
Statistical Validation of a Web-Based GIS Application and Its Applicability to Cardiovascular-Related Studies

Abstract
:1. Background
- (1)
- Internal consistency reliability: How well does the sum score of the selected CVD-related geospatial items (CVD geospatial variables) capture the expected score in the entire domain?
- (2)
- Construct validity: How well do the CVD geospatial variables generated by the DCC GIS application measure the same construct or idea?
- (3)
- Criterion related validity: How well do the CVD geospatial variables correlate with neighborhood socioeconomic status (SES)?
- (4)
- Discriminant validity: How well do CVD geospatial variables discriminate severe hypertension cases from healthy controls?
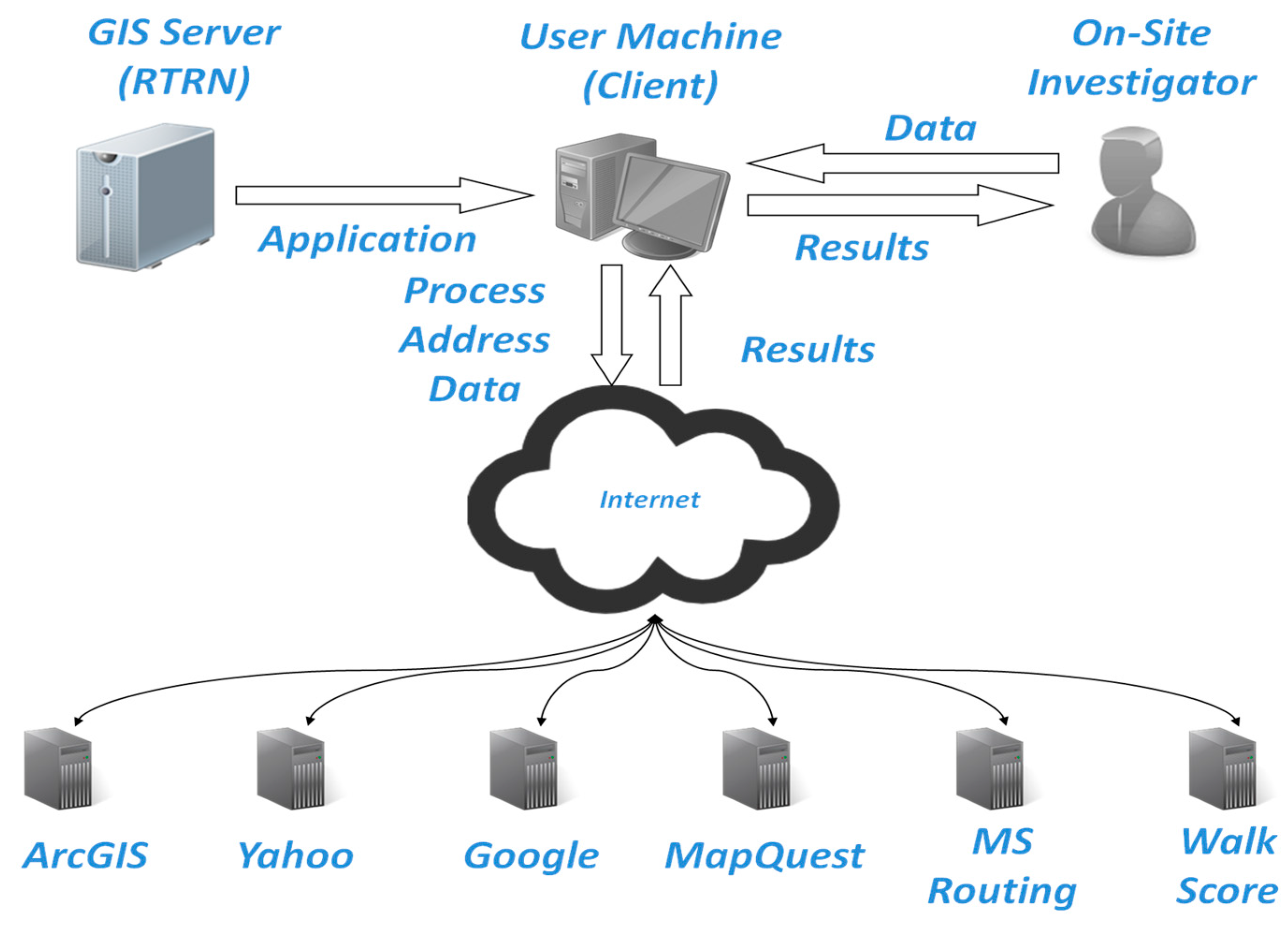
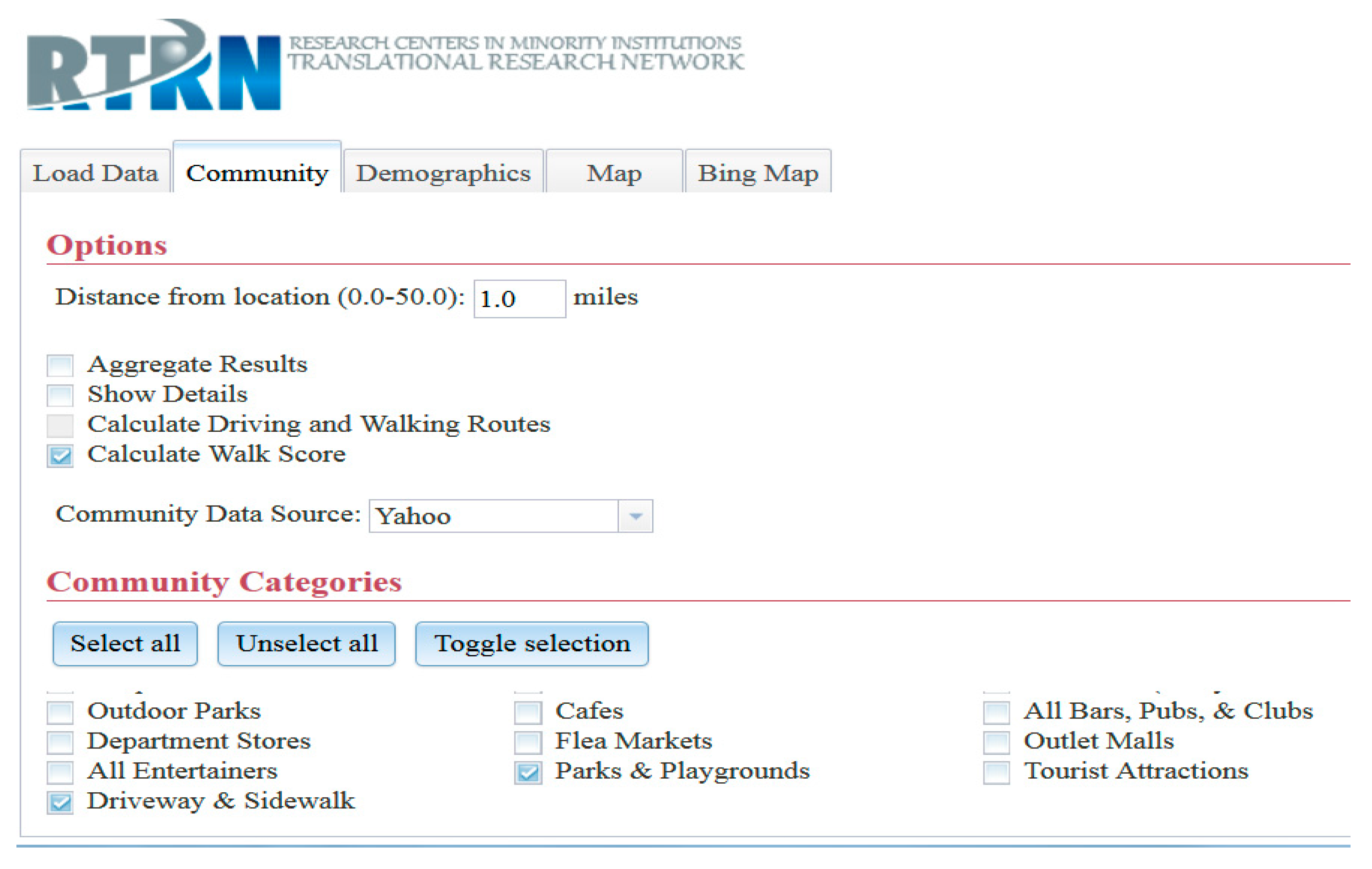
Overview of the RTRN-DCC Web-Based GIS Application


2. Methods
2.1. Procedures for GIS Data Capturing
2.2. Major Neighborhood-Level Measures
2.3. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Cardiovacular Factors | Raw Variables | Standardized Variables | ||
|---|---|---|---|---|
| Correlation with Total | Alpha (0.776) * | Correlation with Total | Alpha (0.955) * | |
| Smart Walk Score | 0.732 | 0.868 | 0.754 | 0.964 |
| Hospital/Clinics within a mile | 0.837 | 0.726 | 0.877 | 0.943 |
| Fast food Restaurants w/in a mile | 0.893 | 0.76 | 0.93 | 0.934 |
| Parks/play grounds within a mile | 0.913 | 0.727 | 0.931 | 0.934 |
| Sidewalks/driveways within a mile | 0.781 | 0.653 | 0.879 | 0.943 |
| Cardiovascular Factors | Walk Score | Hospitals | Fast-Food | Parks | Sideway |
|---|---|---|---|---|---|
| Smart Walk Score | 1 | 0.715 | 0.729 | 0.773 | 0.648 |
| <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| # Hospitals | 0.715 | 1 | 0.89 | 0.847 | 0.792 |
| <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| # Fast food Restaurants | 0.729 | 0.89 | 1 | 0.876 | 0.903 |
| <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| # Parks/Playgrounds | 0.773 | 0.847 | 0.876 | 1 | 0.905 |
| <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| # Sidewalks/Driveways | 0.648 | 0.792 | 0.903 | 0.905 | 1 |
| <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| Factor Pattern | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 |
|---|---|---|---|---|---|
| Smart Walk Score | 0.833 | 0.545 | 0.071 | 0.053 | 0.035 |
| Hospital/Clinics | 0.923 | −0.048 | −0.364 | −0.09 | 0.067 |
| Fast food Restaurants | 0.958 | −0.131 | −0.071 | 0.215 | −0.116 |
| Parks/Play grounds | 0.958 | −0.036 | 0.145 | −0.223 | −0.103 |
| Sidewalks/Driveways | 0.927 | −0.269 | 0.223 | 0.049 | 0.129 |
| Variance Explained | 4.24 (85%) | 0.39(8%) | 0.21 (4%) | 0.11 (2%) | 0.05 (1%) |
| Neighborhood Socio-Economic Factors | Correlation Coefficients with Walk Score | p-Value |
|---|---|---|
| Annual Population Growth Rate | −0.024 | 0.5919 |
| Diversity Index | 0.138 | 0.0023 |
| Labor Force Rate | −0.066 | 0.1462 |
| Median Age | −0.018 | 0.6867 |
| Median Home Value | −0.045 | 0.3197 |
| Median Household Income | −0.181 | <0.0001 |
| % Owner Occupied | −0.44 | <0.0001 |
| Unemployment Rate | 0.021 | 0.6466 |
| Social Vulnerability | 0.027 | 0.5552 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Fradgley, E.A.; Paul, C.L.; Bryant, J. A systematic review of barriers to optimal outpatient specialist services for individuals with prevalent chronic diseases: What are the unique and common barriers experienced by patients in high income countries? Int. J. Equity Health 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.T.; Iqbal, U.; Ko, H.L.; Wu, C.R.; Chiu, H.T.; Lin, Y.C.; Lin, W.; Elsa, Y.H. The relationship between accessibility of healthcare facilities and medical care utilization among the middle-aged and elderly population in Taiwan. Int. J. Qual. Health Care 2015, 27, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Hossain, W.A.; Ehtesham, M.W.; Salzman, G.A.; Jenson, R.; Calkins, C.F. Healthcare access and disparities in chronic medical conditions in urban populations. South Med. J. 2013, 106, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.A.; Elliott, M.; Glanz, K.; Haire-Joshu, D.; Lovegreen, S.L.; Saelens, B.E.; Sallis, J.F.; Brownson, R.C. Impact of the food environment and physical activity environment on behaviors and weight status in rural U.S. communities. Prev. Med. 2008, 47, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Cardinal, B.J.; Vongjaturapat, N. Built environment and changes in blood pressure in middle aged and older adults. Prev. Med. 2009, 48, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Leslie, T.; Pawloski, L.; Kallman-Price, J.; Escheik, C.; Hossain, N.; Fang, Y.; Gerber, L.H.; Younossi, Z.M. Survey of health status, nutrition and geography of food selection of chronic liver disease patients. Ann. Hepatol. 2014, 13, 533–540. [Google Scholar] [PubMed]
- Aytur, S.A.; Jones, S.A.; Stransky, M.; Evenson, K.R. Measuring physical activity in outdoor community recreational environments: Implications for research, policy, and practice. Curr. Cardiovasc. Risk Rep. 2015. [Google Scholar] [CrossRef] [PubMed]
- Salvo, D.; Reis, R.S.; Stein, A.D.; Rivera, J.; Martorell, R.; Pratt, M. Characteristics of the built environment in relation to objectively measured physical activity among Mexican adults, 2011. Prev. Chronic Dis. 2014. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.S.; Lamb, K.E.; Wang, Y.; Ogilvie, D.; Ellaway, A. Access to recreational physical activities by car and bus: An assessment of socio-spatial inequalities in mainland Scotland. PLoS ONE 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu, V.H.; Le, X.Q.; Pham, N.H.; Hens, L. Application of GIS and modelling in health risk assessment for urban road mobility. Environ. Sci. Pollut. Res. Int. 2013, 20, 5138–5149. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Sallis, J.F.; Owen, N.; de Bourdeaudhuij, I.; Cerin, E.; Sugiyama, T.; Reis, R.; Sarmiento, O.; Frömel, K.; Mitás, J.; et al. Advancing science and policy through a coordinated international study of physical activity and built environments: IPEN adult methods. J. Phys. Act. Health 2013, 10, 581–601. [Google Scholar] [PubMed]
- Petrella, R.J.; Kennedy, E.; Overend, T.J. Geographic determinants of healthy lifestyle change in a community-based exercise prescription delivered in family practice. Environ. Health Insights 2008, 1, 51–62. [Google Scholar] [PubMed]
- Leslie, E.; Coffee, N.; Frank, L.; Owen, N.; Bauman, A.; Hugo, G. Walkability of local communities: Using geographic information systems to objectively assess relevant environmental attributes. Health Place 2007, 13, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Diez-Roux, A.V.; Nieto, F.J.; Muntaner, C.; Tyroler, H.A.; Comstock, G.W.; Shahar, E. Neighborhood environments and coronary heart disease: A multilevel analysis. Am. J. Epidemiol. 1997, 146, 48–63. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.H.; Lehman, A.; Hade, E.; Ferketich, A.K.; Gehlert, S.; Rauscher, G.H.; Abrams, J.; Bird, C.E. Challenges for multilevel health disparities research in a transdisciplinary environment. Am. J. Prev. Med. 2008, 35, S182–S192. [Google Scholar] [CrossRef] [PubMed]
- Ogedegbe, G.; Tobin, J.N.; Fernandez, S.; Gerin, W.; Diaz-Gloster, M.; Cassells, A.; Khalida, C.; Pickering, T.; Schoenthaler, A.; Ravenell, J. Counseling African Americans to control hypertension (CAATCH) trial: A multi-level intervention to improve blood pressure control in hypertensive blacks. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Gehlert, S.; Sohmer, D.; Sacks, T.; Mininger, C.; McClintock, M.; Olopade, O. Targeting health disparities: A model linking upstream determinants to downstream interventions. Health Aff. March 2008, 27, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Web GIS-App. Available online: http://t1t2.rtrn.net:8089/fips/login.php (accessed on 3 September 2015).
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Robinson, J.C.; Wyatt, S.B.; Hickson, D.; Gwinn, D.; Faruque, F.; Sims, M.; Sarpong, D.; Taylor, H.A. Methods for retrospective geocoding in population studies: The Jackson Heart Study. J. Urban Health 2010, 87, 136–150. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Adil, M.M.; Miller, Z.; Suri, M.; Rahim, B.; Gilani, S.I.; Gilani, W.I. Walk score and risk of stroke and stroke subtypes among town residents. J. Vasc. Interv. Neurol. 2014, 7, 26–29. [Google Scholar] [PubMed]
- Hirsch, J.A.; Moore, K.A.; Evenson, K.R.; Rodriguez, D.A.; Diez Roux, A.V. Walk Score® and Transit Score® and walking in the multi-ethnic study of atherosclerosis. Am. J. Prev. Med. 2013, 45, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Duncan, D.T.; Aldstadt, J.; Whalen, J.; Melly, S.J.; Gortmaker, S.L. Validation of walk score for estimating neighborhood walkability: An analysis of four U.S. metropolitan areas. Int. J. Environ. Res. Public Health 2011, 8, 4160–4179. [Google Scholar] [CrossRef] [PubMed]
- Tirapani Ldos, S.; Pinheiro, H.S.; Mansur, H.N.; Oliveira, D.D.; Huaira, R.M.; Huaira, C.C.; Grincenkov, F.R.; Bastos, M.G.; Fernandes, N.M. Impact of social vulnerability on the outcomes of predialysis chronic kidney disease patients in an interdisciplinary center. J. Bras. Nefrol. 2015, 37, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Reese, K. 2014/2019 Esri Diversity Index. An Esri® White Paper. Available online: http://downloads.esri.com/esri_content_doc/dbl/us/J10170%20US%20Diversity%20Index.pdf (accessed on 2 September 2014).
- Kline, P. The Handbook of Psychological Testing; Routledge: London, UK, 1993. [Google Scholar]
- Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences, 5th ed.; Houghton Mifflin: Boston, MA, USA, 2003. [Google Scholar]
- Sallis, J.F.; Slymen, D.J.; Conway, T.L.; Frank, L.D.; Saelens, B.E.; Cain, K.; Chapman, J.E. Income disparities in perceived neighborhood built and social environment attributes. Health Place 2011, 17, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Zick, C.D.; Smith, K.R.; Fan, J.X.; Brown, B.B.; Yamada, I.; Kowaleski-Jones, L. Running to the Store? The relationship between neighborhood environments and the risk of obesity. Soc. Sci. Med. 2009, 69, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Tuckel, P.; Milczarski, W. Walk Score (TM), Perceived Neighborhood Walkability, and walking in the USA. Am. J. Health Behav. 2015, 39, 242–256. [Google Scholar] [CrossRef] [PubMed]
- McGinn, A.P.; Evenson, K.R.; Herring, A.H.; Huston, S.L.; Rodriguez, D.A. Exploring associations between physical activity and perceived and objective measures of the built environment. J. Urban Health 2007, 84, 162–184. [Google Scholar] [CrossRef] [PubMed]
- Kirtland, K.A.; Porter, D.E.; Addy, C.L.; Neet, M.J.; Williams, J.E.; Sharpe, P.A.; Neff, L.J.; Kimsey, C.D., Jr.; Ainsworth, B.E. Environmental measures of physical activity supports: Perception versus reality. Am. J. Prev. Med. 2003, 24, 323–331. [Google Scholar] [CrossRef]
- Gebel, K.; Bauman, A.E.; Sugiyama, T.; Owen, N. Mismatch between perceived and objectively assessed neighborhood walkability attributes: Prospective relationships with walking and weight gain. Health Place 2011, 17, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, H.; Lee, J.E.; Hall, J.; Wagenaar, A.C.; Lee, H. Secondhand effects of students alcohol use reported by neighbors of colleges: The role of alcohol outlets. Soc. Sci. Med. 2002, 55, 425–435. [Google Scholar] [CrossRef]
- Code of Federal Regulations. Available online: http://pe.usps.gov/FRN/Group_E_PO_Box_Service_proposed.pdf (accessed on 5 September 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.E.; Sung, J.H.; Malouhi, M. Statistical Validation of a Web-Based GIS Application and Its Applicability to Cardiovascular-Related Studies. Int. J. Environ. Res. Public Health 2016, 13, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010002
Lee JE, Sung JH, Malouhi M. Statistical Validation of a Web-Based GIS Application and Its Applicability to Cardiovascular-Related Studies. International Journal of Environmental Research and Public Health. 2016; 13(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010002
Chicago/Turabian StyleLee, Jae Eun, Jung Hye Sung, and Mohamad Malouhi. 2016. "Statistical Validation of a Web-Based GIS Application and Its Applicability to Cardiovascular-Related Studies" International Journal of Environmental Research and Public Health 13, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010002