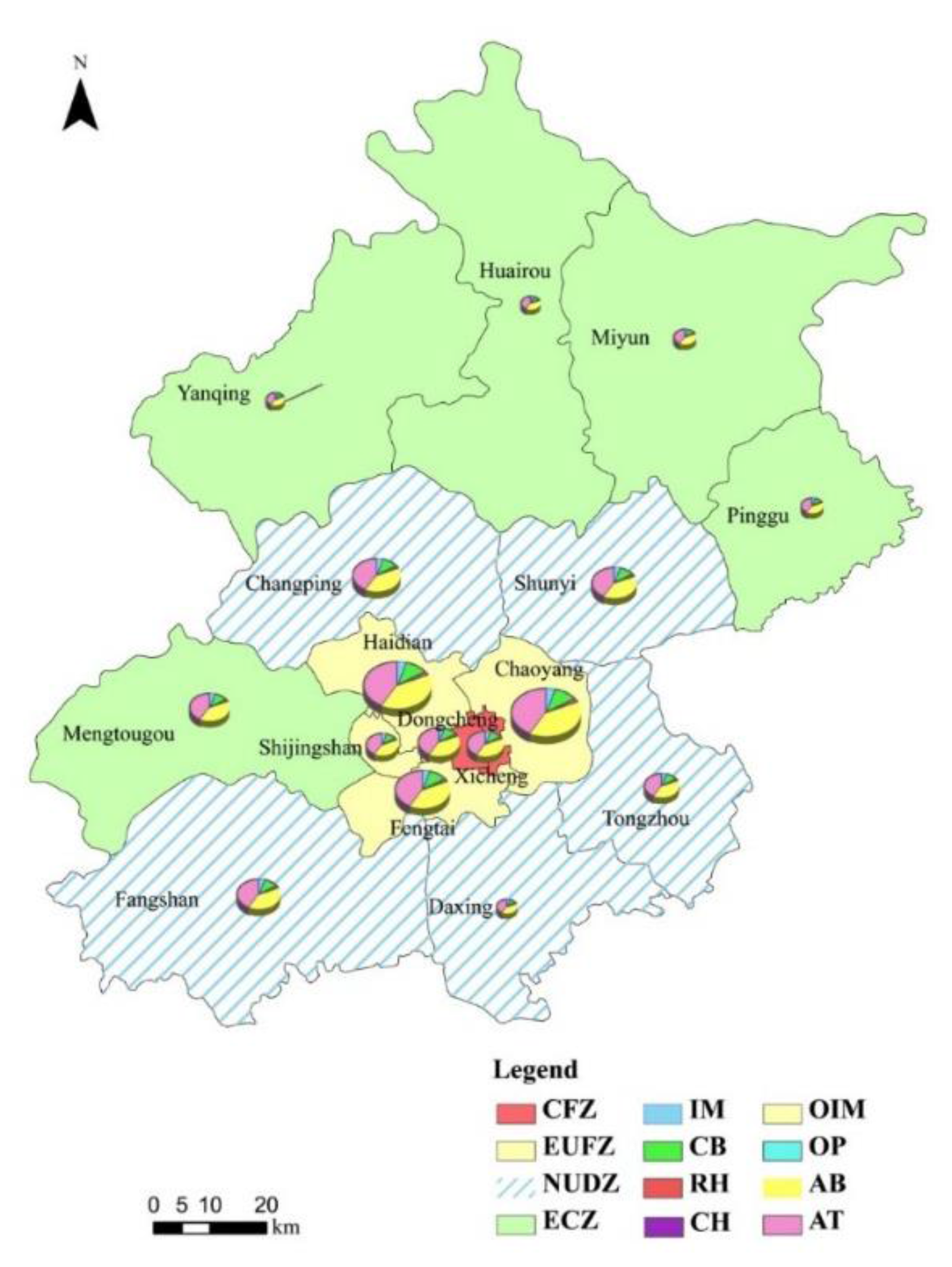
2.1. Study Area
- (1)
- The “core functional zone” (CFZ) includes the Dongcheng and Xicheng districts. The main task of this region is to strengthen city management, protect the ancient style of Beijing, improve the living environment, and develop the modern service industry.
- (2)
- The “expanding urban function zone” (EUFZ) consists of the Chaoyang, Haidian, Fengtai and Shijingshan districts. The function of this region is to expand the nationwide and worldwide export-oriented economical service function, promote scientific and technological innovation and develop high-tech industries.
- (3)
- The “new urban development zone” (NUDZ) includes the five districts of Tongzhou, Daxing, Shunyi, Fangshan and Changping. The region relies on the development of the Beijing manufacturing industry and modern agriculture. Additionally, it is also an important area to relocate industry and population from the city center and is the future economic center of Beijing.
- (4)
- The “ecological conservation zone” (ECZ) includes the five counties of Mentougou, Pinggu, Huairou, Miyun and Yanqing. This region is essential for guaranteeing the regional sustainable development of Beijing.

2.2. PM10-Related Health Risk and Impact Quantification Methods
2.2.1. Hazard Identification
2.2.2. Health Risk and Impact Assessment Method
2.2.3. Exposure-Response Coefficients Selection
| Health Endpoints | β (95% CI) | E0 |
|---|---|---|
| Individual mortality | 4.3 (2.60, 6.10) [13,14] | 0.01013 [48] |
| Chronic bronchitis | 5.77 (1.93, 9.61) [49] | 0.01390 [50] |
| Respiratory hospitalization | 1.2 (0.80, 1.60) [51] | 0.01022 [52] |
| Cardiovascular hospitalization | 0.7 (0.30, 1.10) [51] | 0.00546 [52] |
| Outpatient visits to internal medicine | 0.01374 (0.01077, 0.01679) [53] | 0.41105 [52] |
| Outpatient visits to pediatrics | 0.01551 (0.01041, 0.02060) [53] | 0.15300 [52] |
| Acute bronchitis | 5.5 (1.89, 9.11) [49] | 0.03800 [52] |
| Asthma attacks | 3.9 (1.90, 5.90) [54] | 0.05610 [55] |
2.3. Monetary Valuation Model of PM10-Related Health Risks
| Year | Medical Costs ($) | |||
|---|---|---|---|---|
| Hospitalization | Asthma Attacks | Acute Bronchitis | Outpatient Visits | |
| 2008 | 2233.94 | 255.54 | 406.77 | 52.41 |
| 2009 | 2595.36 | 293.67 | 434.19 | 54.88 |
| 2010 | 2650.59 | 319.90 | 463.47 | 57.35 |
| 2011 | 2705.81 | 346.13 | 494.72 | 59.82 |
| 2012 | 2761.04 | 372.36 | 528.08 | 59.82 |
2.4. Data Collection

3. Results and Discussion
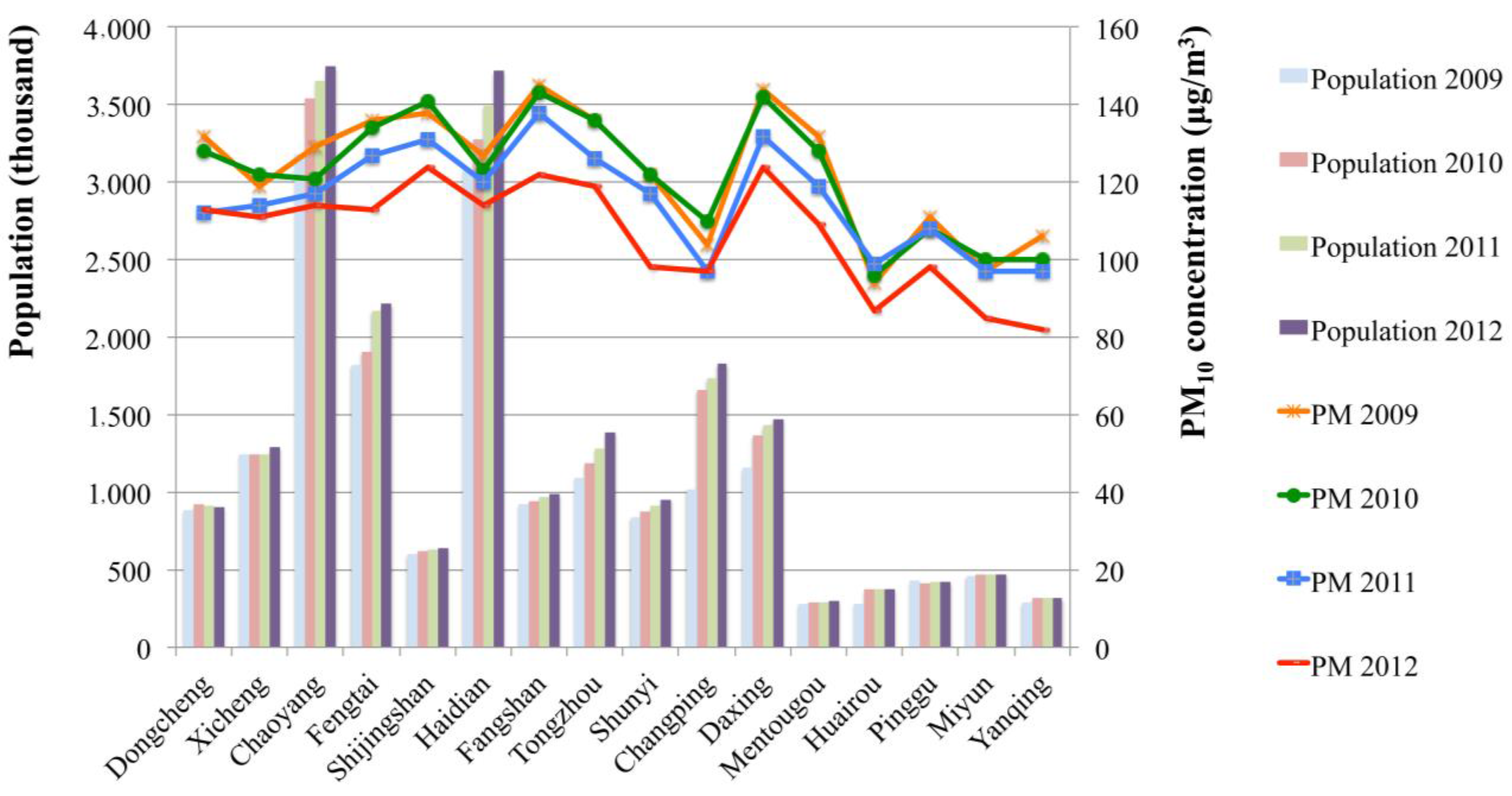
3.1. PM10-Related Health Risks in Beijing
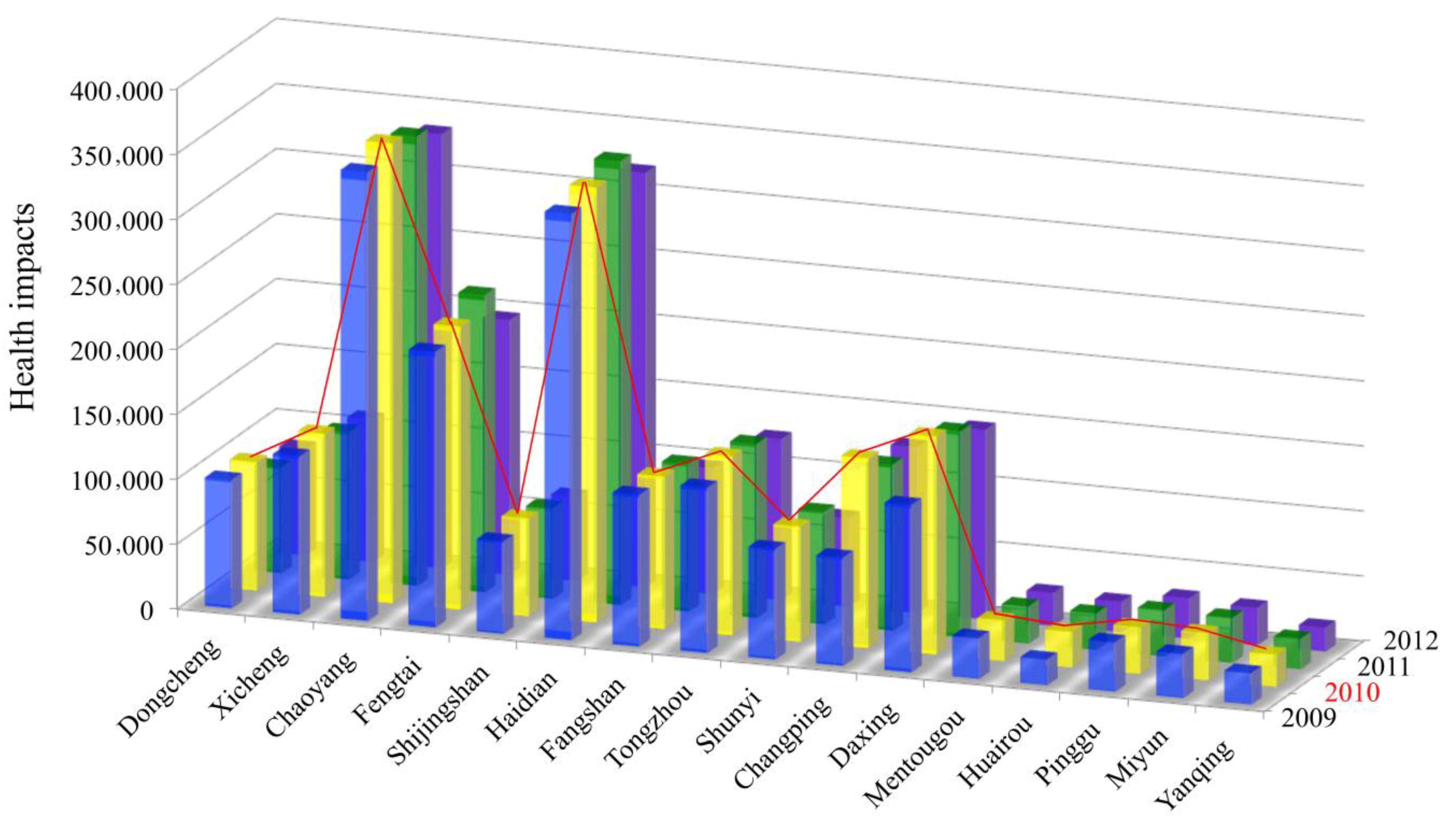
3.2. PM10-Related Health Impacts of Different Districts in Beijing
| Health Endpoints | Frequencies (95% CI) | ||||
|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | |
| Individual mortality | 0.0093 (0.0082–0.0105) | 0.0093 (0.0081–0.0104) | 0.0093 (0.0081–0.0104) | 0.0091 (0.0080–0.0101) | 0.0089 (0.0079–0.0100) |
| Chronic bronchitis | 0.0203 (0.0157–0.0249) | 0.0202 (0.0157–0.0248) | 0.0202 (0.0157–0.0248) | 0.0198 (0.0156–0.0240) | 0.0195 (0.0155–0.0235) |
| Respiratory hospitalization | 0.0115 (0.0111–0.0119) | 0.0115 (0.0110–0.0119) | 0.0115 (0.0110–0.0119) | 0.0114 (0.0110–0.0118) | 0.0113 (0.0109–0.0117) |
| Cardiovascular hospitalization | 0.0059 (0.0056–0.0061) | 0.0058 (0.0056–0.0061) | 0.0058 (0.0056–0.0061) | 0.0058 (0.0056–0.0060) | 0.0058 (0.0056–0.0060) |
| Outpatient visits to internal medicine | 0.4116 (0.4115–0.4118) | 0.4116 (0.4115–0.4117) | 0.4116 (0.4115–0.4116) | 0.4116 (0.4115–0.4117) | 0.4116 (0.4114–0.4117) |
| Outpatient visits to pediatrics | 0.1532 (0.1532–0.1533) | 0.1532 (0.1532–0.1533) | 0.1532 (0.1532–0.1533) | 0.1532 (0.1531–0.1533) | 0.1532 (0.1531–0.1533) |
| Acute bronchitis | 0.0593 (0.0453–0.0733) | 0.0591 (0.0453–0.0730) | 0.0591 (0.0453–0.0730) | 0.0576 (0.0448–0.0705) | 0.0566 (0.0444–0.0688) |
| Asthma attacks | 0.0784 (0.0670–0.0899) | 0.0782 (0.0669–0.0895) | 0.0782 (0.0669–0.0895) | 0.0767 (0.0661–0.0872) | 0.0756 (0.0656–0.0856) |
| Health Endpoints | Number of Cases | ||||
|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | |
| Individual mortality | 55,844 | 57,196 | 63,910 | 60,800 | 58,675 |
| Chronic bronchitis | 126,528 | 129,592 | 144,803 | 137,745 | 132,921 |
| Respiratory hospitalization | 22,400 | 22,954 | 25,648 | 24,493 | 23,706 |
| Cardiovascular hospitalization | 6833 | 7003 | 7825 | 7482 | 7248 |
| Outpatient visits to internal medicine | 9771 | 10,018 | 11,194 | 10,726 | 10,406 |
| Outpatient visits to pediatrics | 4106 | 4210 | 4704 | 4507 | 4373 |
| Acute bronchitis | 431,698 | 442,139 | 494,037 | 469,848 | 453,285 |
| Asthma attacks | 436,235 | 446,815 | 499,261 | 475,068 | 458,547 |
| All | 1,093,415 | 1,119,927 | 1,251,383 | 1,190,669 | 1,149,161 |


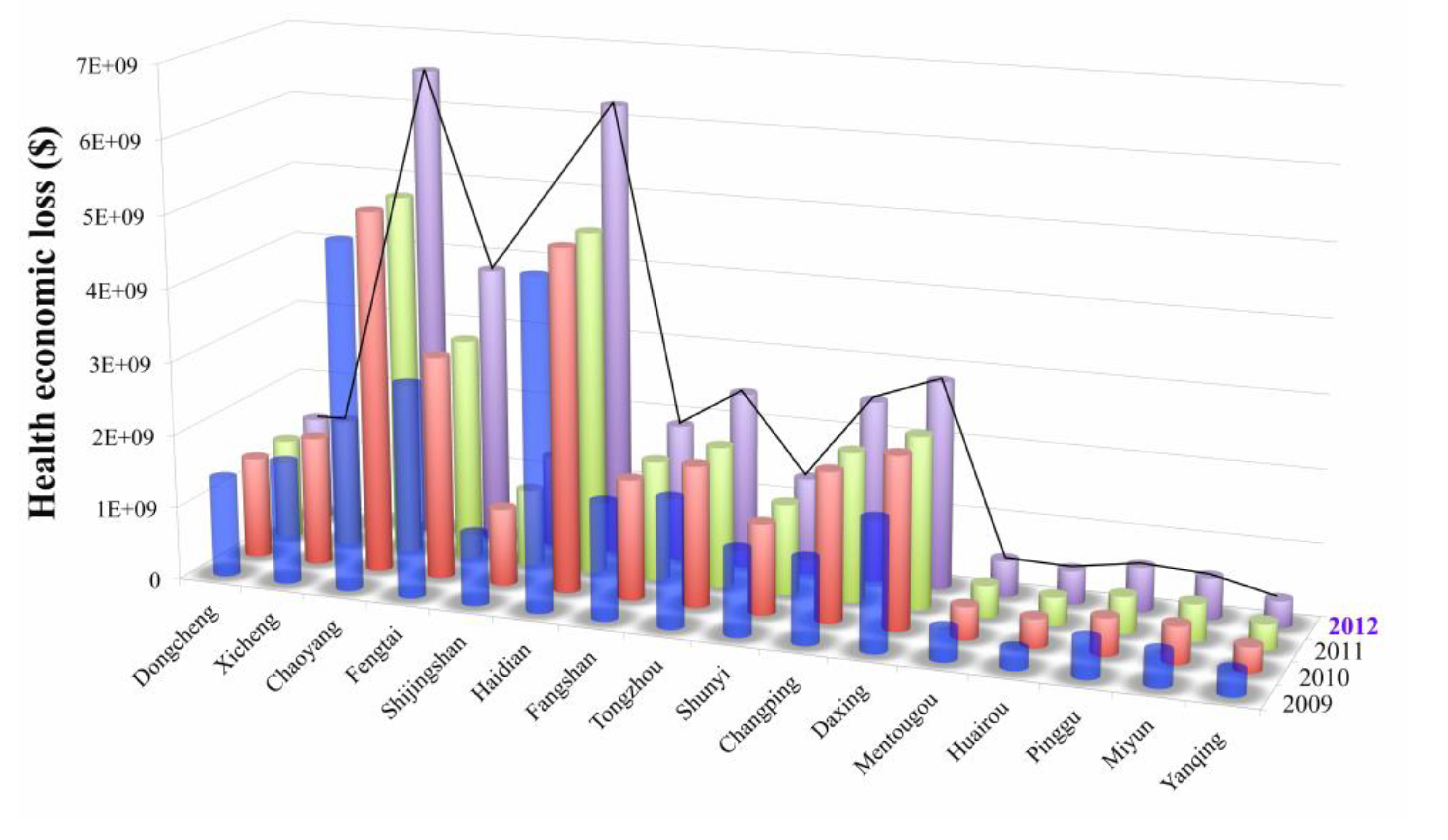
3.3. Monetary Costs of PM10-Related Health Impacts in Beijing
| Health Endpoints | Economic Loss ($) | ||||
|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | |
| Individual mortality | 1.35E + 10 | 1.41E + 10 | 1.71E + 10 | 1.77E + 10 | 1.79E + 10 |
| Chronic bronchitis | 9.82E + 09 | 1.03E + 10 | 1.24E + 10 | 1.28E + 10 | 1.30E + 10 |
| Respiratory hospitalization | 6.12E + 07 | 7.06E + 07 | 7.96E + 07 | 7.70E + 07 | 7.49E + 07 |
| Cardiovascular hospitalization | 1.87E + 07 | 2.15E + 07 | 2.43E + 07 | 2.35E + 07 | 2.29E + 07 |
| Outpatient visits to internal medicine | 5.15E + 05 | 5.54E + 05 | 6.37E + 05 | 6.26E + 05 | 6.23E + 05 |
| Outpatient visits to pediatrics | 2.17E + 05 | 2.33E + 05 | 2.68E + 05 | 2.63E + 05 | 2.62E + 05 |
| Acute bronchitis | 1.04E + 07 | 1.15E + 07 | 1.39E + 07 | 1.40E + 07 | 1.42E + 07 |
| Asthma attacks | 1.20E + 08 | 1.38E + 08 | 1.66E + 08 | 1.67E + 08 | 1.71E + 08 |
| Total loss | 2.36E + 10 | 2.46E + 10 | 2.98E + 10 | 3.08E + 10 | 3.12E + 10 |
3.4. Discussion
3.4.1. Monetary Valuation Based on Different Districts in Beijing


3.4.2. Monetary Valuation Based on Different Functional Zones in Beijing
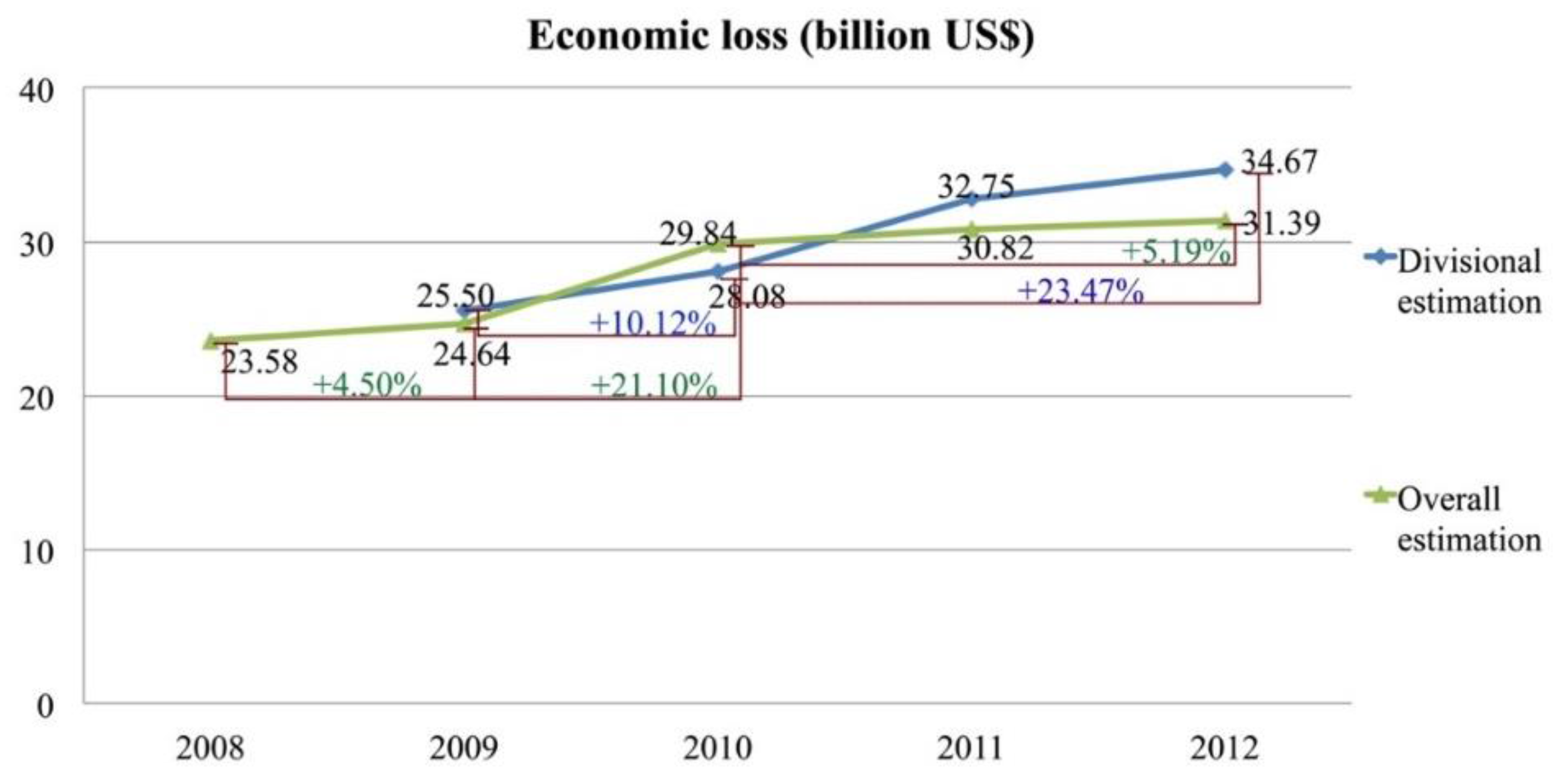
3.4.3. Overall Monetary Valuation in Beijing

3.4.4. PM10 Pollution Control Policies in Beijing from 2008 to 2012
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Liao, X.; Zhang, Y. Economic impacts of shifting sloping farm lands to alternative uses. Agric. Syst. 2008, 97, 48–55. [Google Scholar] [CrossRef]
- Sueyoshi, T.; Yuan, Y. China’s regional sustainability and diversified resource allocation: DEA environmental assessment on economic development and air pollution. Energy Econ. 2015, 49, 239–256. [Google Scholar] [CrossRef]
- Oh, H.; Ho, C.; Kim, J.; Chen, D.; Lee, S.; Choi, Y.S.; Chang, L.S.; Song, C.K. Long-range transport of air pollutants originating in China: A possible major cause of multi-day high-PM10 episodes during cold season in Seoul, Korea. Atmos. Environ. 2015, 109, 23–30. [Google Scholar] [CrossRef]
- Saenz de Miera, O.; Rosselló, J. Modeling tourism impacts on air pollution: The case study of PM10 in Mallorca. Tour. Manag. 2014, 40, 273–281. [Google Scholar] [CrossRef]
- Likhvar, V.N.; Pascal, M.; Markakis, K.; Colette, A.; Hauglustaine, D.; Valari, M.; Klimont, Z.; Medina, S.; Kinney, P. A multi-scale health impact assessment of air pollution over the 21st century. Sci. Total Environ. 2015, 514, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Perrone, M.; Gualtieri, M.; Consonni, V.; Ferrero, L.; Sangiorgi, G.; Longhin, E.; Ballabio, D.; Bolzacchini, E.; Camatini, M. Particle size, chemical composition, seasons of the year and urban, rural or remote site origins as determinants of biological effects of particulate matter on pulmonary cells. Environ. Pollut. 2013, 176, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Ormstad, H.; Gaarder, P.I.; Johansen, B. Quantification and characterisation of suspended particulate matter in indoor air. Sci. Total Environ. 1997, 193, 185–196. [Google Scholar] [CrossRef]
- Happo, M.; Markkanen, A.; Markkanen, P.; Jalava, P.; Kuuspalo, K.; Leskinen, A.; Sippula, O.; Lehtinen, K.; Jokiniemi, J.; Hirvonen, M.R. Seasonal variation in the toxicological properties of size-segregated indoor and outdoor air particulate matter. Toxicol. Vitr. 2013, 27, 1550–1561. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.; Yang, Z.; Zhang, S. Ecological risk assessment of heavy metals in sediment and human health risk assessment of heavy metals in fishes in the middle and lower reaches of the yangtze river basin. Environ. Pollut. 2011, 159, 2575–2585. [Google Scholar] [CrossRef] [PubMed]
- Romanazzi, V.; Casazza, M.; Malandrino, M.; Maurino, V.; Piano, A.; Schilirò, T.; Gilli, G. PM10 size distribution of metals and environmental-sanitary risk analysis in the city of Torino. Chemosphere 2014, 112, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Laden, F.; Schwartz, J.; Speizer, F.E.; Dockery, D.W. Reduction in fine particulate air pollution and mortality—Extended follow-up of the Harvard six cities study. Am. J. Respir. Crit. Care Med. 2006, 173, 667–672. [Google Scholar] [CrossRef] [PubMed]
- An, X.; Hou, Q.; Li, N.; Zhai, S. Assessment of human exposure level to PM10 in China. Atmos. Environ. 2013, 70, 376–386. [Google Scholar] [CrossRef]
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Ferris, B.G., Jr.; Speizer, F.E.; Fay, M.E. An association between air pollution and mortality in six US cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W., Jr. Particulate air pollution as a predictor of mortality in a prospective study of US adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Slezakova, K.; Castro, D.; Delerue Matos, C.; Alvim Ferraz, M.D.C.; Morais, S.; Pereira, M.D.C. Impact of vehicular traffic emissions on particulate-bound PAHs: Levels and associated health risks. Atmos. Res. 2013, 127, 141–147. [Google Scholar] [CrossRef]
- Xu, L.; Xie, X.; Li, S. Correlation analysis of the urban heat island effect and the spatial and temporal distribution of atmospheric particulates using TM images in Beijing. Environ. Pollut. 2013, 178, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Yin, H.; Xie, X. Health risk assessment of inhalable particulate matter in Beijing based on the thermal environment. Int. J. Environ. Res. Public Health 2014, 11, 12368–12388. [Google Scholar] [CrossRef] [PubMed]
- Amador-Muñoz, O.; Bazán-Torija, S.; Villa-Ferreira, S.A.; Villalobos-Pietrini, R.; Bravo-Cabrera, J.L.; Munive-Colín, Z.; Hernández-Mena, L.; Saldarriaga-Noreña, H.; Murillo-Tovar, M.A. Opposing seasonal trends for polycyclic aromatic hydrocarbons and PM10: Health risk and sources in southwest Mexico City. Atmos. Res. 2013, 122, 199–212. [Google Scholar] [CrossRef]
- Hanedar, A.; Alp, K.; Kaynak, B.; Baek, J.; Avsar, E.; Odman, M.T. Concentrations and sources of PAHs at three stations in Istanbul, Turkey. Atmos. Res. 2011, 99, 391–399. [Google Scholar] [CrossRef]
- Xu, L.; Shu, X. Aggregate human health risk assessment from dust of daily life in the urban environment of Beijing. Risk Anal. 2014, 34, 670–682. [Google Scholar] [CrossRef] [PubMed]
- Hou, Q.; An, X.; Wang, Y.; Tao, Y.; Sun, Z. An assessment of China’s PM10-related health economic losses in 2009. Sci. Total Environ. 2012, 435–436, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Liu, Y.; Yin, J.; Zhang, M.; Zhang, T. Chemical characteristics and source apportionment of PM10 during Asian dust storm and non-dust storm days in Beijing. Atmos. Environ. 2014, 91, 85–94. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Y.; Ying, Q.; Zhang, H. Spatial and temporal variability of PM2.5 and PM10 over the north China plain in the Yangtze River Delta, China. Atmos. Environ. 2014, 95, 598–609. [Google Scholar] [CrossRef]
- Zhao, N.; Qiu, J.; Zhang, Y.; He, X.; Zhou, M.; Li, M.; Xu, X.; Cui, H.; Lv, L.; Lin, X.; et al. Ambient air pollutant PM10 and risk of preterm birth in Lanzhou, China. Environ. Int. 2015, 76, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Ragas, A.M.J.; Oldenkamp, R.; Preeker, N.L.; Wernicke, J.; Schlink, U. Cumulative risk assessment of chemical exposures in urban environments. Environ. Int. 2011, 37, 872–881. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; He, L. Welfare loss of China’s air pollution: How to make personal vehicle transportation policy. China Econ. Rev. 2014, 31, 106–118. [Google Scholar] [CrossRef]
- Pizzol, M.; Weidema, B.; Brandão, M.; Osset, P. Monetary valuation in life cycle assessment: A review. J. Clean. Prod. 2015, 86, 170–179. [Google Scholar] [CrossRef]
- Dong, C.; Huang, G.H.; Cai, Y.P.; Liu, Y. Robust planning of energy management systems with environmental and constraint-conservative considerations under multiple uncertainties. Energy Convers. Manage. 2013, 65, 471–486. [Google Scholar] [CrossRef]
- Valente, C.; Spinelli, R.; Hillring, B.G. Lca of environmental and socio-economic impacts related to wood energy production in alpine conditions: Valle di fiemme (Italy). J. Clean. Prod. 2011, 19, 1931–1938. [Google Scholar] [CrossRef]
- Tang, D.; Wang, C.; Nie, J.; Chen, R.; Niu, Q.; Kan, H.; Chen, B.; Perera, F. Health benefits of improving air quality in Taiyuan, China. Environ. Int. 2014, 73, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Othman, J.; Sahani, M.; Mahmud, M.; Sheikh Ahmad, M.K. Transboundary smoke haze pollution in malaysia: Inpatient health impacts and economic valuation. Environ. Pollut. 2014, 189, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Tian, H.; Cheng, K.; Lu, L.; Zheng, M.; Wang, S.; Hao, J.; Wang, K.; Hua, S.; Zhu, C.; et al. The variation of chemical characteristics of PM2.5 and PM10 and formation causes during two haze pollution events in urban Beijing, China. Atmos. Environ. 2015, 107, 1–8. [Google Scholar] [CrossRef]
- Voorhees, A.S.; Wang, J.; Wang, C.; Zhao, B.; Wang, S.; Kan, H. Public health benefits of reducing air pollution in Shanghai: A proof-of-concept methodology with application to Benmap. Sci. Total Environ. 2014, 485–486, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Xu, Y.; Zhang, S. Will joint regional air pollution control be more cost-effective? An empirical study of China’s Beijing-Tianjin-Hebei region. J. Environ. Manag. 2015, 149, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; Chen, B. Particulate air pollution in urban areas of Shanghai, China: Health-based economic assessment. Sci. Total Environ. 2004, 322, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Aunan, K.; Martin Seip, H.; Larssen, S.; Liu, J.; Zhang, D. The assessment of health damage caused by air pollution and its implication for policy making in Taiyuan, Shanxi, China. Energy Policy 2010, 38, 491–502. [Google Scholar] [CrossRef]
- Zhang, M.; Song, Y.; Cai, X.; Zhou, J. Economic assessment of the health effects related to particulate matter pollution in 111 Chinese cities by using economic burden of disease analysis. J. Environ. Manag. 2008, 88, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Guttikunda, S.K.; Carmichael, G.R.; Wang, Y.; Liu, Z.; Stanier, C.O.; Saide, P.E.; Yu, M. Health impacts and economic losses assessment of the 2013 severe haze event in Beijing area. Sci. Total Environ. 2015, 511, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.H.; Tseng, C.H. Cost-benefit analysis of sustainable energy development using life-cycle co-benefits assessment and the system dynamics approach. Appl. Energy 2014, 119, 57–66. [Google Scholar] [CrossRef]
- Li, H.; Liu, Q.; Li, B.; Fraumeni, B.; Zhang, X. Human capital estimates in China: New panel data 1985-2010. China Econ. Rev. 2014, 30, 397–418. [Google Scholar] [CrossRef]
- Ministry of Environmental Protection of the People’s Republic of China, (MEPC). Ambient Air Quality Standards. Available online: http://kjs.mep.gov.cn/hjbhbz/bzwb/dqhjbh/dqhjzlbz/201203/t20120302_224165.htm (accessed on 6 April 2015).
- Sun, Z.; An, X.; Tao, Y.; Hou, Q. Assessment of population exposure to PM10 for respiratory disease in Lanzhou (China) and its health-related economic costs based on GIS. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Yu, D.; Jing, L.; Xu, X. Air pollution and daily mortality in Shenyang, China. Arch. Environ. Health Int. J. 2000, 55, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A. Synoptic weather modeling and estimates of the exposure-response relationship between daily mortality and particulate air pollution. Environ. Health Perspect. 1996, 104, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Zanobetti, A. Using meta-smoothing to estimate dose-response trends across multiple studies, with application to air pollution and daily death. Epidemiology 2000, 11, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Mauzerall, D.L. Evaluating impacts of air pollution in China on public health: Implications for future air pollution and energy policies. Atmos. Environ. 2006, 40, 1706–1721. [Google Scholar] [CrossRef]
- National Bureau of Statistics of the People’s Republic of China. China Population Statistics Yearbook 2002; China Statistics Press: Beijing, China, 2002.
- Jing, L.; Qin, Y.; Xu, Z.; Ren, C.; Wang, S.; Ren, L. Relationship between air pollution and acute and chronic respiratory disease in Benxi. J. Environ. Health 2000, 17, 268–302. [Google Scholar]
- Ministry of Health of People’s Republic of China. Report of the Second National Health Service Survey; Peking Union Medical College: Beijing, China, 1998. (In Chinese)
- Aunan, K.; Pan, X.C. Exposure-response functions for health effects of ambient air pollution applicable for China—A meta-analysis. Sci. Total Environ. 2004, 329, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Zhang, S. Health benefit evaluation for PM2.5 pollution control in Beijing-Tianjin-Hebei region of China. China Environ. Sci. 2013, 33, 166–174. [Google Scholar]
- Wan, Y.; Yang, H.; Masui, T. Air pollution-induced health impacts on the national economy of China: Demonstration of a computable general equilibrium approach. Rev. Environ. Health 2005, 20, 119–140. [Google Scholar] [PubMed]
- Hiltermann, T.J.N.; Stolk, J.; Van Der Zee, S.C.; Brunekreef, B.; De Bruijne, C.R.; Fischer, P.H.; Ameling, C.B.; Sterk, P.J.; Hiemstra, P.S.; van Bree, L. Asthma severity and susceptibility to air pollution. Eur. Respir. J. 1998, 11, 686–693. [Google Scholar] [PubMed]
- Chen, C.; Chen, D.; Green, C.; Wu, C. Benefits of expanded use of natural gas for pollutant reduction and health improvement in Shanghai. Sinosphere J. 2002, 5, 58–64. [Google Scholar]
- National Bureau of Statistics of the People’s Republic of China. China Population Statistics Yearbook 2009–2013; China Statistics Press: Beijing, China, 2009.
- Beijing Municipal Environmental Protection Bureau (BMEP). Beijing Environmental Statement. Available online: http://www.Bjepb.Gov.Cn/bjepb/323474/324034/324735/index.Html (accessed on 24 March 2015).
- Janhäll, S. Review on urban vegetation and particle air pollution—Deposition and dispersion. Atmos. Environ. 2015, 105, 130–137. [Google Scholar] [CrossRef]
- Zhang, B.; Li, N.; Wang, S. Effect of urban green space changes on the role of rainwater runoff reduction in Beijing, China. Landsc. Urban Plan. 2015, 140, 8–16. [Google Scholar] [CrossRef]
- Wang, Z.; Pan, L.; Li, Y.; Zhang, D.; Ma, J.; Sun, F.; Xu, W.; Wang, X. Assessment of air quality benefits from the national pollution control policy of thermal power plants in China: A numerical simulation. Atmos. Environ. 2015, 106, 288–304. [Google Scholar] [CrossRef]
- Wen, C.; Gao, X.; Yu, Y.; Wu, J.; Xu, M.; Wu, H. Emission of inorganic PM10 from included mineral matter during the combustion of pulverized coals of various ranks. Fuel 2015, 140, 526–530. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yin, H.; Xu, L.; Cai, Y. Monetary Valuation of PM10-Related Health Risks in Beijing China: The Necessity for PM10 Pollution Indemnity. Int. J. Environ. Res. Public Health 2015, 12, 9967-9987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120809967
Yin H, Xu L, Cai Y. Monetary Valuation of PM10-Related Health Risks in Beijing China: The Necessity for PM10 Pollution Indemnity. International Journal of Environmental Research and Public Health. 2015; 12(8):9967-9987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120809967
Chicago/Turabian StyleYin, Hao, Linyu Xu, and Yanpeng Cai. 2015. "Monetary Valuation of PM10-Related Health Risks in Beijing China: The Necessity for PM10 Pollution Indemnity" International Journal of Environmental Research and Public Health 12, no. 8: 9967-9987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120809967